Vitamin D Deficiency: Symptoms, Causes, and Recovery
Vitamin D deficiency is one of the most common nutritional shortfalls in the world — by many estimates close to a billion people have levels that are too low. It is easy to miss because for a long time it causes nothing you can feel: no rash, no pain, no obvious sign. Then, quietly, it begins to show up as aching bones, muscles that tire and weaken, a higher chance of falls in older adults, low energy, and, for some, a flat or low mood that deepens through the dark winter months. In children a severe, long-standing lack can soften and bow the growing bones — the disease called rickets — while in adults the same softening is called osteomalacia. The reason one shortage reaches so far is that vitamin D is not really a simple vitamin at all: your body turns it into a hormone that controls how much calcium you absorb from food and how strong your bones and muscles become. The encouraging part is that this is one of the easiest deficiencies to find — a single blood test, the 25-hydroxyvitamin D level — and one of the easiest to fix, with sunlight, a few foods, and inexpensive supplements. This hub explains what the deficiency is, why one low number causes such different symptoms, who is most at risk, how it is diagnosed, and exactly how it is corrected — with deep-dive pages for each of the major symptoms.
Symptom Deep-Dive Pages
Bone Pain & Osteomalacia
The deep, aching bone pain and tenderness of osteomalacia — the adult softening of bone that low vitamin D can cause. What it feels like, why undermineralized bone hurts, and how it differs from arthritis and fibromyalgia.
Rickets in Children
How a long, severe shortage of vitamin D softens a child's growing bones, producing bowed legs, swollen wrists, delayed walking, and growth problems — and why rickets is both preventable and treatable.
Muscle Weakness & Falls
Why low vitamin D weakens the large muscles closest to the body's core, making it hard to climb stairs or rise from a chair, and how that proximal weakness raises the risk of falls and fractures in older adults.
Fatigue & Low Mood
The tiredness and flat, low mood that many people with low vitamin D describe — what the evidence actually shows, why winter and low sunlight matter, and how to tell a true deficiency from the many other causes of feeling worn down.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Vitamin D Deficiency?
- Why One Low Number Causes So Many Symptoms
- Common Causes of Low Vitamin D
- Who Is Most at Risk
- How Vitamin D Deficiency Is Diagnosed
- How Low Vitamin D Is Corrected
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Is Vitamin D Deficiency?
