Vitamin D3 for Bone Health & Fracture Prevention
Bone health is the classical — and best-established — indication for vitamin D3. The fundamental mechanism is that calcitriol (the active hormonal form) drives the transcription of calbindin-D9k and TRPV6 in the intestinal brush border, which raises dietary calcium absorption from 10-15% to 30-40%. Without adequate D3, even abundant calcium intake cannot reach the bloodstream or be deposited into bone. But the picture is more nuanced than the mainstream "calcium + D" framing: D3 alone, given without its three mandatory cofactors (vitamin K2, magnesium, vitamin A), can paradoxically promote arterial calcification and kidney stones. The clinically proven protocol is the quartet: D3 + K2-MK7 + magnesium + adequate calcium from food, with a 25(OH)D target of 40-60 ng/mL for skeletal outcomes. This deep-dive walks through the Bischoff-Ferrari fracture meta-analyses, the calbindin/TRPV6/PTH/RANKL-OPG mechanism stack, and the practical protocol for osteoporosis prevention and reversal.
Table of Contents
- Why D3 Is the Foundation of Bone Health
- The Calbindin / TRPV6 Intestinal Absorption Mechanism
- PTH Suppression and Secondary Hyperparathyroidism
- RANKL / OPG and Osteoclast Regulation
- The Bischoff-Ferrari Fracture Meta-Analyses
- Fall Prevention and Neuromuscular Function
- The Mandatory Quartet: D3 + K2 + Magnesium + Calcium
- Why K2 Without D3 (or D3 Without K2) Is Incomplete
- 25(OH)D Target Levels for Skeletal Outcomes
- Practical Osteoporosis Protocol
- Cautions
- Key Research Papers
- Connections
- Featured Videos
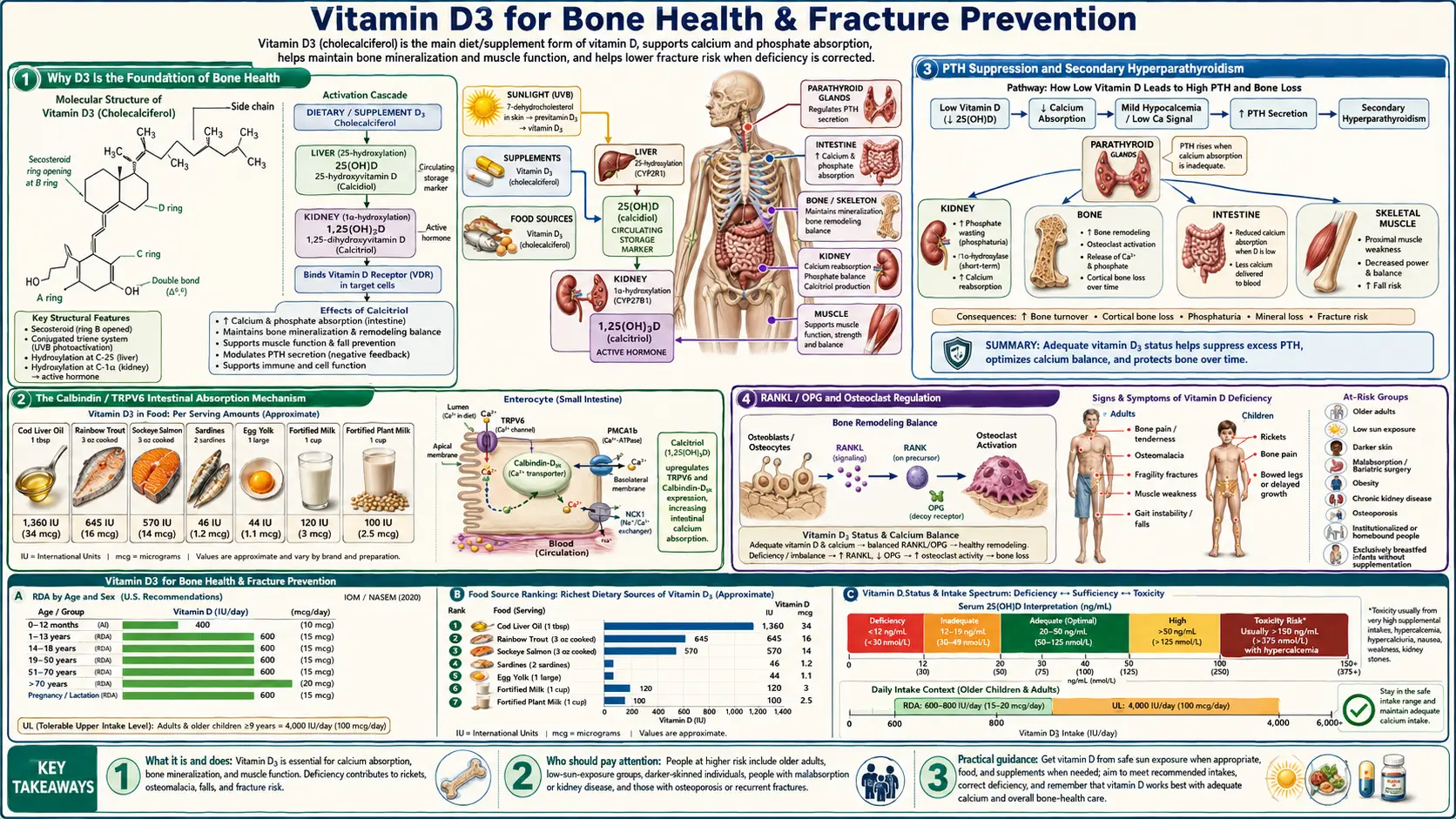
Why D3 Is the Foundation of Bone Health
The skeletal system is in constant turnover — an adult human replaces approximately 10% of skeletal mass every year through the coordinated activity of osteoblasts (bone-forming cells) and osteoclasts (bone-resorbing cells). For osteoblasts to deposit hydroxyapatite crystals into the collagen matrix, two raw materials must be present in adequate concentrations in the extracellular fluid: calcium and phosphorus. Vitamin D3 is the master regulator of both.
Severe D3 deficiency in children produces rickets — bowed legs, widened wrists, frontal bossing of the skull, delayed fontanelle closure, dental defects. Severe deficiency in adults produces osteomalacia, the soft-bone equivalent that often presents as diffuse bone pain and proximal muscle weakness that is misdiagnosed as fibromyalgia. Modest D3 deficiency over decades produces osteoporosis — the progressive loss of bone mineral density that culminates in fragility fractures of the hip, spine, and wrist.
