Vitamin D3 for Autoimmune Disease
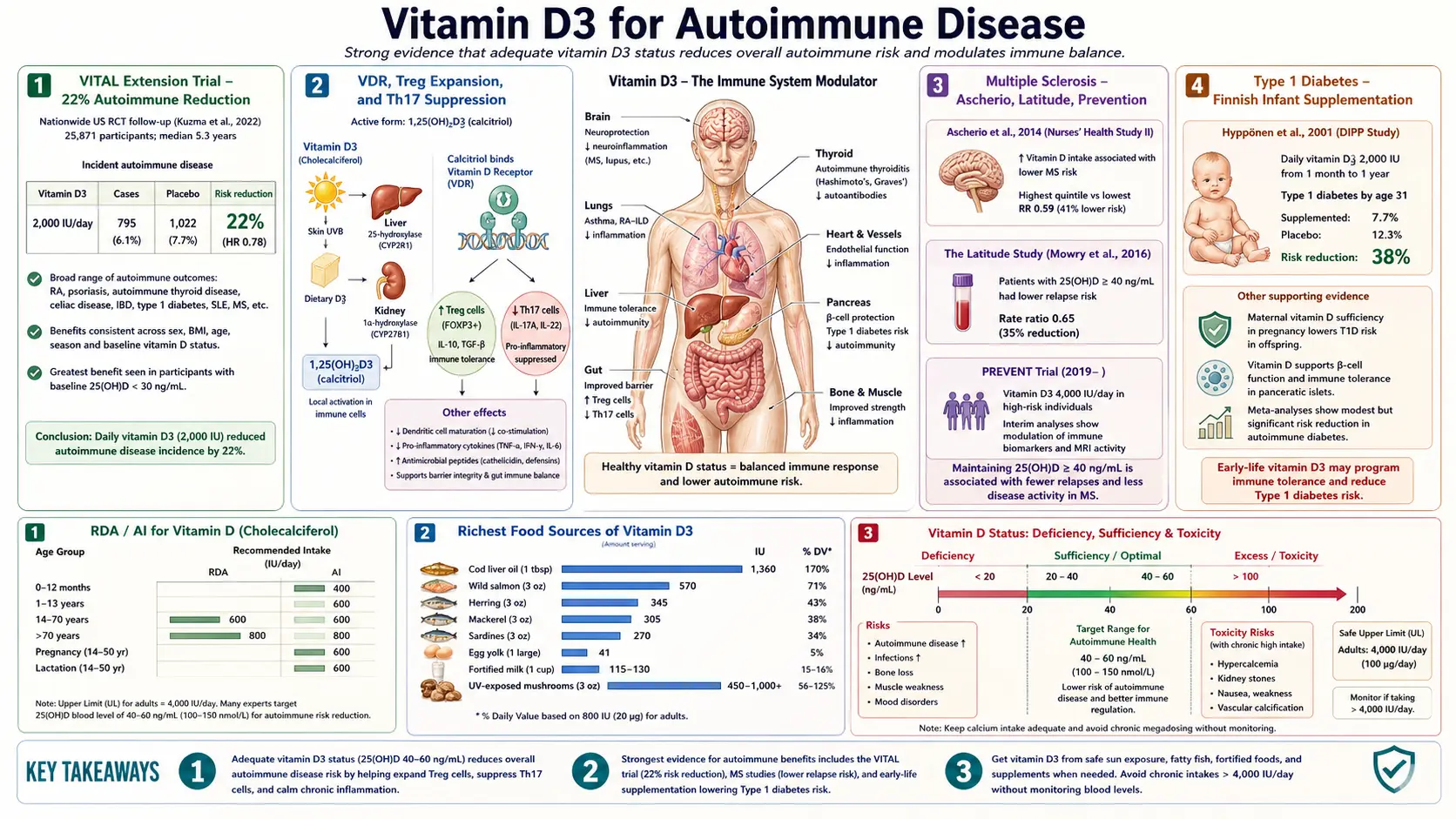
Vitamin D3 has emerged as one of the most important modifiable risk factors for autoimmune disease — the family of disorders in which the immune system attacks the body's own tissues. The landmark 2022 VITAL extension trial demonstrated a 22% reduction in incident autoimmune disease in adults receiving 2,000 IU/day of vitamin D3 over 5 years. Underlying this finding is a clear mechanism: calcitriol acts on naive T-cells and dendritic cells to suppress pathogenic Th17 differentiation, expand regulatory T-cell (Treg) populations via FoxP3 induction, and tilt the immune system toward tolerance rather than attack. The geographic latitude gradient seen in multiple sclerosis (and most other autoimmune conditions) mirrors the gradient in UVB-driven D3 synthesis. Specific evidence supports protective and therapeutic effects in MS, type 1 diabetes (especially when supplemented in infancy), inflammatory bowel disease, Hashimoto's thyroiditis, psoriasis, lupus, and rheumatoid arthritis. At the most aggressive end of the dose spectrum, the Coimbra Protocol uses very-high-dose vitamin D under strict specialist supervision and calcium-restricted diet for treatment-resistant autoimmune conditions.
