Burnout: The Occupational Phenomenon Eroding Modern Work
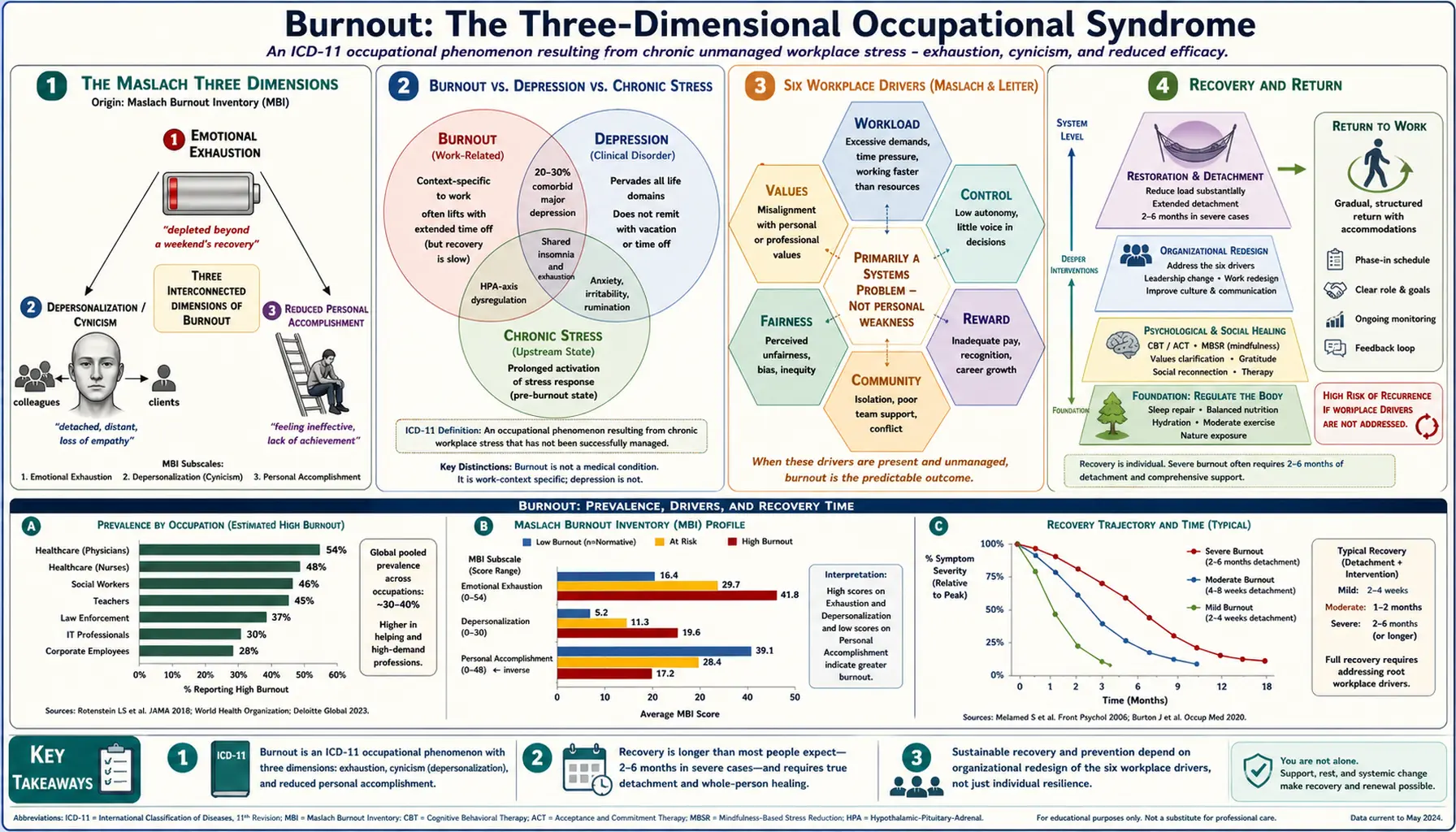
Burnout was formally recognized by the World Health Organization in 2019 as an occupational phenomenon in the ICD-11 — not a medical diagnosis per se, but a syndrome resulting from chronic workplace stress that has not been successfully managed. Its three core dimensions are exhaustion, cynicism or depersonalization, and reduced professional efficacy. Rates are particularly high in healthcare (especially nursing and physicians), teaching, first responders, and high-autonomy knowledge work, and they rose sharply during the pandemic and have not fully returned to baseline.
Table of Contents
- What Burnout Is
- Burnout vs Depression vs Chronic Stress
- Signs and Symptoms
- Systemic Drivers
- Measuring Burnout
- Individual Recovery Strategies
- Organizational Interventions
- Returning to Work
- Research Papers
- Connections
- Featured Videos
What Burnout Is
The Maslach Burnout Inventory, developed by Christina Maslach in the 1970s, defined burnout along three dimensions still used today:
- Emotional exhaustion. Feeling drained, depleted, beyond recovery by a weekend or vacation.
