Sinusitis
A comprehensive guide to understanding and managing sinusitis from a Naturopathic Doctor perspective, covering conventional treatments and evidence-based natural approaches for acute, chronic, and recurrent sinus inflammation.
Table of Contents
- What Is Sinusitis?
- Anatomy of the Sinuses
- Causes of Sinusitis
- Risk Factors
- Symptoms
- Conventional Treatment
- Natural and Naturopathic Approaches
- Nasal Irrigation and Steam Inhalation
- Essential Oils for Sinus Support
- Elimination of Dairy and Food Triggers
- Gut Health and Sinus Connection
- Mold Exposure as a Hidden Cause
- Cautions and When to Seek Medical Attention
- References & Research
- Featured Videos
What Is Sinusitis?
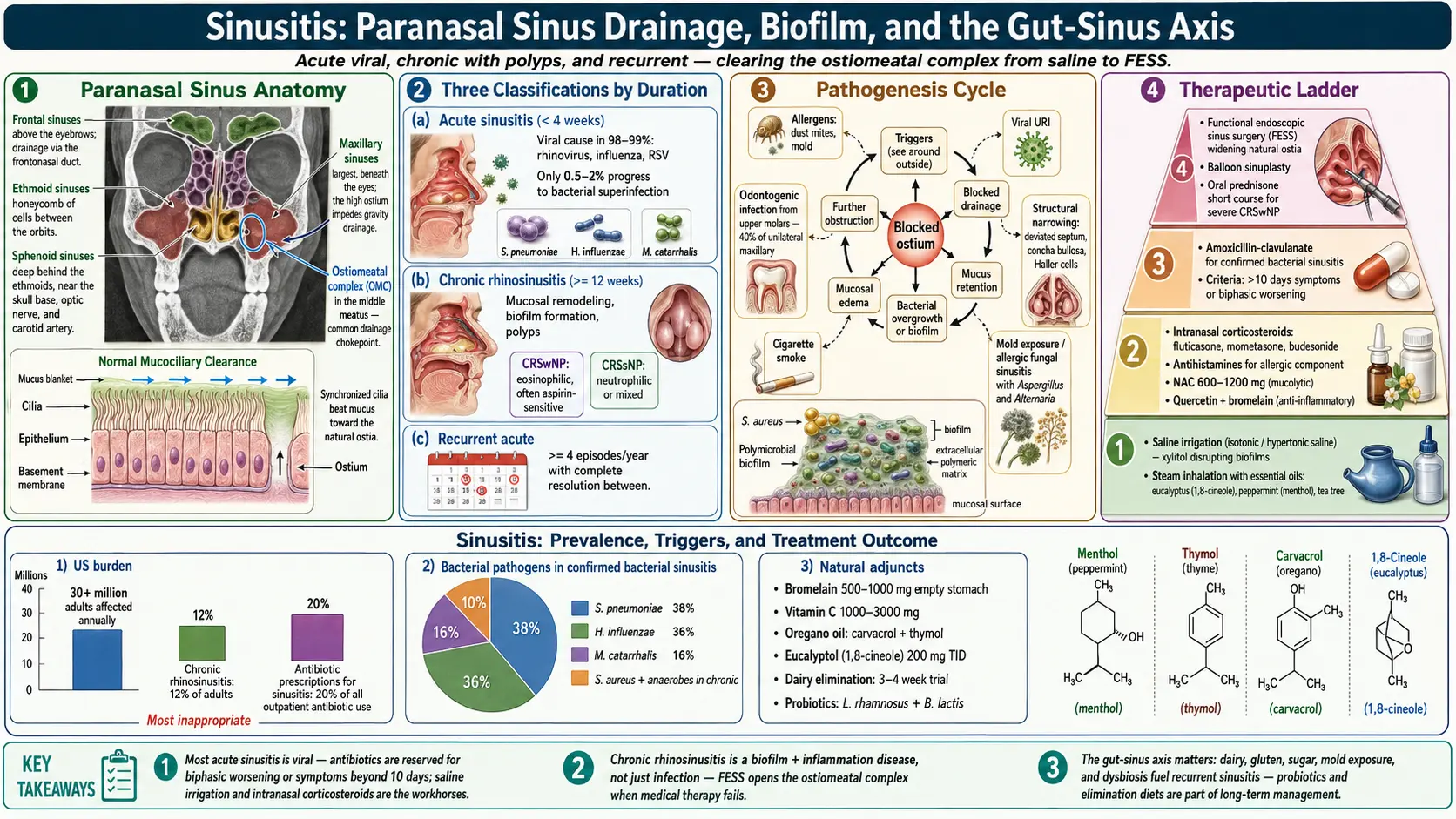
Sinusitis, also called rhinosinusitis, is inflammation of the mucous membranes lining the paranasal sinuses. It is one of the most common health conditions worldwide, affecting over 30 million adults annually in the United States alone. Sinusitis is classified by duration and pattern:
Acute Sinusitis
Acute sinusitis lasts fewer than 4 weeks and is most often triggered by a viral upper respiratory infection (the common cold). Symptoms typically include nasal congestion, purulent or discolored nasal discharge, facial pain or pressure, and reduced sense of smell. Most cases resolve on their own within 7 to 10 days. Bacterial superinfection occurs in only 0.5 to 2 percent of viral cases and should be suspected when symptoms worsen after initial improvement or persist beyond 10 days without resolution.
Chronic Sinusitis
Chronic sinusitis is defined by symptoms lasting 12 weeks or longer despite treatment attempts. It is a fundamentally different condition from acute sinusitis, driven by persistent inflammation, mucosal remodeling, biofilm formation, and often an underlying immune or allergic component rather than simple infection. Chronic sinusitis with nasal polyps represents a distinct subtype associated with eosinophilic inflammation and aspirin sensitivity.
Recurrent Acute Sinusitis
