Thiamine Deficiency (Beriberi): Symptoms, Causes, and Recovery
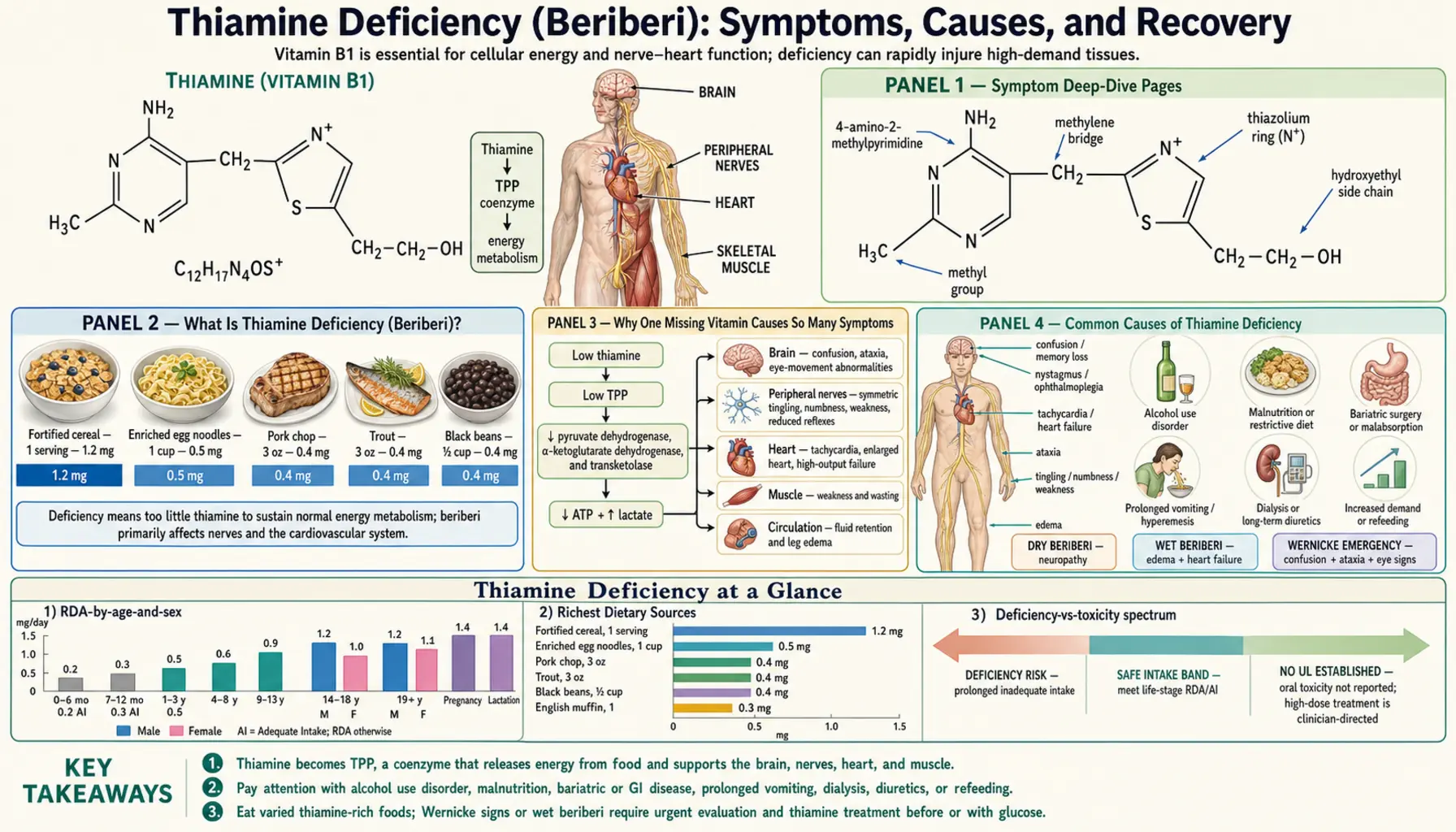
Thiamine deficiency means the body has run short of vitamin B1 — and because B1 is the spark that lets cells turn food into usable energy, the shortage can show up almost anywhere. The classic disease it causes is called beriberi, a word from Sinhalese that doubles as "I cannot, I cannot," capturing the profound weakness it brings. Thiamine deficiency wears several faces: wet beriberi floods the heart and legs (high-output heart failure and swelling); dry beriberi attacks the nerves (numbness, tingling, and weakness in the feet and legs); and Wernicke-Korsakoff syndrome strikes the brain (confusion, unsteady walking, eye-movement problems, and, if untreated, lasting memory loss). Long before any of these, the earliest signs are quiet and easy to dismiss — fatigue, loss of appetite, irritability, and a vague heaviness. The reason one missing vitamin produces such scattered trouble is that thiamine powers a handful of enzymes at the very center of how every cell — especially energy-hungry heart and brain cells — makes fuel. The encouraging part: thiamine is cheap, and when deficiency is caught and treated early, many symptoms reverse strikingly fast, sometimes within hours for the heart and days for the nerves. This hub explains what thiamine deficiency is, why one shortage causes so many different problems, who is at risk, how it is diagnosed, and exactly how it is corrected — with deep-dive pages for each of the major forms.
Symptom Deep-Dive Pages
Wet Beriberi (Heart)
How thiamine deficiency overworks and weakens the heart, producing high-output heart failure, breathlessness, and swelling in the legs — plus the dramatic "Shoshin" emergency and how fast it can respond to treatment.
Dry Beriberi (Nerves)
Why low thiamine damages the longest nerves first, causing burning, numbness, and tingling in the feet and progressive weakness in the legs — the symmetrical peripheral neuropathy of beriberi.