Hip fractures in particular are catastrophic events: roughly 20% of patients over 65 die within one year of a hip fracture, and a substantial fraction of survivors never regain prior mobility. Preventing the fracture in the first place is one of the highest-leverage interventions in geriatric medicine, and adequate vitamin D status is the most cost-effective component of that prevention.
For the broader clinical picture of bone disease, see our Osteoporosis page. For the synergistic partners, see Vitamin K and Magnesium.
The Calbindin / TRPV6 Intestinal Absorption Mechanism
Dietary calcium is absorbed in the small intestine through two parallel pathways:
- Paracellular (passive) absorption — calcium ions diffuse between enterocytes through tight junctions. This pathway accounts for absorption when dietary calcium is abundant but is unregulated — the gut absorbs only what passively diffuses.
- Transcellular (active) absorption — calcium enters enterocytes through the apical TRPV6 calcium channel, is shuttled across the cell bound to calbindin-D9k (which prevents toxic intracellular calcium accumulation), and is extruded across the basolateral membrane by the PMCA1b plasma membrane Ca-ATPase and the NCX1 Na/Ca exchanger. This pathway is the one that is upregulated by calcitriol.
Calcitriol binds its nuclear receptor (VDR), which heterodimerizes with the Retinoid X Receptor (RXR) and binds Vitamin D Response Elements (VDREs) in the promoter regions of the genes encoding calbindin-D9k, TRPV6, PMCA1b, and the basolateral exchanger. Within hours of vitamin D action, transcription of all four genes increases dramatically, and the intestinal absorption efficiency of dietary calcium rises from a baseline of roughly 10-15% (in vitamin D deficiency) to 30-40% (in repletion).
This is why "take more calcium" without addressing vitamin D status is largely futile. A 1,500 mg dietary calcium intake in a deficient individual delivers only 150-225 mg of absorbed calcium to the bloodstream. The same intake in a vitamin D-replete individual delivers 450-600 mg — a three- to four-fold increase from the identical diet, achieved entirely through gene-expression changes in the intestinal epithelium.