Recurrent acute sinusitis is characterized by four or more episodes per year, each lasting fewer than 4 weeks, with complete resolution between episodes. This pattern suggests an underlying predisposing factor that should be identified and addressed.
Anatomy of the Sinuses
Understanding sinus anatomy helps explain why sinusitis occurs and why drainage is central to treatment.
The paranasal sinuses are four pairs of air-filled cavities within the facial bones:
- Maxillary sinuses — the largest sinuses, located in the cheekbones below the eyes; most commonly affected in sinusitis because their drainage opening (ostium) is located high on the medial wall, making gravity-dependent drainage difficult
- Frontal sinuses — located in the forehead above the eyebrows; drain through the narrow frontonasal duct into the middle meatus
- Ethmoid sinuses — a honeycomb of small air cells between the eyes; their thin walls are adjacent to the orbits, making orbital complications a concern in severe ethmoid sinusitis
- Sphenoid sinuses — deep sinuses behind the ethmoids near the base of the skull; infection here is less common but potentially more dangerous due to proximity to the brain, optic nerves, and carotid arteries
All sinuses are lined with ciliated pseudostratified columnar epithelium that produces mucus. The cilia beat in a coordinated wave to sweep mucus and trapped particles toward the natural ostia and into the nasal cavity. Any condition that causes mucosal swelling, impairs ciliary function, or increases mucus viscosity can obstruct drainage and set the stage for sinusitis.
Causes of Sinusitis
Viral
Viruses cause the vast majority of acute sinusitis episodes. Rhinovirus is the most common culprit, followed by influenza, parainfluenza, and respiratory syncytial virus. Viral infection causes mucosal edema that obstructs sinus ostia, traps mucus, and impairs ciliary clearance. Most viral sinusitis resolves within 7 to 10 days.
Bacterial
Bacterial sinusitis typically develops as a secondary complication of viral sinusitis. The most common pathogens are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. In chronic sinusitis, Staphylococcus aureus, anaerobic bacteria, and polymicrobial biofilms play a more prominent role.