Wernicke-Korsakoff Syndrome
The brain emergency of thiamine deficiency: confusion, an unsteady walk, and abnormal eye movements that, untreated, can collapse into permanent amnesia. Why it is so often missed and why treatment cannot wait.
Fatigue & Appetite Loss
The earliest, easiest-to-miss signs: deep tiredness, loss of appetite, irritability, and a heavy, run-down feeling — what they mean, why they are non-specific, and when they should prompt a check for thiamine.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Thiamine Deficiency (Beriberi)?
- Why One Missing Vitamin Causes So Many Symptoms
- Common Causes of Thiamine Deficiency
- Who Is Most at Risk
- How Thiamine Deficiency Is Diagnosed
- How Thiamine Deficiency Is Corrected
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Is Thiamine Deficiency (Beriberi)?
Thiamine, also called vitamin B1, is a water-soluble vitamin the body cannot make and stores only in small amounts — roughly 25 to 30 milligrams total, enough for only about two to three weeks if intake stops completely. When the supply runs short, the resulting illness is called beriberi. The word comes from Sinhalese and is usually translated as "I cannot, I cannot," a fitting name for a disease whose hallmark is overwhelming weakness. Beriberi was once one of the great scourges of rice-eating populations, and the search for its cause — eventually traced to something missing from polished white rice rather than a germ or a poison — helped launch the entire science of vitamins.
Doctors describe thiamine deficiency in several recognizable forms, though they overlap and a person can have more than one at once:
- Dry beriberi — the nervous-system form. It produces a symmetrical peripheral neuropathy: burning, numbness, "pins and needles," and aching that usually starts in the feet and creeps upward, along with progressive weakness, especially in the legs. People may notice they stumble, struggle to rise from a squat, or develop a high-stepping "foot drop." The deep-dive page is Dry Beriberi (Nerves).