Table of Contents
- The VITAL Extension Trial — 22% Autoimmune Reduction
- VDR, Treg Expansion, and Th17 Suppression
- Multiple Sclerosis — Ascherio, Latitude, Prevention
- Type 1 Diabetes — Finnish Infant Supplementation
- Inflammatory Bowel Disease (Crohn's, UC)
- Hashimoto's Thyroiditis
- Psoriasis (Topical and Systemic)
- Lupus and Rheumatoid Arthritis
- The Coimbra Protocol (High-Dose Supervised)
- Target 25(OH)D for Autoimmune Outcomes
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The VITAL Extension Trial — 22% Autoimmune Reduction
The VITAL trial (VITamin D and OmegA-3 TriaL) was the largest randomized trial of vitamin D supplementation ever conducted. 25,871 American adults aged 50+ were randomized in a 2×2 factorial design to vitamin D3 2,000 IU/day vs placebo and to fish oil 1 gram/day vs placebo, with a median follow-up of 5.3 years. The primary outcomes were cancer and cardiovascular disease.
In 2022, Hahn and colleagues published the pre-specified autoimmune disease secondary analysis in BMJ. The result was striking:
- Vitamin D3 alone: 22% reduction in incident autoimmune disease (HR 0.78, 95% CI 0.61-0.99)
- Vitamin D3 + fish oil: 30% reduction in incident autoimmune disease
- Fish oil alone: 15% reduction (not statistically significant)
- The effect grew over time — protection became more pronounced after the first 2 years of supplementation, suggesting a cumulative effect of sustained vitamin D sufficiency
- The benefit was statistically significant for the composite autoimmune endpoint despite the relatively modest 2,000 IU/day dose (which only modestly raised 25(OH)D in many participants)
The autoimmune endpoints in VITAL included rheumatoid arthritis, psoriasis, autoimmune thyroid disease, polymyalgia rheumatica, and a smaller number of other conditions. The trial was not powered to detect effects within individual diseases, but the composite finding has substantial clinical implications: vitamin D supplementation at a modest dose of 2,000 IU/day, in a generally well-nourished older American population, prevented roughly 1 in 5 incident autoimmune diagnoses over 5 years.
The clinical translation is straightforward: routine vitamin D supplementation should be considered for primary prevention of autoimmune disease, particularly in individuals with a family history of autoimmunity or with risk factors for vitamin D deficiency (high latitude, dark skin, obesity, indoor occupation).
VDR, Treg Expansion, and Th17 Suppression
The mechanistic basis for vitamin D's anti-autoimmune effect is now well-characterized at the molecular level. Calcitriol acts on three cell types in the autoimmune cascade:
Dendritic cells
Dendritic cells (DCs) are the antigen-presenting cells that determine whether a naive T-cell encountering a particular antigen will be activated (mount an immune response) or tolerized (learn to ignore it). Calcitriol shifts DCs toward a tolerogenic phenotype — reduced expression of MHC class II and costimulatory molecules (CD80, CD86), reduced IL-12 production, and increased IL-10 production. Tolerogenic DCs present self-antigens to T-cells in a way that promotes tolerance rather than autoreactive attack.