Fungal
Fungal sinusitis takes several forms. Allergic fungal sinusitis is a hypersensitivity reaction to fungal elements (commonly Aspergillus or Alternaria) trapped in thick mucus, and is a significant cause of chronic sinusitis with nasal polyps. Fungal ball (mycetoma) is a non-invasive mass of fungal hyphae, usually in the maxillary sinus. Invasive fungal sinusitis is a life-threatening emergency occurring in immunocompromised patients.
Allergic
Allergic rhinitis is one of the strongest risk factors for sinusitis. Allergen-triggered inflammation causes chronic mucosal swelling and mucus hypersecretion that predispose to sinus obstruction. Common aeroallergens include dust mites, mold spores, pet dander, and pollens.
Risk Factors
- Allergies — allergic rhinitis creates chronic mucosal inflammation that obstructs sinus drainage; both seasonal and perennial allergies increase sinusitis risk
- Structural abnormalities — deviated nasal septum, concha bullosa (pneumatized middle turbinate), paradoxical middle turbinate, and Haller cells can narrow the ostiomeatal complex and impair drainage
- Nasal polyps — benign growths arising from inflamed mucosa that physically obstruct sinus ostia
- Immune deficiency — IgA deficiency, common variable immunodeficiency, and other immune disorders predispose to recurrent and chronic sinusitis; HIV/AIDS increases risk of opportunistic fungal sinusitis
- Dental infections — the roots of the upper premolars and molars are separated from the maxillary sinus floor by only a thin layer of bone; periapical abscesses, periodontal disease, or complications from dental procedures can cause odontogenic sinusitis, which accounts for up to 40 percent of unilateral maxillary sinusitis
- Ciliary dyskinesia — primary ciliary dyskinesia and secondary impairment from smoking, pollution, or viral damage
- Environmental irritants — cigarette smoke, air pollution, chlorine, and occupational chemical exposure
- GERD — laryngopharyngeal reflux may contribute to chronic nasal and sinus inflammation
- Swimming and diving — chlorinated water and barotrauma can irritate sinus mucosa
Symptoms
The cardinal symptoms of sinusitis include:
- Nasal congestion and obstruction — difficulty breathing through one or both nostrils
- Nasal discharge — anterior (from the nose) or posterior (postnasal drip); may be clear, yellow, green, or blood-tinged
- Facial pain and pressure — location depends on which sinuses are affected: cheek and upper teeth (maxillary), forehead (frontal), between the eyes (ethmoid), or top of the head and behind the eyes (sphenoid)
- Reduced or lost sense of smell (hyposmia or anosmia)
- Headache — often worse with bending forward
- Ear fullness or pressure — due to eustachian tube dysfunction
- Cough — particularly at night from postnasal drip
- Fatigue and malaise
- Bad breath (halitosis) — from stagnant infected mucus
- Dental pain — upper teeth may ache due to maxillary sinus floor inflammation
Conventional Treatment
Antibiotics
Antibiotics are indicated only for confirmed or strongly suspected bacterial sinusitis (symptoms lasting more than 10 days without improvement, or worsening after initial improvement). Amoxicillin-clavulanate is the first-line antibiotic. For penicillin-allergic patients, doxycycline or a respiratory fluoroquinolone may be used. Overuse of antibiotics for viral sinusitis contributes to antibiotic resistance and disrupts the beneficial microbiome.
Corticosteroids
Intranasal corticosteroid sprays (fluticasone, mometasone, budesonide) are a mainstay of both acute and chronic sinusitis treatment. They reduce mucosal inflammation and edema, improving sinus drainage and symptom relief. Short courses of oral corticosteroids (prednisone) may be used for severe acute sinusitis or chronic sinusitis with nasal polyps.
Decongestants
Topical decongestants (oxymetazoline) provide rapid but temporary relief by constricting blood vessels in the nasal mucosa. Use must be limited to 3 days to avoid rebound congestion (rhinitis medicamentosa). Oral decongestants (pseudoephedrine) may be used for longer periods but raise blood pressure.
Surgery
Functional endoscopic sinus surgery (FESS) is considered when medical therapy fails after adequate trials. FESS widens the natural sinus ostia, removes polyps and diseased tissue, and restores normal drainage pathways. It is performed endoscopically through the nostrils with no external incisions. Balloon sinuplasty is a less invasive alternative for select patients, using an inflatable catheter to dilate blocked ostia.