- Wet beriberi — the cardiovascular form. "Wet" refers to the fluid build-up (edema) that swells the legs and, in severe cases, the lungs. The heart is forced to pump a very large volume of blood (so-called high-output heart failure), causing a fast heartbeat, breathlessness, and swelling. Its most extreme, sudden, life-threatening version is called Shoshin beriberi. The deep-dive page is Wet Beriberi (Heart).
- Wernicke-Korsakoff syndrome — the brain form, sometimes called "cerebral beriberi." Wernicke encephalopathy is the acute, reversible phase: a classic triad of confusion, an unsteady wide-based walk (ataxia), and abnormal eye movements (such as jerking eyes or a paralyzed gaze). If thiamine is not given quickly, it can progress to Korsakoff syndrome, a often-permanent memory disorder. The deep-dive page is Wernicke-Korsakoff Syndrome.
- Infantile beriberi — affects breastfed babies of thiamine-deficient mothers, sometimes appearing suddenly with heart failure, a hoarse or silent cry, and vomiting. (See the related page Infantile Thiamine Deficiency.)
Before any of these dramatic syndromes appear, deficiency usually announces itself quietly. The earliest signs are non-specific: fatigue, loss of appetite, nausea, irritability, poor concentration, and a vague run-down feeling — symptoms so common and so easily blamed on stress or overwork that thiamine is rarely the first thing anyone suspects. That early, easy-to-miss stage is covered on the Fatigue & Appetite Loss page.
One crucial point frames everything that follows: thiamine deficiency is a clinical diagnosis, treated on suspicion. Blood tests for thiamine exist but are slow and imperfect, so when the picture fits — especially the brain form — doctors give thiamine immediately rather than wait for confirmation. The downside of giving thiamine to someone who turns out not to need it is essentially nothing; the downside of withholding it from someone who does can be permanent brain damage or death.
Why One Missing Vitamin Causes So Many Symptoms
The puzzle of beriberi is how a single missing vitamin can cause troubles as different as a swollen heart, numb feet, and a confused mind. The answer is that thiamine is not a specialist — it is a foundational cofactor sitting at the exact crossroads where cells turn food into energy. When it disappears, the tissues that burn the most fuel feel it first and hardest.
Here is the core idea in everyday language. After your body absorbs thiamine, it converts it into an active form called thiamine pyrophosphate (TPP). TPP is a required helper — a cofactor — for a small group of enzymes that perform the central steps of energy metabolism. Two of them are especially important: pyruvate dehydrogenase, the gate that lets carbohydrate (glucose) enter the cell's main energy furnace, and alpha-ketoglutarate dehydrogenase, a key step inside that furnace (the Krebs cycle). A third, transketolase, runs a separate pathway the body uses to build and repair. Without TPP, these enzymes stall. Pekovich and colleagues showed in human cells that thiamine deficiency directly lowers the activity of transketolase and pyruvate dehydrogenase, confirming the biochemical bottleneck.
Picture thiamine as the key that starts the engine in which cells burn sugar for power. Take the key away and the engine sputters: fuel piles up unburned (lactic acid accumulates, which is why severe deficiency can cause a dangerous lactic acidosis), and the cell cannot make enough ATP, the energy currency that every function depends on. Because the same engine sits behind so many tissues, one missing key is felt in many places at once:
- The heart — cardiac muscle never rests and runs almost entirely on aerobic energy, so it is acutely sensitive to a fuel shortage. Low thiamine also makes the body's blood vessels dilate, forcing the heart to pump an enormous volume to compensate — the high-output failure of wet beriberi. See also Heart Failure.
- Peripheral nerves — the longest nerves in the body (those reaching the feet) must keep their distant tips supplied with energy through a very long axon. They are the first to fail when fuel runs short, producing the foot-first numbness and weakness of dry beriberi. See also Peripheral Neuropathy.
- The brain — certain brain regions around the third ventricle and brainstem have an unusually high metabolic demand and depend heavily on thiamine-driven enzymes; when those falter, the result is the confusion, unsteadiness, and eye-movement problems of Wernicke-Korsakoff syndrome.