Naive T-cells — Th17 suppression
Th17 cells are the pathogenic T-cell subset that drives most autoimmune tissue damage. They produce IL-17, which recruits neutrophils, induces tissue inflammation, and damages target organs. Calcitriol directly suppresses Th17 differentiation by:
- Inhibiting RORγt, the master transcription factor for Th17 development
- Suppressing IL-17 production from already-differentiated Th17 cells
- Reducing the Th17-supporting cytokine environment (IL-6, IL-23)
Naive T-cells — Treg expansion
Regulatory T-cells (Tregs) are the immune system's brake pedal. They suppress effector T-cells, including autoreactive ones, and maintain peripheral tolerance. Calcitriol promotes Treg differentiation by:
- Inducing FoxP3 expression, the master transcription factor for Treg identity
- Promoting CD25 (IL-2 receptor) expression, which Tregs need to compete for IL-2
- Synergizing with TGF-β in driving Treg differentiation
The net effect of calcitriol on the adaptive immune system is therefore a coordinated shift: fewer pathogenic Th17 cells, more suppressive Tregs, and tolerogenic dendritic cells presenting self-antigens in a way that doesn't trigger autoreactive responses. This is exactly the immune phenotype seen in healthy individuals and lost in autoimmune patients.
The 22% autoimmune reduction in VITAL is consistent with this mechanism: vitamin D doesn't eliminate autoimmunity (the immune system can still mount autoreactive responses to strong genetic or environmental triggers), but it provides ongoing tonic support for the regulatory phenotype that suppresses incipient autoimmunity before it becomes clinically evident.
Multiple Sclerosis — Ascherio, Latitude, Prevention
Multiple sclerosis (MS) is the autoimmune disease with the strongest, most consistent evidence for a vitamin D connection. Three lines of evidence converge:
The latitude gradient
MS incidence rises dramatically with distance from the equator. In the United States, MS is roughly 3-4 times more common in Minnesota than in Florida. In the Australasian region, MS is roughly 7 times more common in Tasmania than in Queensland. These gradients track UVB intensity and therefore endogenous vitamin D synthesis, suggesting that childhood and young-adult vitamin D status (when MS is sown) is a major determinant of lifetime risk.
Migration studies reinforce the inference: individuals who migrate from a high-MS-risk to a low-MS-risk region before age 15 acquire the lower risk of their adopted region. Those who migrate after age 15 retain the higher risk of their birthplace. This suggests that childhood vitamin D status is the critical exposure.
The Ascherio prospective cohort data
Alberto Ascherio (Harvard) and colleagues used the Nurses Health Study cohorts to test the vitamin D-MS hypothesis prospectively. Higher dietary vitamin D intake (with or without supplements) was associated with approximately 40% lower MS risk. More compellingly, women with serum 25(OH)D in the highest quintile (above approximately 40 ng/mL) had roughly 50% lower MS risk than those in the lowest quintile. This was a graded, dose-response relationship.
Subsequent work in active-duty US military personnel (who have serial blood draws routinely banked) confirmed that pre-disease 25(OH)D levels were predictive of subsequent MS diagnosis — the lower the level, the higher the risk.
Vitamin D in established MS
For patients with established MS, evidence supports vitamin D supplementation as a disease-modifying adjunct, though it does not replace standard MS therapies. The SOLAR and CHOLINE trials showed reduced relapse rates and slowed brain atrophy in MS patients given high-dose vitamin D, though effect sizes were modest. The Charcot Project and ongoing trials continue to refine optimal dosing.
The clinical takeaway for MS: aggressive 25(OH)D optimization (target 50-80 ng/mL minimum, with some specialists targeting higher) is now standard in integrative MS practice. Vitamin D is complementary to disease-modifying therapies, not a substitute. For prevention in those at risk (family history, female, northern latitude), maintaining 25(OH)D above 40-50 ng/mL throughout childhood and young adulthood is the most plausible intervention currently available.