Natural and Naturopathic Approaches
From a Naturopathic Doctor perspective, treating sinusitis involves clearing infection, reducing inflammation, restoring mucosal health, addressing underlying predisposing factors, and supporting immune function. The following natural agents have evidence supporting their use.
N-Acetylcysteine (NAC) as a Mucolytic
NAC breaks disulfide bonds in mucus glycoproteins, reducing viscosity and promoting drainage. It also replenishes intracellular glutathione, supporting antioxidant defense and immune function. Dosing of 600 to 1200 mg daily is typical. NAC can be taken orally or used in nebulized form for more direct sinus application.
Quercetin
Quercetin is a flavonoid with potent anti-inflammatory and mast cell-stabilizing properties. It inhibits histamine release and downregulates the production of pro-inflammatory cytokines and leukotrienes. Doses of 500 to 1000 mg twice daily, taken between meals, can help reduce allergic and inflammatory components of sinusitis. Quercetin combined with bromelain enhances absorption and efficacy.
Bromelain
Bromelain, a proteolytic enzyme from pineapple stems, reduces nasal mucosal inflammation and edema, thins mucus, and may have mild antimicrobial activity. Clinical trials in sinusitis patients have shown faster symptom resolution compared to placebo. The typical dose is 500 to 1000 mg daily on an empty stomach. Germany's Commission E has approved bromelain for the treatment of acute sinusitis.
Vitamin C
Vitamin C supports immune function through multiple mechanisms: enhancing neutrophil chemotaxis and phagocytosis, supporting epithelial barrier integrity, and providing antioxidant protection. Doses of 1000 to 3000 mg daily in divided doses are commonly recommended during acute sinusitis. Buffered or liposomal forms are gentler on the stomach at higher doses.
Oregano Oil
Oil of oregano (Origanum vulgare) contains carvacrol and thymol, which have broad-spectrum antimicrobial activity against bacteria, fungi, and some viruses in laboratory studies. It can be taken as enteric-coated capsules (150 to 200 mg of a standardized extract two to three times daily) or used in steam inhalation by adding two to three drops to a bowl of hot water. Direct nasal application of undiluted oregano oil should be avoided due to mucosal irritation.
Garlic
Garlic (Allium sativum) contains allicin and other sulfur compounds with antimicrobial, antiviral, and immune-enhancing properties. Fresh crushed raw garlic provides the highest allicin content. Aged garlic extract (600 to 1200 mg daily) is better tolerated and still provides immune support. Garlic may be particularly beneficial for preventing secondary bacterial infection during viral sinusitis.
Goldenseal and Berberine
Goldenseal (Hydrastis canadensis) and its primary alkaloid berberine have antimicrobial activity against common sinusitis pathogens including Staphylococcus aureus and Streptococcus species. Berberine also has anti-inflammatory and immune-modulating effects. Goldenseal can be taken as capsules (500 to 1000 mg three times daily of the dried root) or as a tincture. Berberine-containing herbs should be used for limited courses (2 to 3 weeks) rather than continuously. Goldenseal is an endangered plant; sustainably sourced or cultivated products or Oregon grape root (Mahonia aquifolium) as an alternative berberine source should be preferred.
Nasal Irrigation and Steam Inhalation
Neti Pot and Saline Irrigation
Nasal saline irrigation is one of the most effective and well-supported therapies for sinusitis. It physically flushes mucus, allergens, bacteria, and inflammatory mediators from the nasal passages and sinuses, reduces mucosal edema, and improves ciliary function.
- Use a neti pot, squeeze bottle, or pulsating irrigation device with isotonic or hypertonic saline
- The saline solution should be made with distilled, sterile, or previously boiled water to eliminate the risk of amoebic infection
- Add one-quarter to one-half teaspoon of non-iodized salt and a pinch of baking soda per 8 ounces of water
- Irrigate each nostril once to twice daily during active sinusitis
Xylitol Nasal Rinse
Adding xylitol to saline irrigation provides additional benefit. Xylitol disrupts bacterial biofilms, inhibits bacterial adherence to mucosal surfaces, and has osmotic properties that thin mucus. Use one teaspoon of xylitol dissolved in the standard saline solution. Commercial xylitol nasal sprays are also available.