- Whole-body energy — because every cell relies on this pathway to some degree, the earliest and most universal symptom is simply a failure to make enough energy: profound fatigue and loss of appetite.
This is the unifying theme to carry into the symptom pages: there is nothing mysterious about thiamine deficiency producing such a scattershot of problems. One vitamin powers the engine of energy production in many tissues, so one shortage is felt wherever the energy demand is highest.
Common Causes of Thiamine Deficiency
Thiamine runs low for one of three broad reasons: you are taking in too little, you are losing or breaking down too much, or your body's demand has outstripped its supply. Often several push in the same direction at once. Here are the causes worth knowing.
- Heavy alcohol use — by far the most common cause in wealthy countries. Alcohol hits thiamine three ways: it displaces nourishing food, it directly blocks thiamine absorption in the gut, and it impairs the liver's ability to store and activate the vitamin. This is why thiamine deficiency and its brain form are so strongly linked to alcohol-use disorder.
- A diet built on polished (white) rice or refined carbohydrate — the original cause of epidemic beriberi. Milling rice strips away the thiamine-rich outer layers; a diet of mostly white rice, refined flour, or sugar delivers carbohydrate that requires thiamine to burn while supplying almost none, a double blow. Beriberi still appears today where polished rice dominates the diet.
- Vomiting, especially severe pregnancy sickness — persistent vomiting both empties out intake and is a recognized trigger of Wernicke encephalopathy. Hyperemesis gravidarum (severe morning sickness) is a classic, dangerous, and very treatable cause in pregnancy.
- Bariatric (weight-loss) surgery and gut malabsorption — operations that bypass or shrink the stomach and upper intestine, as well as conditions like chronic diarrhea, Crohn's disease, and short-bowel syndrome, reduce how much thiamine the body can absorb. Wernicke encephalopathy after bariatric surgery is well documented, often when vomiting compounds the problem.
- Long-term diuretics ("water pills") — loop diuretics such as furosemide, widely used for heart failure, flush thiamine out in the urine. Sica reviewed this loop-diuretic–thiamine link in heart-failure patients; the irony is sharp, because thiamine deficiency can itself worsen the very heart failure being treated.
- Refeeding after starvation — when a malnourished person suddenly resumes eating (especially carbohydrate), the surge of metabolism demands a flood of thiamine the depleted body cannot supply, and deficiency can crash within hours. This is one strand of the dangerous refeeding syndrome, which is why hospitals give thiamine before and during refeeding.
- Other high-demand states — prolonged critical illness, severe infection, high fever, an overactive thyroid, dialysis, and cancer all raise metabolic demand or increase losses. Giving IV sugar (dextrose) to a depleted patient without thiamine can actually precipitate Wernicke encephalopathy by suddenly demanding thiamine to burn that sugar — which is why thiamine is given first.
- Poor diet in older adults — reduced appetite, limited variety, and chronic illness make marginal thiamine intake common in the elderly, and O'Keeffe has highlighted how easily it is overlooked in this group.
A practical note: these causes combine. An older adult on a loop diuretic for heart failure who has been eating poorly and then catches a vomiting illness can become deeply thiamine-deficient from the sum of several modest losses pushing the same way.
Who Is Most at Risk
Anyone can become thiamine-deficient, but several groups are far more vulnerable. Recognizing yourself or a loved one here is reason to make sure thiamine intake is solid — and reason for a doctor to keep the diagnosis in mind.
- People with alcohol-use disorder — the single largest risk group in wealthy countries, because alcohol attacks thiamine from every angle. Anyone drinking heavily who develops confusion, unsteadiness, or eye-movement changes should be treated for Wernicke encephalopathy without delay.
- Pregnant people with severe vomiting — hyperemesis gravidarum can deplete thiamine quickly; Wernicke encephalopathy in pregnancy is rare but devastating and entirely preventable with thiamine.