Type 1 Diabetes — Finnish Infant Supplementation
Type 1 diabetes (T1D) is an autoimmune destruction of insulin-producing pancreatic beta cells, typically with onset in childhood or young adulthood. The classic vitamin D-T1D study is the Finnish birth cohort published by Hyppönen et al. in Lancet (2001).
In Finland during the 1960s, infants were routinely supplemented with cod liver oil (which provided approximately 2,000 IU/day of vitamin D3) during the first year of life. The Hyppönen team followed 10,366 of these infants for over 30 years and assessed T1D incidence.
- Infants given vitamin D supplementation in their first year had approximately 78% reduction in T1D risk over 31 years of follow-up compared to non-supplemented infants (RR 0.22, 95% CI 0.05-0.89)
- Infants with suspected rickets (the marker of severe deficiency) had approximately 3-fold increased T1D risk
- The dose-response was clear: regular supplementation gave more protection than irregular supplementation, which gave more than none
This is an extraordinary effect size for a nutritional intervention — comparable in magnitude to the most effective vaccines. Other observational studies (EURODIAB case-control, Norwegian birth cohorts) have replicated the protective effect, though with more modest effect sizes (typically 25-50% reduction).
The mechanistic rationale: T1D arises when autoreactive T-cells destroy pancreatic beta cells. Vitamin D's Treg-promoting and Th17-suppressing effects directly oppose this autoimmune cascade. The first year of life is a critical window during which the developing immune system establishes tolerance toward self-antigens, and adequate vitamin D during this window may program lifelong protection against beta-cell autoimmunity.
The clinical takeaway: vitamin D supplementation in infancy and early childhood may meaningfully reduce T1D risk, particularly in high-risk populations (family history, HLA-DR3/DR4 genotype). The standard pediatric recommendation of 400 IU/day for all breastfed infants is the minimum; many natural-medicine pediatricians use 800-1,200 IU/day. Pregnant women in high-risk pregnancies may benefit from optimizing their own 25(OH)D to support fetal immune programming.
Inflammatory Bowel Disease (Crohn's, UC)
Crohn's disease and ulcerative colitis (collectively, inflammatory bowel disease or IBD) are autoimmune-inflammatory conditions of the intestinal tract. The vitamin D connection is multifaceted:
Epidemiology
- IBD incidence shows the same latitude gradient as MS — more common in northern populations
- Low 25(OH)D is highly prevalent in IBD patients (often < 15 ng/mL even outside winter)
- Low 25(OH)D predicts worse disease course, more frequent flares, more steroid courses, more hospitalizations, and higher rates of surgery
Mechanism
Vitamin D's IBD-relevant effects include:
- Treg expansion in gut-associated lymphoid tissue (suppressing the autoreactive responses that drive IBD)
- Upregulation of intestinal tight-junction proteins (claudins, occludin, ZO-1), reducing the "leaky gut" that allows microbial antigens to drive inflammation
- Cathelicidin LL-37 induction in intestinal epithelium (improving antimicrobial defense)
- Modulation of the gut microbiome composition
- Direct anti-inflammatory effects on intestinal mucosa
Trial evidence
Multiple small RCTs have shown that vitamin D supplementation reduces inflammatory markers, improves quality of life, and reduces relapse rates in IBD. Effect sizes are modest, but trial doses have generally been conservative (1,000-4,000 IU/day). Some integrative gastroenterologists use much higher doses (10,000-20,000 IU/day) for active IBD with calcium and 25(OH)D monitoring.
Note that IBD patients have increased risk of vitamin D toxicity at standard doses because intestinal inflammation can paradoxically increase calcitriol production (via inflammatory upregulation of 1α-hydroxylase). Monitor calcium and 25(OH)D carefully in IBD patients on higher-dose D3.