Steam Inhalation
Inhaling warm, moist steam helps hydrate and loosen thick mucus, soothe inflamed mucosa, and promote sinus drainage. Lean over a bowl of steaming water with a towel draped over the head for 10 to 15 minutes, two to three times daily. Adding essential oils such as eucalyptus, peppermint, or tea tree enhances the decongestant and antimicrobial effect. A warm, wet washcloth applied to the face can also provide relief between steam sessions.
Essential Oils for Sinus Support
Several essential oils have properties that support sinus health when used appropriately.
Eucalyptus Oil
Eucalyptus (Eucalyptus globulus or E. radiata) contains 1,8-cineole (eucalyptol), which has mucolytic, anti-inflammatory, and antimicrobial properties. A randomized controlled trial demonstrated that oral 1,8-cineole capsules (200 mg three times daily) significantly improved symptoms in acute sinusitis. Eucalyptus oil can also be used in steam inhalation (3 to 5 drops in a bowl of hot water) or applied diluted to the chest and temples.
Peppermint Oil
Peppermint (Mentha piperita) contains menthol, which activates cold receptors in the nasal mucosa, creating a sensation of improved airflow even before physical decongestion occurs. Menthol also has mild analgesic and anti-inflammatory properties. Use in steam inhalation or apply diluted (with a carrier oil) to the forehead and under the nose. Avoid direct contact with eyes and mucous membranes.
Tea Tree Oil
Tea tree (Melaleuca alternifolia) has broad-spectrum antimicrobial activity including against Staphylococcus aureus and fungal organisms relevant to chronic sinusitis. It can be added to steam inhalation but should never be ingested or applied undiluted to nasal passages.
Safety note: Essential oils are potent and concentrated. Always dilute before topical application. Do not instill essential oils directly into the nose. Keep away from young children. Discontinue use if irritation occurs.
Elimination of Dairy and Food Triggers
Dietary factors can significantly influence sinus health, and identifying food triggers is an important part of the naturopathic approach to chronic and recurrent sinusitis.
Dairy
Dairy products are the most commonly implicated dietary trigger for sinus congestion. While the belief that dairy increases mucus production is debated in research, many patients report significant improvement after eliminating dairy. Proposed mechanisms include:
- Casein protein triggering an inflammatory immune response in sensitive individuals
- A1 beta-casein (from conventional cow's milk) generating beta-casomorphin-7, which may stimulate mucus secretion from respiratory glands
- Undiagnosed dairy allergy or intolerance contributing to chronic inflammation
A strict dairy elimination trial of 3 to 4 weeks, followed by systematic reintroduction, is the most reliable way to determine individual sensitivity.
Other Food Triggers
- Gluten — wheat and other gluten-containing grains may promote inflammation in sensitive individuals, even without celiac disease
- Refined sugar — suppresses immune function and promotes inflammatory pathways
- Alcohol — causes nasal congestion through vasodilation and histamine release; beer and wine contain additional histamine and sulfites
- Histamine-rich foods — aged cheeses, fermented foods, cured meats, and vinegar may worsen symptoms in patients with histamine intolerance
- Food additives — sulfites, MSG, and artificial colorings may trigger nasal symptoms in sensitive individuals
An anti-inflammatory diet emphasizing vegetables, fruits, omega-3 fatty acids, and whole foods while minimizing processed foods, sugar, and common allergens provides a supportive nutritional foundation for sinus health.
Gut Health and Sinus Connection
Emerging research highlights the interconnection between gut health and respiratory mucosal immunity, often termed the gut-lung axis. This concept is directly relevant to chronic and recurrent sinusitis.