The phosphorus story is parallel: calcitriol upregulates the NaPi-IIb sodium-phosphate cotransporter in the intestinal brush border, improving phosphate absorption. Adequate serum phosphate is critical because hydroxyapatite, the mineral phase of bone, is calcium-phosphate.
PTH Suppression and Secondary Hyperparathyroidism
The parathyroid glands continuously sample blood calcium and adjust the secretion of parathyroid hormone (PTH) to maintain serum calcium within a narrow range. When blood calcium falls (because dietary absorption is inadequate from D3 deficiency), PTH rises — and PTH mobilizes calcium from bone to restore blood levels.
This is a critical adaptive mechanism for acute calcium emergencies, but when it operates chronically — as in long-standing D3 deficiency — it produces secondary hyperparathyroidism, a state in which PTH is chronically elevated and bone is steadily being decalcified to maintain blood calcium. This is one of the principal mechanisms by which vitamin D deficiency drives osteoporosis.
Vitamin D3 suppresses PTH through two mechanisms: directly via VDR-mediated repression of the PTH gene in parathyroid cells, and indirectly by raising blood calcium so the calcium-sensing receptor on parathyroid cells signals "calcium is adequate, stand down." Restoring 25(OH)D to the 30-50 ng/mL range typically brings PTH from the elevated 80-150 pg/mL range (secondary hyperparathyroidism) down to the desirable 20-40 pg/mL range within 8-16 weeks.
Clinically, the response of PTH to D3 repletion is one of the better biomarkers of "adequate" vitamin D status — when PTH stops dropping with additional D3, the body is signaling that bone-relevant D3 sufficiency has been reached.
RANKL / OPG and Osteoclast Regulation
Bone turnover is governed by the balance between two cytokines produced by osteoblasts:
- RANKL (Receptor Activator of NF-κB Ligand) — activates osteoclasts, driving bone resorption
- OPG (osteoprotegerin) — a decoy receptor that binds RANKL and prevents it from activating osteoclasts, slowing bone resorption
The ratio of RANKL to OPG determines whether bone is in net resorption (RANKL dominant) or in net building (OPG dominant). Calcitriol has complex, context-dependent effects on this axis: in conditions of dietary calcium scarcity, calcitriol upregulates RANKL to mobilize calcium from bone (an evolved emergency mechanism). In conditions of calcium sufficiency, calcitriol shifts the ratio toward OPG, favoring bone preservation.
The clinical implication is that vitamin D supplementation produces the best bone outcomes when calcium intake is also adequate — isolated D3 supplementation in calcium-deficient individuals can theoretically accelerate bone loss through inappropriate RANKL upregulation. The clinical evidence (especially the WHI calcium-and-D trials) supports the calcium-and-D combination as bone-protective; D3 monotherapy is harder to interpret.
This is also one mechanism by which the calcium-K2-D3 combination outperforms calcium-D3 alone: K2 activates osteocalcin, which directs calcium into the hydroxyapatite matrix, biasing the system toward bone building rather than serum calcium maintenance.
The Bischoff-Ferrari Fracture Meta-Analyses
Heike Bischoff-Ferrari (Zurich) is the principal investigator who established the modern dose-response evidence for vitamin D in fracture prevention. Two pivotal meta-analyses anchor the literature:
Bischoff-Ferrari 2009 (Archives of Internal Medicine)
Pooled analysis of 12 double-blind RCTs of vitamin D supplementation for nonvertebral fracture prevention. The key finding was a clear dose-response: low-dose vitamin D (400 IU/day, the doses used in older trials) produced no significant fracture reduction. Higher-dose vitamin D (482-770 IU/day, with achieved 25(OH)D of approximately 30 ng/mL or higher) produced a 20% reduction in nonvertebral fractures and a 18% reduction in hip fractures.
This meta-analysis was clinically important because it explained the apparent contradiction in earlier literature: trials using inadequate doses (and not measuring achieved 25(OH)D levels) had produced null results that led clinicians to dismiss D3 supplementation, while adequate-dose trials consistently showed fracture reduction.