Hashimoto's Thyroiditis
Hashimoto's thyroiditis is the most common cause of hypothyroidism in iodine-sufficient regions and is fundamentally an autoimmune destruction of the thyroid gland mediated by anti-TPO (thyroid peroxidase) and anti-thyroglobulin antibodies. Vitamin D's role in Hashimoto's:
- Low 25(OH)D is observed in 70-90% of Hashimoto's patients
- Lower 25(OH)D correlates with higher anti-TPO antibody titers in observational studies
- Several RCTs (including Mazokopakis et al. 2015 and Krysiak 2018) have shown that vitamin D supplementation reduces anti-TPO antibody levels by 20-50% over 4-6 months, particularly in patients starting from low baseline 25(OH)D
- The autoimmune-modulating mechanism (Treg expansion, Th17 suppression) is the proposed driver
Whether antibody reduction translates into preservation of thyroid function over the long term is less clear — Hashimoto's typically progresses slowly, and trials long enough to detect levothyroxine-dose reduction or restoration of normal TSH have not been completed. But the antibody-reduction signal is consistent and the safety profile is excellent, so vitamin D optimization is now standard in integrative Hashimoto's management.
For Hashimoto's, target 25(OH)D 60-80 ng/mL, combine with selenium 200 mcg/day (which independently reduces anti-TPO antibodies), and ensure adequate iodine intake without excess. See the Hashimoto's page for the broader protocol.
Psoriasis (Topical and Systemic)
Psoriasis is the autoimmune condition where vitamin D's clinical role is most established — topical vitamin D analogues (calcipotriol, calcitriol, tacalcitol, maxacalcitol) are first-line treatments for plaque psoriasis.
Topical analogues
Topical calcipotriol (the most widely used) is applied directly to psoriatic plaques and works through three mechanisms: it normalizes keratinocyte differentiation (psoriatic keratinocytes are hyperproliferative and undifferentiated), it reduces local Th17 and IL-17 activity, and it activates local Tregs. Effect onset is typically 4-8 weeks; combination with topical corticosteroids accelerates response.
Systemic supplementation
Systemic vitamin D3 supplementation (separate from topical analogues) is also valuable. Psoriasis patients have lower 25(OH)D than controls, and supplementation reduces PASI (Psoriasis Area and Severity Index) scores in several RCTs. The systemic approach addresses the underlying immunoregulatory abnormality that drives flares, while topical analogues address the current visible lesions.
Coimbra protocol use
Psoriasis is one of the conditions where the Coimbra Protocol (very high-dose vitamin D, calcium-restricted diet) has been used most extensively. Many treatment-resistant patients report dramatic improvement or remission on the protocol, though it requires specialist supervision (see below).
Lupus and Rheumatoid Arthritis
Systemic Lupus Erythematosus (SLE)
SLE patients almost universally have low 25(OH)D, partly because they are advised to avoid sun exposure (sun exposure triggers lupus flares) and partly because of the disease itself. Low 25(OH)D in SLE is associated with higher disease activity, more frequent flares, increased anti-dsDNA antibody titers, and worse cardiovascular outcomes.
Supplementation trials in SLE have generally shown improvements in fatigue scores and disease activity, but no large definitive trials have established disease-modifying effects. The strategy in integrative SLE management is to optimize 25(OH)D to 60-80 ng/mL using daily oral supplementation (since sun avoidance is mandatory), combined with standard immunosuppressive therapy.
Rheumatoid Arthritis (RA)
RA shares much of the same biology — Th17-driven autoimmune attack on joint tissue. Vitamin D deficiency is common in RA, correlates with disease activity, and supplementation in several trials has shown modest reductions in tender joint counts, morning stiffness, and DAS28 (disease activity) scores.
RA patients are also at elevated osteoporosis risk (from chronic inflammation, glucocorticoid use, and reduced activity), so the bone-protective effects of vitamin D add to its autoimmune-modulatory benefits. The quartet protocol (D3 + K2 + magnesium + calcium) is particularly important in RA patients.
The Coimbra Protocol (High-Dose Supervised)
The Coimbra Protocol is a treatment approach developed by Brazilian neurologist Cicero Galli Coimbra for severe autoimmune disease. It uses very-high-dose vitamin D (typically 40,000-200,000 IU/day, dose-titrated to suppress PTH to a low-normal range) combined with a strict calcium-restricted diet (essentially no dairy, low-calcium plant foods only) and daily hydration of 2.5+ liters of water.