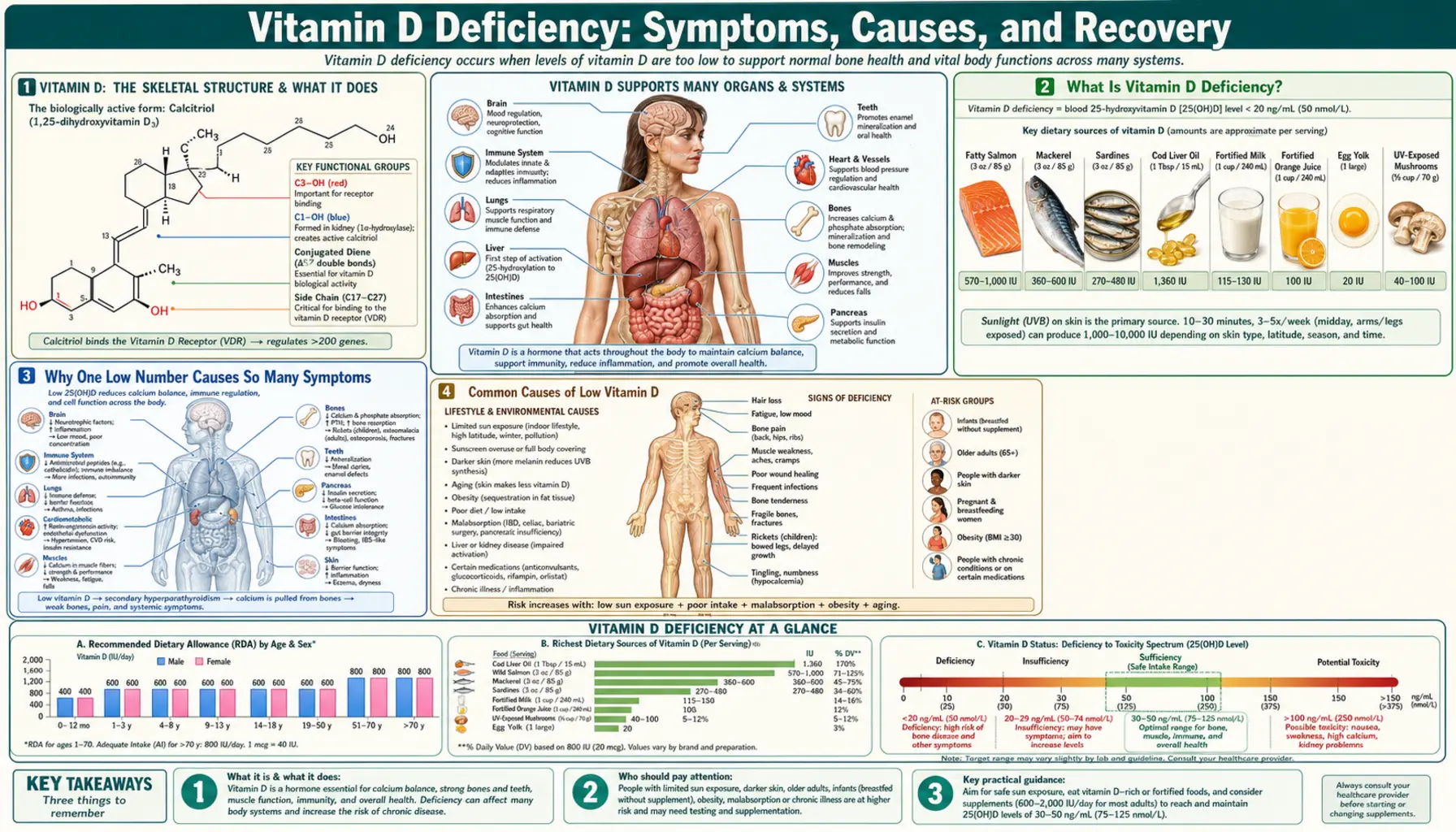
Vitamin D deficiency means your body does not have enough vitamin D to do its main jobs — chiefly absorbing calcium and keeping bones and muscles strong. Doctors do not measure vitamin D by how much you eat; they measure the form that circulates in your blood, called 25-hydroxyvitamin D (often written 25(OH)D). This is the storage form the liver makes, and it is the best single marker of your overall vitamin D status. The result is usually reported in nanograms per milliliter (ng/mL) in the United States, or in nanomoles per liter (nmol/L) elsewhere; to convert, multiply ng/mL by 2.5.
There is genuine, long-running debate among expert groups about exactly where "low" begins, and it is worth being honest about that rather than pretending there is one universal cutoff. Two influential frameworks bracket the discussion. The Institute of Medicine (now the National Academy of Medicine), focusing on what bones need across the whole population, judged that a level of 20 ng/mL (50 nmol/L) is sufficient for almost everyone, and that true deficiency — the level linked to rickets and osteomalacia — sits below about 12 ng/mL (30 nmol/L). The Endocrine Society, focusing on patients at risk, set a higher bar, defining deficiency as below 20 ng/mL and "insufficiency" as 21–29 ng/mL, and suggesting 30 ng/mL or above as a target for those being treated. In everyday clinical practice, most laboratories and clinicians use roughly these bands:
- Severe deficiency (below 10–12 ng/mL / under ~30 nmol/L) — this is the range associated with the classic bone diseases, rickets in children and osteomalacia in adults, and the most likely to cause symptoms you can feel. It clearly needs treatment.
- Deficiency (12–20 ng/mL / 30–50 nmol/L) — below what is considered adequate for bone health; commonly treated, especially in people with risk factors or symptoms.
- Insufficiency / "in-between" (21–29 ng/mL / 52–72 nmol/L) — a gray zone. Some experts treat it, others consider it adequate. The right call depends on the person.
- Sufficient (30 ng/mL and above / 75 nmol/L and above) — comfortably adequate for bone health by every standard.
The key practical point is that mild and moderate shortfalls usually cause no symptoms at all — this is the most important thing to understand about vitamin D deficiency. Most low levels are found by chance on a blood test, not because the person felt unwell. Symptoms tend to appear only when the level is quite low and has stayed low for a long time, because it takes months of inadequate calcium handling for bones and muscles to noticeably suffer. That silence is exactly why deficiency is so common and so easy to overlook.