- Depersonalization / cynicism. Detachment, negativity, reduced empathy, cynicism about one’s work or clients.
- Reduced personal accomplishment. Feeling ineffective, diminished sense of meaning.
Burnout vs Depression vs Chronic Stress
- Burnout is context-specific (primarily work); symptoms typically lift during extended time away (though recovery is slower than expected).
- Depression pervades all life domains and does not remit with vacation.
- Chronic stress is the upstream state; burnout is what happens when chronic stress exceeds adaptive capacity over months to years.
The three overlap substantially. About 20–30% of burnout cases meet formal criteria for major depression, and the inverse is common too.
Signs and Symptoms
- Chronic fatigue not relieved by sleep
- Insomnia or fragmented sleep despite exhaustion
- Dread approaching work days; Sunday-evening anxiety
- Cognitive difficulties — focus, memory, decision-making
- Physical symptoms: headaches, GI complaints, muscle tension
- Cynicism about colleagues, clients, or mission
- Emotional dysregulation — short temper, tearfulness
- Withdrawal from work relationships and personal relationships
- Reduced productivity and quality
- Increased mistakes and near-misses
- Substance use for stress relief
- Feeling “hollow,” “numb,” or “flat”
Systemic Drivers
Research consistently identifies six workplace factors that drive burnout:
- Workload. Sustained demand exceeding capacity.
- Control. Lack of autonomy over how, when, where work gets done.
- Reward. Insufficient recognition, compensation, or intrinsic satisfaction.
- Community. Broken or toxic workplace relationships.
- Fairness. Perceived or actual injustice in decisions, treatment, or compensation.
- Values. Conflict between one’s values and organizational practices.
Individual traits modulate risk — perfectionism, high agreeableness, strong caregiving motivation all increase susceptibility — but the evidence overwhelmingly indicates burnout is primarily a systems problem, not a personal weakness. This matters because most workplace “wellness” programs target individuals while leaving the organizational drivers untouched.
Measuring Burnout
- Maslach Burnout Inventory (MBI) — the gold standard, 22 items across the three dimensions.
- Oldenburg Burnout Inventory (OLBI) — shorter alternative.
- Copenhagen Burnout Inventory (CBI) — separates personal, work, and client burnout.
Individual Recovery Strategies
- Reduce load. Taking work off the plate is the single most effective intervention if achievable.
- Recovery time requires longer and more complete detachment than most people assume. A single weekend is insufficient once burnout is established.
- Sleep hygiene — burnout recovery requires sleep repair.
- Physical activity at moderate intensity — cardiovascular and mood benefit without further depleting.
- Nature exposure — 120 minutes per week of nature time has measurable effect on stress markers.
- Therapy — cognitive behavioral therapy, acceptance and commitment therapy.
- Social connection — ring-fenced relationships outside work.
- Mindfulness-based stress reduction (MBSR) — 8-week programs have trial evidence.
- Creative and meaningful activities outside work domain.
- Treatment of comorbid depression or anxiety when present.
- In severe cases, medical leave — often 2 to 6 months is required rather than the 2 weeks commonly prescribed.
Organizational Interventions
- Adjust workload and staffing ratios.
- Increase autonomy and decision-latitude.
- Improve management quality through training and accountability.
- Reduce administrative burden (a major driver of healthcare and teaching burnout).
- Create genuine psychological safety and feedback channels.
- Fair compensation and recognition.
- Transparent and fair processes.
- Support for mission alignment between values and practices.
Returning to Work
Gradual, structured return after a burnout leave is more successful than sudden full return. Workplace adjustments — at least temporarily — are frequently necessary. Without modification of the original drivers, recurrence is common. In many severe cases, a role or employer change is ultimately the most effective intervention.
Research Papers
The PubMed topic searches below return up-to-date peer-reviewed literature for the subjects covered on this page.
- PubMed: burnout occupational
- PubMed: burnout Maslach inventory
- PubMed: physician burnout
- PubMed: burnout depression
- PubMed: burnout cortisol HPA
- PubMed: burnout mindfulness
- PubMed: burnout cognitive behavioral therapy
- PubMed: burnout organizational intervention
- PubMed: burnout healthcare workers
- PubMed: burnout teachers
- PubMed: burnout sleep
- PubMed: burnout recovery rest
Connections
- Depression
- Anxiety
- Insomnia
- Loneliness
- Grief
- PTSD
- Sleep Hygiene
- Stress Management
- Natural Anxiety Relief
- Breathwork
- Cortisol Test
- ME/CFS
- Fatigue
- Insomnia Symptom
- Rhodiola Rosea
- Adrenal Fatigue
- Vitamin B5
- Sleep, Stress & Cortisol in Insulin Resistance