Bischoff-Ferrari 2012 (NEJM)
Individual-patient-data pooled analysis of 11 RCTs (n = 31,022). Subjects in the highest tertile of achieved vitamin D intake (median 800 IU/day) had a 30% reduction in hip fracture and a 14% reduction in any nonvertebral fracture compared to placebo. The lower two tertiles showed no significant benefit. This established 800 IU/day as the minimum effective dose for fracture prevention in older adults — well above the conventional 400 IU recommendation.
Subsequent work has refined this further: achieved 25(OH)D of 30-44 ng/mL is associated with the lowest hip fracture risk, and the relationship plateaus above 44 ng/mL. This is the basis for the 40-60 ng/mL target range now used in integrative practice for bone outcomes.
Fall Prevention and Neuromuscular Function
Hip fractures in the elderly are not purely a bone-fragility phenomenon — they require both fragile bone and a fall. Vitamin D contributes to fracture prevention through both mechanisms: it strengthens bone (the mechanism discussed above) and it reduces fall risk by improving neuromuscular function.
VDRs are expressed in skeletal muscle, and calcitriol directly regulates muscle protein synthesis and intramuscular calcium handling. Vitamin D deficiency produces proximal muscle weakness — difficulty rising from a chair, climbing stairs, or maintaining single-leg balance. These deficits are subtle, often attributed to aging, and reversible with D3 repletion.
Meta-analyses of fall prevention trials show that vitamin D supplementation (700-1000 IU/day) reduces fall risk by approximately 20% in community-dwelling older adults. The effect is more pronounced in those starting from lower baseline 25(OH)D levels. The mechanism is improvement in lower-extremity strength, postural sway, and reaction time — all VDR-dependent in muscle.
The combined effect of fracture-reduction (bone strengthening) plus fall-reduction (muscle strengthening) is why vitamin D is one of the few single interventions that demonstrably reduces hip fracture in randomized trials.
The Mandatory Quartet: D3 + K2 + Magnesium + Calcium
Isolated vitamin D supplementation, while better than nothing, is suboptimal and carries some risk. The clinically validated bone-protective protocol is a quartet:
| Nutrient | Role | Typical Dose |
|---|---|---|
| Vitamin D3 | Drives intestinal calcium absorption (calbindin/TRPV6), suppresses PTH, supports muscle function | 2,000-5,000 IU/day |
| Vitamin K2 (MK-7) | Activates osteocalcin (directs calcium into bone) and matrix Gla protein (keeps calcium out of arteries) | 100-200 mcg/day |
| Magnesium | Cofactor for the enzymes that hydroxylate D3 to 25(OH)D and 1,25(OH)2D; cofactor for osteoblast function | 300-500 mg/day elemental (glycinate or citrate) |
| Calcium | Raw material for hydroxyapatite; ideally from food (dairy, leafy greens, sardines, almonds) | 1,000-1,200 mg/day total intake (food preferred over supplements) |
A fifth nutrient, boron, deserves mention — it influences vitamin D metabolism and bone matrix protein activity. Trace amounts (3-10 mg/day) from prunes, raisins, almonds, and avocados are typically sufficient; supplementation is rarely required.
Why K2 Without D3 (or D3 Without K2) Is Incomplete
Vitamin K2 (the menaquinone family, most studied as MK-4 from animal foods and MK-7 from fermented foods like natto) is the activator of two Gla-protein enzymes critical to bone and cardiovascular health:
- Osteocalcin — produced by osteoblasts; when K2-activated (carboxylated), it binds calcium and directs it into the hydroxyapatite matrix of bone
- Matrix Gla Protein (MGP) — produced by vascular smooth muscle cells; when K2-activated, it prevents calcium deposition in arterial walls
Both osteocalcin and MGP are produced at rates that depend on vitamin D — calcitriol upregulates their gene transcription — but they are activated by vitamin K2-dependent carboxylation. In K2 deficiency, osteocalcin and MGP are produced but remain inactive (uncarboxylated), so the calcium that D3 brought across the intestinal epithelium has nowhere to go: it accumulates in soft tissues and arterial walls rather than being deposited into bone.