Why One Low Number Causes So Many Symptoms
It can seem strange that a single low vitamin can be blamed for problems as different as aching bones, weak legs, falls, and low mood. The explanation is that vitamin D is not a typical vitamin that simply plugs into one chemical reaction. Once in the body it is converted, in two steps, into a hormone — first by the liver into 25-hydroxyvitamin D (the form we measure), then by the kidney into the active hormone calcitriol (1,25-dihydroxyvitamin D). That hormone travels through the blood and acts on receptors found in a remarkable range of tissues, which is why a shortage ripples outward.
The central job — the one that explains the bone and muscle symptoms — is calcium. Active vitamin D is the main signal that tells your gut to absorb calcium and phosphate from food. When vitamin D runs low, you absorb far less calcium, sometimes only 10–15% of what you eat instead of 30–40%. The body refuses to let blood calcium fall, because the heart and nerves depend on it, so it triggers a backup system: the parathyroid glands release more parathyroid hormone (PTH), which pulls calcium out of the bones to keep the blood level normal. This state — called secondary hyperparathyroidism — quietly drains the skeleton. (See Hyperparathyroidism for more on this hormone system, and Calcium and Phosphorus for the minerals involved.)
From that one disturbance, the different symptoms follow:
- Bone — without enough calcium and phosphate, newly built bone cannot harden properly, leaving it soft and undermineralized. In adults this is osteomalacia, which causes a deep, aching bone pain and tenderness; in growing children it is rickets, which deforms the soft bones into bowed legs and swollen joints. The constant pull of PTH also worsens long-term bone density.
- Muscle — vitamin D receptors sit on muscle cells, and the hormone helps muscles work normally. Low levels cause a characteristic weakness of the large muscles near the hips and shoulders, making it hard to climb stairs or rise from a chair — and, in older adults, raising the risk of falls.
- Energy and mood — vitamin D receptors are also present in the brain, and low levels are statistically linked with fatigue and low mood, though here the evidence is weaker and the link is less certain than for bone. See also Vitamin D and Mood.
- Immune function — immune cells carry vitamin D receptors too, which is why low status has been studied in relation to infections and autoimmune conditions, although supplementing has not proven to be a cure-all (see Vitamin D and Immune Function).
This is the unifying idea: vitamin D acts like a hormone that quietly manages calcium and supports bone, muscle, and other tissues. So a single, long-standing shortage is felt in several places at once — and correcting it tends to help those systems together.
Common Causes of Low Vitamin D
Vitamin D is unusual among nutrients because most of it does not come from food at all — in most people, the majority is made in the skin when ultraviolet B (UVB) sunlight strikes it. That means low vitamin D usually traces back to one of three things: not making enough in the skin, not taking in enough from food or supplements, or, less often, a medical problem that interferes with how the body absorbs or processes it. Here are the causes worth knowing.
- Too little sun on the skin — the single biggest reason. Spending most of the day indoors, living far from the equator (where winter sunlight is too weak to make vitamin D for months at a time), covering the skin for cultural or sun-safety reasons, and routine sunscreen use all reduce the amount the skin produces. None of these are "wrong" — sun protection prevents skin cancer — but they shift the burden onto diet and supplements.
- Darker skin — melanin is a natural sunscreen. People with more deeply pigmented skin need substantially more sun exposure to make the same amount of vitamin D, which is why deficiency is markedly more common in people with darker skin living in temperate climates.
- Older age — the skin's ability to produce vitamin D falls with age, so an older adult makes far less vitamin D from the same sunlight as a young person. Combined with more time indoors, this makes the elderly especially prone to deficiency.
- A diet low in vitamin D — very few foods naturally contain much vitamin D. The richest are fatty fish such as salmon, sardines, and cod (and cod liver oil); smaller amounts are in egg yolks and some mushrooms. Many countries fortify milk and some cereals, but a diet without these can supply very little.
- Fat malabsorption — vitamin D is fat-soluble, so any condition that impairs fat absorption also impairs vitamin D absorption. This includes celiac disease, Crohn's disease and other inflammatory bowel disease, cystic fibrosis, chronic pancreatitis, and the years after weight-loss (bariatric) surgery, especially gastric bypass.
- Obesity — vitamin D is stored in body fat, so in people with a higher body fat mass the vitamin is sequestered away from the bloodstream, lowering the measured blood level even when total body stores are not necessarily low. People with obesity often need higher doses to reach the same blood level.
- Liver or kidney disease — because the liver and kidney perform the two activation steps, advanced disease in either organ can reduce the body's ability to make active vitamin D, even when intake is adequate.