The rationale is based on observations of vitamin D receptor polymorphisms in autoimmune patients — the Coimbra group hypothesizes that many autoimmune patients have reduced VDR sensitivity, requiring supraphysiologic 25(OH)D levels (often above 100 ng/mL, sometimes above 300 ng/mL) to achieve adequate VDR activation in immune cells. The calcium restriction and high water intake are protective measures to prevent hypercalcemia and kidney stones at these extreme doses.
Reported clinical experience (mostly published as case series) describes substantial improvements in MS, psoriasis, lupus, RA, IBD, and other conditions, with high rates of disease stabilization or improvement. The protocol has spread internationally; certified Coimbra physicians practice in many countries.
Critical caveats:
- The Coimbra Protocol is not a self-administered intervention. The doses used (10-50 times typical supplementation) can cause severe hypercalcemia and kidney damage in inadequately monitored patients.
- Periodic 25(OH)D, calcium (serum and 24-hour urine), PTH, kidney function, and DEXA monitoring are mandatory.
- The calcium-restricted diet is non-negotiable; even occasional dairy can trigger hypercalcemic episodes.
- Randomized trial evidence is limited; the protocol is supported by case series and clinician experience rather than definitive RCTs.
- Patients interested in the protocol should seek a certified Coimbra Protocol practitioner; do not attempt high-dose vitamin D therapy without specialist supervision.
For the typical autoimmune patient, conventional integrative vitamin D supplementation (5,000-10,000 IU/day with K2 and magnesium, target 25(OH)D 60-100 ng/mL) provides a substantial fraction of the benefit at far lower risk. The Coimbra Protocol is reserved for severe, treatment-resistant cases under specialist care.
Target 25(OH)D for Autoimmune Outcomes
| Indication | Target 25(OH)D | Typical D3 Dose |
|---|---|---|
| Autoimmune prevention (family history, no disease) | 50-70 ng/mL | 2,000-5,000 IU/day |
| Established autoimmune disease (stable, on conventional therapy) | 60-100 ng/mL | 5,000-10,000 IU/day |
| Active flare or treatment-resistant | 80-150 ng/mL (with monitoring) | 10,000-20,000 IU/day under specialist care |
| Coimbra Protocol | 100-300+ ng/mL (PTH-suppressed) | 40,000-200,000 IU/day, certified Coimbra physician only |
K2 and magnesium dosing scales with D3 dose. For 10,000 IU/day D3, use approximately 200 mcg MK-7 and 400 mg elemental magnesium. For Coimbra-level doses, K2 and magnesium scale up substantially under specialist guidance.
Cautions
- Hypercalcemia — the principal risk of higher-dose autoimmune protocols. Monitor serum calcium every 1-3 months at doses above 5,000 IU/day, more frequently above 10,000 IU/day, and at every visit on the Coimbra Protocol.
- Kidney stones and nephrocalcinosis — risk rises with hypercalciuria. Monitor 24-hour urinary calcium periodically on higher-dose protocols.
- Sarcoidosis and granulomatous disease — absolute caution. Granuloma macrophages produce calcitriol without normal regulation. Even modest D3 doses can cause hypercalcemia. Specialist supervision and frequent calcium monitoring are mandatory.
- Hypercalcemia of malignancy — some lymphomas and other tumors produce calcitriol, mimicking sarcoidosis biology. Investigate persistent hypercalcemia in any vitamin D-supplemented patient.
- Drug interactions in autoimmune patients — many autoimmune patients are on glucocorticoids (accelerate D3 catabolism, requiring higher doses), hydroxychloroquine (lupus — no significant D3 interaction), methotrexate (no significant interaction), and biologics (no significant interaction). Anticonvulsants used for autoimmune neurologic conditions accelerate D3 metabolism.