This is the mechanistic basis for the observation that isolated vitamin D supplementation, especially at high doses, is associated with increased arterial calcification in some studies. The Rotterdam Study and other epidemiological data show that high K2 intake (especially MK-7) is associated with significantly reduced cardiovascular mortality and reduced arterial calcification — effects that are likely synergistic with vitamin D rather than independent of it.
The clinical takeaway: never supplement high-dose D3 without K2-MK7 co-administration. The typical ratio is 100-200 mcg MK-7 per 2,000-5,000 IU of D3. For very high D3 doses (10,000+ IU/day as used in the Coimbra autoimmune protocol), K2 dosing scales up proportionally.
25(OH)D Target Levels for Skeletal Outcomes
| 25(OH)D Range | Bone-Relevant Interpretation |
|---|---|
| < 20 ng/mL (50 nmol/L) | Deficient. Risk of rickets in children, osteomalacia in adults, secondary hyperparathyroidism, accelerated bone loss. |
| 20-29 ng/mL (50-72 nmol/L) | Insufficient. PTH may still be inappropriately elevated; calcium absorption is suboptimal. |
| 30-39 ng/mL (75-97 nmol/L) | Conventional sufficiency. The Endocrine Society and most fracture-prevention trials use this as the minimum target. |
| 40-60 ng/mL (100-150 nmol/L) | Optimal for skeletal outcomes. Bischoff-Ferrari data show fracture risk plateaus in this range. PTH fully suppressed. Active calcium absorption maximal. |
| 60-100 ng/mL (150-250 nmol/L) | Higher than needed for bone alone; may be targeted for immune or autoimmune indications. Monitor calcium. |
| > 100 ng/mL (250 nmol/L) | Risk of hypercalcemia rises; reduce dose unless under specialist supervision. |
Test 25(OH)D (not 1,25(OH)2D — that test is essentially never appropriate for assessing vitamin D status). See the Vitamin D Test page for ordering and interpretation guidance.
Practical Osteoporosis Protocol
Assessment
- Baseline 25(OH)D level (target 40-60 ng/mL for bone)
- PTH level (target 20-40 pg/mL; elevated PTH suggests vitamin D inadequacy even if 25(OH)D appears borderline-adequate)
- Serum calcium, phosphorus, magnesium
- DEXA scan for baseline bone mineral density (T-score)
- If T-score < -2.5: osteoporosis. If T-score -1.0 to -2.5: osteopenia.
Repletion phase (12-16 weeks)
- Vitamin D3: 5,000 IU/day (more if BMI > 30; consider 10,000 IU/day for severe deficiency)
- Vitamin K2 (MK-7): 200 mcg/day
- Magnesium glycinate or citrate: 400 mg elemental at bedtime
- Dietary calcium: 1,000-1,200 mg/day from sardines, dairy (if tolerated), almonds, leafy greens, calcium-set tofu
- Re-test 25(OH)D and PTH at 12 weeks
Maintenance phase (indefinite)
- Vitamin D3: 2,000-4,000 IU/day to maintain 25(OH)D in 40-60 ng/mL range; periodic monitoring
- Vitamin K2 (MK-7): 100-200 mcg/day indefinitely
- Magnesium: 300-400 mg/day elemental
- Continued calcium-rich diet
- Weight-bearing exercise (essential for the mechanical signaling that drives osteoblast activity); resistance training 2-3x/week
- Annual 25(OH)D and PTH; DEXA every 1-2 years to track BMD trajectory
When to consider pharmaceutical bone agents
Patients with established osteoporosis (T-score < -2.5), prior fragility fractures, or rapid bone loss should usually receive the quartet protocol plus a pharmaceutical agent (bisphosphonate, denosumab, teriparatide, or romosozumab depending on context). The quartet is complementary to these drugs, not a substitute — bisphosphonates work poorly in vitamin D-deficient patients, and many "bisphosphonate failures" are actually vitamin D failures.
Cautions
- Hypercalcemia at high doses — the principal toxicity of D3 supplementation. Typically requires sustained intake above 10,000-40,000 IU/day for weeks to months, but individual susceptibility varies. Monitor serum calcium periodically at doses above 5,000 IU/day, and at any dose if symptoms of hypercalcemia develop (nausea, polyuria, polydipsia, confusion, kidney stones).