- Certain medications — some drugs speed up the breakdown of vitamin D in the liver, lowering levels over time. These include several anti-seizure medicines (such as phenytoin, phenobarbital, and carbamazepine), the tuberculosis drug rifampin, the steroid prednisone, and certain HIV medications.
- Exclusive breastfeeding without a supplement — breast milk is naturally low in vitamin D, so exclusively breastfed infants who are not given a vitamin D supplement are at real risk — a leading cause of rickets in babies (covered in detail on the Rickets in Children page).
As with most deficiencies, these causes often stack. An older adult with darker skin who lives in a northern city, stays mostly indoors, and eats little fish can become deficient from the sum of several ordinary factors, none of which alone would be enough.
Who Is Most at Risk
Because so many of the causes above are common, vitamin D deficiency is widespread — but some groups are far more likely to be affected and are the ones in whom doctors most often check a level. If you recognize yourself in this list, it is reasonable to ask about testing.
- Older adults — the highest-risk group overall. Aging skin makes less vitamin D, time outdoors tends to fall, intake is often low, and the consequences (falls and fractures) are most serious. This is why vitamin D matters so much in muscle strength and fall prevention.
- People with darker skin — needing more sun to make the same amount, they have consistently higher rates of low blood levels in temperate countries.
- Infants who are exclusively breastfed — breast milk's low vitamin D content means a daily supplement (commonly 400 IU) is recommended for breastfed babies in many countries to prevent rickets.
- People who get little sun — those who are housebound, work night shifts, are in residential care, live at high latitudes, or cover most of their skin.
- Pregnant and breastfeeding women — the demands of pregnancy and lactation, layered on any pre-existing shortfall, make adequate vitamin D especially important for both mother and baby.
- People with obesity — with vitamin D held in fat tissue, blood levels are commonly low and higher doses are usually needed.
- People with malabsorption conditions — celiac disease, inflammatory bowel disease, cystic fibrosis, and a history of gastric bypass or other bariatric surgery.
- People with chronic kidney or liver disease — whose ability to activate vitamin D is reduced.
- People taking the medications listed above — anti-seizure drugs, glucocorticoids, rifampin, and certain antiretrovirals.
Worth a note: vitamin D screening is not recommended for the whole healthy population, and routine testing in people with no risk factors and no symptoms has uncertain value. Testing is most useful when you have a reason — symptoms that fit, a bone or malabsorption condition, or membership in one of the higher-risk groups above.
How Vitamin D Deficiency Is Diagnosed
The good news, again, is how simple the diagnosis is. Vitamin D status is measured with a single, widely available blood test for 25-hydroxyvitamin D (25(OH)D). It does not require fasting, it is inexpensive, and it is the one test that reliably reflects your overall vitamin D stores — combining what you make from sunlight and what you take in from food and supplements. (For a fuller explanation of the test, the result ranges, and how to read your report, see the dedicated Vitamin D Test (25-Hydroxyvitamin D) page.)
A few practical points make the test easier to understand:
- It is 25(OH)D, not the active hormone, that is measured. A different test, for 1,25-dihydroxyvitamin D (the active form), exists but is rarely the right test for diagnosing ordinary deficiency — it can look deceptively normal even when stores are low, because the body ramps up activation to compensate. It is reserved for specific kidney and calcium disorders.
- The number is interpreted against the bands above — broadly, below ~12 ng/mL is severe deficiency, 12–20 ng/mL is deficiency, 21–29 ng/mL is the in-between zone, and 30 ng/mL or above is sufficient by every standard. Remember that the exact cutoff is a matter of expert debate, so your clinician interprets it alongside your symptoms and risks, not in isolation.
When the level is found to be low — especially if it is very low, or if you have bone symptoms — a doctor may add a few related tests to understand the full picture and to look for the consequences of long-standing deficiency:
- Calcium — usually still normal in deficiency (the body works hard to keep it so), but checked because a low calcium signals more advanced disease.
- Phosphate — often low in osteomalacia and rickets, an important clue to softened bone.
- Parathyroid hormone (PTH) — frequently raised in long-standing deficiency (the secondary hyperparathyroidism described above), confirming that the low vitamin D is actively affecting calcium handling.
- Alkaline phosphatase — an enzyme that tends to rise when bone is being remodeled abnormally, as in osteomalacia and rickets.