- People after bariatric surgery — especially in the first months, and especially if they are vomiting or not taking their supplements. This is a growing source of cases as weight-loss surgery becomes more common.
- Older adults — through poor appetite, restricted diets, multiple medications (including diuretics), and chronic illness.
- People with heart failure on long-term loop diuretics — both from urinary thiamine losses and from the poor appetite that often accompanies the illness.
- People with chronic gut disease or malabsorption — Crohn's disease, chronic diarrhea, recurrent vomiting, or short-bowel syndrome.
- People who are critically ill or recovering from starvation — including those with eating disorders, prolonged fasting, or anyone being refed after a period of poor intake.
- Populations eating mostly polished rice or refined carbohydrate — where dietary beriberi still occurs, including in some refugee and food-insecure settings.
- Breastfed infants of thiamine-deficient mothers — infantile beriberi can appear suddenly and is a medical emergency (see Infantile Thiamine Deficiency).
If you are in one of these groups, the reassuring news is that prevention is simple and cheap: a balanced diet, or a routine B-vitamin or thiamine supplement when intake or absorption is uncertain. The food sources page lists the best dietary sources.
How Thiamine Deficiency Is Diagnosed
The most important fact about diagnosing thiamine deficiency is also the most counter-intuitive: it is usually diagnosed and treated on clinical suspicion, not on a blood test. The reason is timing. The brain form (Wernicke encephalopathy) can cause irreversible damage within days, while laboratory tests for thiamine are not available quickly in most hospitals and are imperfect even when they are. So when the story fits — an at-risk person with confusion, unsteadiness, abnormal eye movements, unexplained heart failure, or a neuropathy — doctors give thiamine first and confirm later. Major guidelines, including the European Federation of Neurological Societies guideline by Galvin and colleagues, stress treating on suspicion precisely because the test is too slow to rely on.
That said, testing has a role, especially to confirm a diagnosis after treatment has begun or to investigate a less urgent case. The tools include:
- Blood thiamine tests — the most useful is a measurement of thiamine diphosphate (TDP, the active form) in whole blood or red cells, usually by a method called HPLC. A simpler "erythrocyte transketolase activity" test, which measures how much an enzyme speeds up when extra thiamine is added, is an older functional marker. These tests are helpful but are sent to specialized labs and take time — which is exactly why treatment should not wait for them.
- The response to treatment itself — one of the most telling "tests" is how the person responds. In wet beriberi, the heart can improve dramatically within hours of intravenous thiamine; in Wernicke encephalopathy, eye signs often begin to clear within hours to days. A rapid response strongly supports the diagnosis.
- Brain MRI — in suspected Wernicke encephalopathy, an MRI can show characteristic changes in specific deep-brain regions. It supports the diagnosis when positive but does not rule it out when normal — another reason not to withhold treatment.
- Supporting blood work — doctors often check related labs that round out the picture: a high blood lactate (from the metabolic bottleneck), electrolytes including magnesium (frequently low in the same at-risk people; see Magnesium), and a Comprehensive Metabolic Panel to assess organ function and refeeding risk.
An important practical caution: do not give intravenous glucose (dextrose) to an at-risk patient before giving thiamine. A sugar load suddenly increases the demand for thiamine to metabolize it, and in a depleted person this can tip a borderline state into full Wernicke encephalopathy. The standing rule in emergency care is "thiamine before (or with) glucose" in anyone who might be deficient.
How Thiamine Deficiency Is Corrected
Treatment is matched to severity and form, but the unifying principles are simple: replace thiamine promptly and in adequate amounts, give it by the right route, treat the cause, and check for partner deficiencies. Thiamine is remarkably safe even at high doses, so when in doubt, doctors treat.