- Pregnancy and breastfeeding — vitamin D is safe and beneficial during pregnancy at 4,000-6,000 IU/day (Hollis RCT). Very-high-dose Coimbra-style protocols should not be initiated in pregnancy.
- Coimbra Protocol-specific cautions — absolute requirement for calcium-restricted diet, 2.5+ L daily water intake, frequent monitoring of calcium and kidney function. Patients who cannot reliably adhere to the calcium restriction should not be on the protocol.
- K2 with warfarin — K2 antagonizes warfarin's anticoagulant effect. Patients on warfarin who add K2 should have INR monitored and warfarin dose adjusted; the K2 dose should be kept stable rather than oscillating.
Key Research Papers
- Hahn J, Cook NR, Alexander EK, et al. (2022). Vitamin D and marine omega-3 fatty acid supplementation and incident autoimmune disease: VITAL randomized controlled trial. BMJ 376:e066452. — PubMed
- Hyppönen E, Läärä E, Reunanen A, Järvelin MR, Virtanen SM (2001). Intake of vitamin D and risk of type 1 diabetes: a birth-cohort study. Lancet 358:1500-1503. — PubMed
- Munger KL, Levin LI, Hollis BW, Howard NS, Ascherio A (2006). Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis. JAMA 296:2832-2838. — PubMed
- Ascherio A, Munger KL, White R, et al. (2014). Vitamin D as an early predictor of multiple sclerosis activity and progression. JAMA Neurology 71:306-314. — PubMed
- Mazokopakis EE, Papadakis JA, Papadomanolaki MG, et al. (2007). Effects of 12 months treatment with L-selenomethionine on serum anti-TPO levels in patients with Hashimoto's thyroiditis. Thyroid. — PubMed
- Krysiak R, Szkróbka W, Okopień B (2018). The effect of vitamin D on thyroid autoimmunity in levothyroxine-treated women with Hashimoto's thyroiditis and normal vitamin D status. Exp Clin Endocrinol Diabetes. — PubMed
- Cantorna MT (2010). Mechanisms underlying the effect of vitamin D on the immune system. Proc Nutr Soc. — PubMed
- Joshi S, Pantalena LC, Liu XK, et al. (2011). 1,25-dihydroxyvitamin D3 ameliorates Th17 autoimmunity via transcriptional modulation of interleukin-17A. Mol Cell Biol. — PubMed
- Smolders J, Thewissen M, Peelen E, et al. (2009). Vitamin D status is positively correlated with regulatory T cell function in patients with multiple sclerosis. PLoS One. — PubMed
- Jorgensen SP, Agnholt J, Glerup H, et al. (2010). Clinical trial: vitamin D3 treatment in Crohn's disease — a randomized double-blind placebo-controlled study. Aliment Pharmacol Ther. — PubMed
- Amrein K, Scherkl M, Hoffmann M, et al. (2020). Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. — PubMed
- Finamor DC, Sinigaglia-Coimbra R, Neves LCM, et al. (2013). A pilot study assessing the effect of prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis. Dermatoendocrinol. (Early Coimbra protocol paper.) — PubMed
PubMed Topic Searches
- PubMed: vitamin D autoimmune disease VITAL trial
- PubMed: vitamin D multiple sclerosis latitude
- PubMed: vitamin D type 1 diabetes pediatric prevention
- PubMed: vitamin D IBD Crohn colitis
- PubMed: vitamin D Hashimoto anti-TPO
- PubMed: Coimbra protocol high-dose vitamin D
Connections
- Vitamin D3 Overview
- D3 Benefits Hub
- D3 for Bone Health
- D3 for Immune Function
- D3 for Mood & Depression
- Multiple Sclerosis
- Hashimoto's Thyroiditis
- Diabetes (Type 1)
- Inflammatory Bowel Disease
- Psoriasis
- Lupus (SLE)
- Rheumatoid Arthritis
- Vitamin K2
- Vitamin A
- Magnesium
- Selenium
- Omega-3 Fatty Acids
- Vitamin D Test
- Calcium — the mineral whose absorption vitamin D governs; restricted on the Coimbra Protocol and monitored on every higher-dose D3 regimen.