- Kidney and liver function — checked when there is reason to suspect these organs are part of the problem.
In children with suspected rickets, and occasionally in adults with severe osteomalacia, an X-ray may be added because softened, poorly mineralized bone has a characteristic appearance — the details are on the Rickets in Children page.
How Low Vitamin D Is Corrected
Treating vitamin D deficiency is, for most people, straightforward, inexpensive, and effective. The general approach has three parts: raise the level with supplements (and food and sensible sun), make sure calcium intake is adequate so the corrected vitamin D has the raw material to work with, and address whatever caused the deficiency so it does not simply return.
- Food first, but realistically. A vitamin-D-rich diet is healthy and worth pursuing, but honesty matters: food alone usually cannot correct an established deficiency, because so few foods are rich enough. The best natural sources are fatty fish — salmon, sardines, cod and cod liver oil — with smaller amounts in eggs, some mushrooms, and fortified milk and cereals. (The fuller list and amounts are on the Vitamin D3 food sources page.) Food is excellent for maintaining a good level, less so for repairing a deep deficit.
- Supplements are the mainstay. The form used for treatment is usually vitamin D3 (cholecalciferol), the same form the skin makes; it raises and sustains blood levels somewhat more effectively than the plant-derived D2 (ergocalciferol). For ongoing maintenance in adults, common daily doses are in the range of 600–800 IU (the official Recommended Dietary Allowance is 600 IU for most adults and 800 IU for those over 70). To correct an established deficiency, clinicians typically prescribe a higher loading dose for a period — for example, around 50,000 IU once a week for 6–8 weeks, or an equivalent daily dose — then drop to a maintenance dose and re-check the level after a few months. Doses should be individualized; people with obesity or malabsorption often need more.
- Don't forget calcium. Because vitamin D's main job is to help you absorb calcium, correcting vitamin D works best when calcium intake is also adequate — from calcium-rich foods first. In severe deficiency with very soft bones, treatment is sometimes started carefully under medical supervision, because rapidly improving calcium absorption in someone who is calcium-depleted needs monitoring.
- Sensible sunlight — short, non-burning sun exposure helps the body make its own vitamin D and supports a healthy level, though it should never come at the cost of sunburn or skin-cancer risk, and it is unreliable in winter at higher latitudes. It is a useful supplement to, not a replacement for, the measures above.
- Treat the cause. Correcting the level without fixing why it dropped just resets the clock. That might mean managing a malabsorption condition, adjusting a medication where possible, using higher maintenance doses in obesity, or simply committing to a year-round supplement for someone who gets little sun.
A word of balance on expectations: vitamin D reliably prevents and treats the diseases of deficiency — rickets, osteomalacia, and, with adequate calcium, it supports bone strength and reduces falls and fractures in deficient older adults. But large trials such as the VITAL study found that giving extra vitamin D to people who are not deficient does not prevent cancer, heart disease, or most other conditions. The honest summary is that fixing a real deficiency is genuinely worthwhile; taking ever-higher doses beyond sufficiency is not, and can eventually cause harm (see the Vitamin D Toxicity hub).
For most people, the outlook is excellent: once a true deficiency is corrected and the cause addressed, bone pain eases, muscle strength returns, and energy often improves over weeks to a few months.
When to Seek Care / Red Flags
Vitamin D deficiency itself is rarely an emergency — it develops slowly and is corrected at a measured pace. For most situations, the right step is a non-urgent visit to your doctor for a blood test: ask to be checked if you have ongoing bone aches, unexplained muscle weakness, frequent falls, or persistent low energy, especially if you fall into one of the higher-risk groups above. But a few signs deserve prompt medical attention, either because they point to severe or advanced deficiency or because they suggest a different, more serious problem that should not be missed.
- In an infant or young child: delayed walking, bowed or knock-kneed legs, swelling at the wrists or ankles, a soft skull, or poor growth — these can be signs of rickets and should be evaluated by a doctor without long delay.
- In a baby: muscle spasms, twitching, or a seizure — severe deficiency can drop blood calcium low enough to cause these, which is a medical emergency requiring immediate care.
- Severe, unrelenting, or rapidly worsening bone pain — while osteomalacia can ache deeply, bone pain that is severe, focused on one spot, or escalating quickly should be checked promptly, since several other conditions can cause it.
- A bone that breaks after a minor fall or with little force — a so-called fragility fracture warrants medical evaluation of bone health.