- Prevention and mild deficiency — food first, then a supplement. The Recommended Dietary Allowance for adults is modest — about 1.2 mg per day for men and 1.1 mg per day for women (slightly higher, around 1.4 mg, in pregnancy and breastfeeding). These amounts are easily met by a varied diet. Good sources include pork (one of the richest), oats and other whole grains, lentils and beans, fortified cereals and breads, nuts and seeds, and eggs. See the Thiamine Food Sources page for fuller details. For people with marginal intake, an inexpensive oral B-vitamin or thiamine supplement closes the gap.
- Established or symptomatic deficiency — therapeutic doses, often by injection. When deficiency is causing symptoms, treatment uses doses far above the RDA. Because the deficiency often coexists with poor gut absorption (alcohol, surgery, vomiting), thiamine is frequently given by injection or intravenously at first to guarantee it gets in, then continued orally.
- Suspected Wernicke encephalopathy — high-dose IV thiamine, urgently. This is the situation where speed matters most. Guidelines such as the EFNS recommendation by Galvin and colleagues call for high-dose intravenous thiamine (commonly cited as around 500 mg three times daily for the first days in established cases, with lower preventive doses for at-risk patients), given before any glucose. Eye signs and confusion often respond within hours to days; the memory loss of Korsakoff syndrome is far less reversible, which is why early, generous treatment is the whole game. Isenberg-Grzeda and colleagues have documented how often the syndrome is under-recognized and under-treated — including outside the alcohol setting, such as in patients with cancer.
- Wet beriberi / Shoshin — can reverse dramatically. In acute cardiac beriberi, intravenous thiamine can produce a striking, sometimes near-miraculous improvement in heart function within hours, which is part of what distinguishes it from other causes of heart failure.
- Always: treat the cause and check partners. Replacing thiamine without addressing why it dropped just resets the clock — that may mean treating alcohol-use disorder, adjusting a diuretic, controlling pregnancy vomiting, or correcting a malabsorption problem. Magnesium is commonly low in the same people and is needed for thiamine to be activated, so it is checked and replaced as part of care. When refeeding a malnourished person, thiamine is given before and during the process to head off refeeding syndrome (Mehanna and colleagues).
For most people the outlook is genuinely good when treatment is not delayed: the heart and the earliest fatigue recover fastest, the nerves recover more slowly over weeks to months (and not always completely if damage was severe and long-standing), and the brain recovers best when thiamine is given before memory loss sets in.
When to Seek Care / Red Flags
Vague early symptoms — tiredness, poor appetite, mild numbness — warrant a non-urgent talk with your doctor, especially if you are in one of the at-risk groups above. But certain symptoms mean thiamine deficiency may be threatening the brain or heart, and these are emergencies. Seek emergency care right away — and say "could this be thiamine deficiency?" — if you or someone you are caring for has any of the following, particularly with heavy alcohol use, severe vomiting, recent weight-loss surgery, or poor nutrition:
- New confusion, disorientation, or a sudden change in mental state — the leading sign of Wernicke encephalopathy, which is a true emergency because delay can cause permanent memory loss.
- An unsteady, staggering, wide-based walk — especially when it appears over days and cannot be explained by intoxication alone.
- Abnormal eye movements or double vision — jerking eyes, a drifting or paralyzed gaze, or sudden double vision.
- Severe shortness of breath, a racing heart, or rapid swelling of the legs — possible high-output heart failure of wet beriberi, which can deteriorate quickly. See Heart Failure.
- Rapidly worsening leg weakness or numbness — difficulty walking, standing, or feeling the feet that is progressing over days.
- In a young infant: sudden poor feeding, vomiting, a hoarse or silent cry, fast breathing, or breathlessness — infantile beriberi is a pediatric emergency.
The crucial message for caregivers, especially of someone who drinks heavily or has been vomiting and not eating: thiamine is cheap and safe, and treatment should not wait for a test. If a clinician is uncertain, asking directly whether thiamine should be given can be the question that prevents lasting harm. For the early, non-urgent end of the spectrum, see Fatigue & Appetite Loss.