- Mucosal immune system — the gut-associated lymphoid tissue (GALT) and nasal-associated lymphoid tissue (NALT) are part of a common mucosal immune system; immune cells educated in the gut migrate to and protect respiratory mucosa
- Microbiome diversity — a diverse gut microbiome supports balanced immune function; dysbiosis (from antibiotics, poor diet, or stress) skews the immune response toward excessive inflammation and allergic reactivity
- Antibiotic disruption — repeated courses of antibiotics for sinusitis can deplete beneficial gut and nasal bacteria, creating a cycle of recurrent infection; probiotic supplementation during and after antibiotic use is essential
- Probiotics for sinusitis — Lactobacillus rhamnosus, Lactobacillus paracasei, and Bifidobacterium lactis strains have shown benefit for reducing allergic rhinitis symptoms and upper respiratory infections in clinical trials
- Intestinal permeability — increased gut permeability (leaky gut) allows food antigens and bacterial endotoxins to enter the bloodstream, promoting systemic inflammation that can manifest as chronic sinus inflammation
- Gut healing — addressing gut health through elimination of trigger foods, probiotic and prebiotic supplementation, glutamine, zinc carnosine, and anti-inflammatory herbs can have a profound indirect benefit on chronic sinusitis
Mold Exposure as a Hidden Cause
Mold exposure is an underrecognized cause of chronic sinusitis that should be investigated in any patient with persistent or treatment-resistant symptoms.
How Mold Causes Sinusitis
- Allergic response — mold spores are potent aeroallergens that trigger IgE-mediated inflammation in the nasal and sinus mucosa
- Fungal colonization — inhaled mold spores can colonize the warm, moist environment of the sinuses, especially in the setting of pre-existing mucosal damage or immune compromise
- Mycotoxin exposure — some mold species produce toxic secondary metabolites (mycotoxins) including aflatoxins, ochratoxin, and trichothecenes that can impair immune function, damage mucosal barriers, and promote chronic inflammation
- Inflammatory cascade — mold exposure can activate the innate immune system and drive a chronic inflammatory response even at exposure levels below those that trigger classic allergic symptoms
Identifying Mold Exposure
- Inspect the home and workplace for visible mold, water damage, musty odors, and humidity issues
- Common problem areas include bathrooms, basements, HVAC systems, window sills, and behind walls with water damage
- Professional mold testing (air sampling, surface sampling) can quantify exposure levels
- Urine mycotoxin testing can help determine whether a patient has significant mycotoxin burden
Addressing Mold-Related Sinusitis
- Professional mold remediation of the home environment is the essential first step
- HEPA air purifiers reduce airborne mold spore counts
- Maintain indoor humidity below 50 percent
- Nasal irrigation with antifungal agents (dilute povidone-iodine or colloidal silver under practitioner guidance) may help clear fungal colonization
- Systemic support with glutathione, NAC, activated charcoal, and cholestyramine may assist mycotoxin clearance
Cautions and When to Seek Medical Attention
While most sinusitis can be managed conservatively, certain situations require prompt medical evaluation:
- High fever (above 102 degrees F or 39 degrees C) with facial pain — may indicate severe bacterial infection
- Periorbital swelling, redness, or vision changes — orbital cellulitis is a serious complication of ethmoid sinusitis requiring urgent treatment
- Severe headache, stiff neck, or altered mental status — may indicate intracranial complications such as meningitis, epidural abscess, or cavernous sinus thrombosis
- Symptoms lasting beyond 10 days without improvement — bacterial sinusitis likely requiring antibiotic therapy
- Recurrent episodes (four or more per year) — warrant investigation for underlying allergies, immune deficiency, structural abnormalities, or dental pathology
- Unilateral symptoms with bloody nasal discharge — require evaluation to rule out dental infection, fungal disease, or rarely, sinonasal malignancy
Important notes on natural treatments:
- Always use distilled or previously boiled water for nasal irrigation to prevent amoebic infection
- Essential oils should never be instilled directly into the nasal passages undiluted
- Goldenseal and berberine-containing herbs should not be used during pregnancy
- High-dose vitamin C may cause gastrointestinal discomfort; reduce dose if diarrhea occurs
- Bromelain may increase bleeding risk in patients on anticoagulant medications
- Natural approaches should complement, not replace, appropriate medical care for severe or complicated sinusitis
- Work with a qualified Naturopathic Doctor or integrative practitioner to develop an individualized treatment plan
14. References & Research
Historical Background
Sinusitis was recognized in ancient medicine, with Hippocrates describing nasal discharge and facial pain around 400 BCE. The paranasal sinuses were first anatomically described by Leonardo da Vinci and later detailed by Nathaniel Highmore in 1651, after whom the maxillary sinus (antrum of Highmore) is named. Modern endoscopic sinus surgery was pioneered by Messerklinger and Stammberger in Austria during the 1970s and 1980s, and David Kennedy introduced functional endoscopic sinus surgery (FESS) to North America in the late 1980s.