- Marked or worsening muscle weakness, especially with falls — this should be assessed both to treat any deficiency and to look for other causes.
- Numbness, tingling around the mouth or in the hands and feet, or muscle cramps and spasms in an adult — possible signs of low blood calcium from severe deficiency, which should be evaluated.
One more piece of honest framing: feeling tired or low is extremely common and has many causes, and a low vitamin D level found on testing is not proof that vitamin D is the reason you feel that way — a point explored on the Fatigue & Low Mood page. It is reasonable to correct a genuine deficiency and see whether you improve, while keeping an open mind about other explanations. When symptoms are severe, persistent, or do not improve after the deficiency is corrected, that is the signal to look further. For general tiredness, see also Fatigue.
Key Research Papers
- Holick MF (2007). Vitamin D Deficiency. New England Journal of Medicine;357(3):266-281. — DOI: 10.1056/NEJMra070553
- Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, et al. (2011). Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism;96(7):1911-1930. — DOI: 10.1210/jc.2011-0385
- Rosen CJ, Abrams SA, Aloia JF, Brannon PM, Clinton SK, et al. (2012). IOM Committee Members Respond to Endocrine Society Vitamin D Guideline (2011 Report on Dietary Reference Intakes for Calcium and Vitamin D). Journal of Clinical Endocrinology & Metabolism;97(4):1146-1152. — DOI: 10.1210/jc.2010-2704
- Pearce SH, Cheetham TD (2010). Diagnosis and management of vitamin D deficiency. BMJ;340:b5664. — DOI: 10.1136/bmj.b5664
- Pfotenhauer KM, Shubrook JH (2017). Vitamin D Deficiency, Its Role in Health and Disease, and Current Supplementation Recommendations. Journal of the American Osteopathic Association;117(5):301-305. — DOI: 10.7556/jaoa.2017.055
- Munns CF, Shaw N, Kiely M, Specker BL, Thacher TD, et al. (2016). Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. Journal of Clinical Endocrinology & Metabolism;101(2):394-415. — DOI: 10.1210/jc.2015-2175
- Reid IR, Bolland MJ, Grey A (2014). Effects of vitamin D supplements on bone mineral density: a systematic review and meta-analysis. Lancet;383(9912):146-155. — DOI: 10.1016/S0140-6736(13)61647-5
- Bolland MJ, Grey A, Gamble GD, Reid IR (2014). The effect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: a trial sequential meta-analysis. Lancet Diabetes & Endocrinology;2(4):307-320. — DOI: 10.1016/S2213-8587(13)70212-2
- Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, Orav JE, Stuck AE, et al. (2009). Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. BMJ;339:b3692. — DOI: 10.1136/bmj.b3692
- Ceglia L (2008). Vitamin D and its role in skeletal muscle. Molecular Aspects of Medicine;29(6):407-414. — DOI: 10.1016/j.mam.2008.07.002
- Anglin RES, Samaan Z, Walter SD, McDonald SD (2013). Vitamin D deficiency and depression in adults: systematic review and meta-analysis. British Journal of Psychiatry;202(2):100-107. — DOI: 10.1192/bjp.bp.111.106666
- Manson JE, Cook NR, Lee IM, Christen W, Bassuk SS, et al. (2019). Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease (VITAL trial). New England Journal of Medicine;380(1):33-44. — DOI: 10.1056/NEJMoa1809944
PubMed Topic Searches
- PubMed — Vitamin D deficiency: diagnosis and management
- PubMed — Osteomalacia and vitamin D deficiency in adults
- PubMed — Nutritional rickets in children
- PubMed — Vitamin D, muscle weakness, and falls in older adults
- PubMed — 25-hydroxyvitamin D screening and supplementation
Connections
- Vitamin D Deficiency: Bone Pain & Osteomalacia
- Vitamin D Deficiency: Rickets in Children
- Vitamin D Deficiency: Muscle Weakness & Falls
- Vitamin D Deficiency: Fatigue & Low Mood
- Vitamin D3 Overview
- Vitamin D Toxicity Hub
- Vitamin D3 Benefits Hub
- Vitamin D and Bone Health
- Vitamin D and Immune Function
- Vitamin D and Mood
- Vitamin D3 Food Sources
- Vitamin D Test (25-Hydroxyvitamin D)
- Calcium
- Phosphorus
- Magnesium
- Hyperparathyroidism
- Fatigue
- Salmon
- Sardines
- Cod
- Eggs