Key Research Papers
- Sechi G, Serra A (2007). Wernicke's encephalopathy: new clinical settings and recent advances in diagnosis and management. The Lancet Neurology;6(5):442-455. — DOI: 10.1016/S1474-4422(07)70104-7
- Galvin R, Bråthen G, Ivashynka A, Hillbom M, Tanasescu R, Leone MA (2010). EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. European Journal of Neurology;17(12):1408-1418. — DOI: 10.1111/j.1468-1331.2010.03153.x
- Isenberg-Grzeda E, Kutner HE, Nicolson SE (2012). Wernicke-Korsakoff Syndrome: Under-Recognized and Under-Treated. Psychosomatics;53(6):507-516. — DOI: 10.1016/j.psym.2012.04.008
- Isenberg-Grzeda E, Rahane S, DeRosa AP, Ellis J, Nicolson SE (2016). Wernicke-Korsakoff syndrome in patients with cancer: a systematic review. The Lancet Oncology;17(4):e142-e148. — DOI: 10.1016/S1470-2045(16)00037-1
- Marrs C, Lonsdale D (2021). Hiding in Plain Sight: Modern Thiamine Deficiency. Cells;10(10):2595. — DOI: 10.3390/cells10102595
- Cui Y, Zhang Y, et al. (2014). Thiamine Deficiency (Beriberi) Induced Polyneuropathy and Cardiomyopathy: Case Report and Review of the Literature. Journal of Medical Cases;5(8):444-448. — DOI: 10.14740/jmc1780w
- Amiya E, Morita H (2024). Characteristics of Shoshin Beriberi, a Fulminant Cardiovascular Type of Beriberi. International Heart Journal;65(2):171-172. — DOI: 10.1536/ihj.24-034
- Sica DA (2007). Loop Diuretic Therapy, Thiamine Balance, and Heart Failure. Congestive Heart Failure;13(4):244-247. — DOI: 10.1111/j.1527-5299.2007.06260.x
- O'Keeffe ST (2000). Thiamine deficiency in elderly people. Age and Ageing;29(2):99-101. — DOI: 10.1093/ageing/29.2.99
- Pekovich SR, Martin PR, Singleton CK (1998). Thiamine Deficiency Decreases Steady-State Transketolase and Pyruvate Dehydrogenase but not α-Ketoglutarate Dehydrogenase mRNA Levels in Three Human Cell Types. The Journal of Nutrition;128(4):683-687. — DOI: 10.1093/jn/128.4.683
- Mehanna HM, Moledina J, Travis J (2008). Refeeding syndrome: what it is, and how to prevent and treat it. BMJ;336(7659):1495-1498. — DOI: 10.1136/bmj.a301
- National Institutes of Health, Office of Dietary Supplements (2023). Thiamin — Health Professional Fact Sheet. — NIH Office of Dietary Supplements
PubMed Topic Searches
- PubMed — Thiamine deficiency and beriberi: review
- PubMed — Wernicke encephalopathy: diagnosis and treatment
- PubMed — Wet beriberi and high-output heart failure
- PubMed — Thiamine deficiency and peripheral neuropathy
- PubMed — Thiamine deficiency and alcohol-use disorder
Connections
- Wet Beriberi (Heart)
- Dry Beriberi (Nerves)
- Wernicke-Korsakoff Syndrome
- Fatigue & Appetite Loss
- Vitamin B1 Overview
- Vitamin B1 Toxicity
- Vitamin B1 Benefits Hub
- Thiamine Food Sources
- History of Thiamine & Beriberi
- Thiamine and Beriberi
- Thiamine and Brain Health
- Infantile Thiamine Deficiency
- Peripheral Neuropathy
- Heart Failure
- Comprehensive Metabolic Panel
- Magnesium
- Pork
- Oats
- Lentils
- Beans
- Eggs