Key Research Papers
- Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 Suppl):S1-S39.
- Fokkens WJ, Lund VJ, Hopkins C, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020 (EPOS 2020). Rhinology. 2020;58(Suppl S29):1-464.
- Meltzer EO, Hamilos DL. Rhinosinusitis diagnosis and management for the clinician: a synopsis of recent consensus guidelines. Mayo Clin Proc. 2011;86(5):427-443.
- Chong LY, Head K, Hopkins C, et al. Saline irrigation for allergic rhinitis. Cochrane Database Syst Rev. 2016;(4):CD012597.
- Ponikau JU, Sherris DA, Kern EB, et al. The diagnosis and incidence of allergic fungal sinusitis. Mayo Clin Proc. 1999;74(9):877-884.
- Harvey R, Hannan SA, Badia L, Scadding G. Nasal saline irrigations for the symptoms of chronic rhinosinusitis. Cochrane Database Syst Rev. 2007;(3):CD006394.
- Desrosiers MY, Kilty SJ. Treatment alternatives for chronic rhinosinusitis persisting after ESS: what to do when debridement, maximal medical therapy, irrigation, and topical corticosteroids fail. Rhinology. 2008;46(1):3-14.
- Cazzola M, Calzetta L, Page CP, et al. Influence of N-acetylcysteine on chronic bronchitis or COPD exacerbations: a meta-analysis. Eur Respir Rev. 2015;24(137):451-461.
- Bachert C, Zhang L, Gevaert P. Current and future treatment options for adult chronic rhinosinusitis: focus on nasal polyposis. J Allergy Clin Immunol. 2015;136(6):1431-1440.
- Laidlaw TM, Mullol J, Woessner KM, et al. Chronic rhinosinusitis with nasal polyps and asthma. J Allergy Clin Immunol Pract. 2021;9(3):1133-1141.
- Guo R, Canter PH, Ernst E. Herbal medicines for the treatment of rhinosinusitis: a systematic review. Otolaryngol Head Neck Surg. 2006;135(4):496-506.
- Ahovuo-Saloranta A, Rautakorpi UM, Borisenko OV, et al. Antibiotics for acute maxillary sinusitis in adults. Cochrane Database Syst Rev. 2014;(2):CD000243.
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Sinusitis. Each link opens a live PubMed query so you always see the most recent publications.
- Chronic rhinosinusitis review
- Acute bacterial sinusitis diagnosis
- Saline nasal irrigation sinusitis
- Intranasal corticosteroid rhinosinusitis
- Dupilumab chronic rhinosinusitis nasal polyps
- Fungal sinusitis allergic
- Endoscopic sinus surgery outcomes
- Sinusitis antibiotic stewardship
- Xylitol nasal spray sinusitis
- Eucalyptus essential oil sinus
- Quercetin allergic rhinitis sinus
Connections
- Oregano
- Vitamin C
- Garlic
- Berberine
- Eucalyptus
- Quercetin
- Omega-3 Fatty Acids
- Probiotics
- Gut Healing
- Anti-Inflammatory Diet
- Thyme
- Oral Microbiome
- Immune Boosting
- Vitamin D3
- Goldenseal
- Allergies
- Peppermint
- NAC
- Hearing Loss
- Common Cold
- Strep Throat
- Ear Infections
- Trigeminal Neuralgia