- Sarcoidosis and other granulomatous diseases — macrophages in granulomatous tissue express extrarenal 1α-hydroxylase and convert 25(OH)D to calcitriol without normal feedback regulation. These patients can develop hypercalcemia at modest D3 intakes and should be supplemented only under specialist supervision with frequent calcium and 25(OH)D monitoring.
- Williams syndrome, idiopathic infantile hypercalcemia — rare genetic disorders causing exaggerated calcium response to D3. Standard pediatric D3 doses can be toxic.
- Drug interactions:
- Thiazide diuretics reduce calcium excretion — can predispose to hypercalcemia in D3-supplemented patients
- Glucocorticoids accelerate D3 catabolism (long-term steroid users typically need higher D3 doses)
- Anticonvulsants (phenytoin, phenobarbital, carbamazepine) induce hepatic CYP enzymes and accelerate D3 metabolism
- Rifampin similarly accelerates D3 metabolism
- Bile acid sequestrants (cholestyramine, colestipol) and orlistat reduce D3 absorption (separate dosing by 4+ hours)
- Cardiac glycosides (digoxin) interact with hypercalcemia — arrhythmia risk if D3-induced hypercalcemia develops in a digoxin patient
- Kidney disease — impaired renal 1α-hydroxylation may require calcitriol or its analogues (paricalcitol, doxercalciferol) rather than D3
- K2 caution with warfarin — vitamin K antagonizes warfarin's anticoagulant effect. Patients on warfarin who add K2 should have INR monitored and warfarin dose adjusted; the K2 dose should be kept stable rather than oscillating
Key Research Papers
- Bischoff-Ferrari HA, Willett WC, Wong JB, et al. (2009). Prevention of nonvertebral fractures with oral vitamin D and dose dependency: a meta-analysis of randomized controlled trials. Archives of Internal Medicine. — PubMed
- Bischoff-Ferrari HA et al. (2012). A pooled analysis of vitamin D dose requirements for fracture prevention. NEJM 367:40-49. — PubMed
- Holick MF (2007). Vitamin D deficiency. NEJM 357:266-281. — PubMed
- Bouillon R, Marcocci C, Carmeliet G, et al. (2019). Skeletal and extraskeletal actions of vitamin D: current evidence and outstanding questions. Endocrine Reviews. — PubMed
- Christakos S, Dhawan P, Verstuyf A, Verlinden L, Carmeliet G (2016). Vitamin D: metabolism, molecular mechanism of action, and pleiotropic effects. Physiological Reviews. — PubMed
- Lips P, van Schoor NM (2011). The effect of vitamin D on bone and osteoporosis. Best Pract Res Clin Endocrinol Metab. — PubMed
- Knapen MHJ et al. Three-year low-dose menaquinone-7 (MK-7) supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporosis International. — PubMed
- Schurgers LJ et al. Vitamin K-containing dietary supplements: comparison of synthetic vitamin K1 and natto-derived menaquinone-7. Blood. — PubMed
- Uwitonze AM, Razzaque MS (2018). Role of magnesium in vitamin D activation and function. J Am Osteopath Assoc. — PubMed
- Cranney A, Horsley T, O'Donnell S, et al. (2007). Effectiveness and safety of vitamin D in relation to bone health. AHRQ Evidence Report. — PubMed
- Hollick MF, Binkley NC, Bischoff-Ferrari HA, et al. (2011). Evaluation, treatment, and prevention of vitamin D deficiency: Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. — PubMed
- Bischoff-Ferrari HA et al. (2009). Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. BMJ. — PubMed
PubMed Topic Searches
- PubMed: vitamin D osteoporosis fracture prevention
- PubMed: vitamin D + K2 (MK-7) bone synergy
- PubMed: calbindin/TRPV6 intestinal calcium absorption
- PubMed: magnesium vitamin D hydroxylation cofactor
- PubMed: vitamin D PTH secondary hyperparathyroidism
Connections
- Vitamin D3 Overview
- D3 Benefits Hub
- D3 for Immune Function
- D3 for Autoimmune Disease
- D3 for Mood & Depression
- Vitamin K (essential partner)
- Vitamin A
- Magnesium (essential cofactor)
- Calcium
- Phosphorus
- Boron
- Osteoporosis
- Vitamin D Test
- All Vitamins
- All Minerals