Infantile Thiamine Deficiency: Wernicke Encephalopathy in Infants
Infantile thiamine deficiency is a distinct clinical entity from the classical adult presentation. Infants depend on a continuous external supply of vitamin B1 because their endogenous stores are small (roughly 25–30 mg total body content at birth) and their basal metabolic rate is two to three times higher per kilogram than that of adults. When supply is interrupted — through a defective infant formula, a thiamine-deficient breastfeeding mother, or an inborn error of thiamine transport — symptoms can appear in days to a few weeks, and the cardiac form (Shoshin beriberi) can kill within hours of cardiovascular collapse. The encephalopathic form produces the classic Wernicke triad of ophthalmoplegia, ataxia, and altered consciousness, but in infants the most visible sign is often esotropia — cross-eyes caused by abducens (cranial nerve VI) palsy. Recognition is a paediatric emergency: IV or IM thiamine must be given empirically, before any confirmatory laboratory test, because every hour of delay multiplies the risk of permanent neurocognitive injury or death.
Table of Contents
- Why Infants Are Uniquely Vulnerable
- Causes of Infantile Thiamine Deficiency
- The Three Clinical Forms
- Cardiac (Shoshin) Form
- Neurological (Aphonic) Form
- Encephalopathic (Wernicke) Form
- Ocular Signs: CN VI Palsy, Esotropia, Nystagmus
- Brain MRI Findings
- Diagnosis — Don't Wait for the Lab
- Emergency Treatment
- Long-Term Sequelae in Survivors
- Prevention
- Research Papers and References
- Connections
- Featured Videos
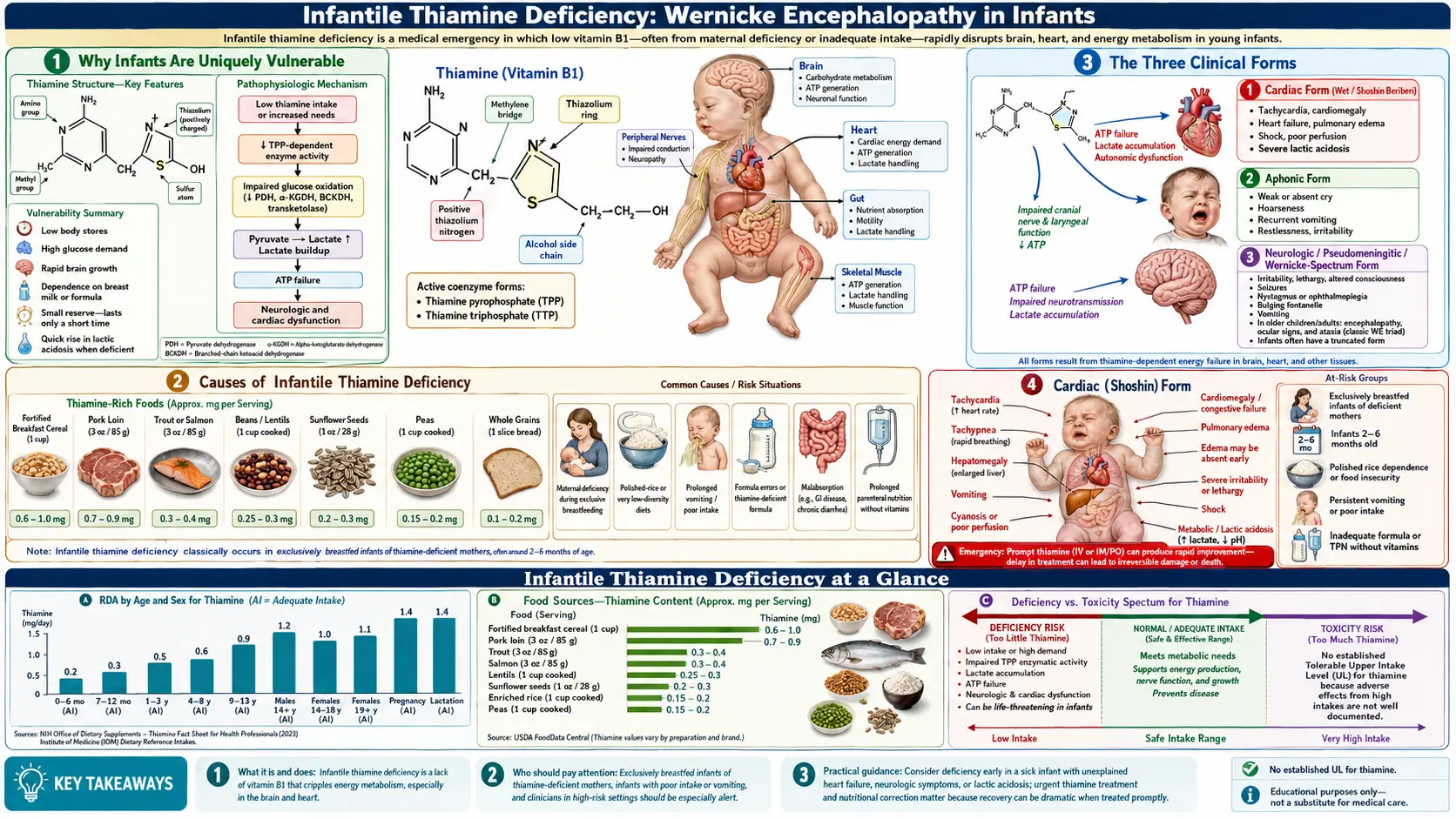
1. Why Infants Are Uniquely Vulnerable
Thiamine pyrophosphate (TPP) is the obligate cofactor for three enzymes that sit at the centre of glucose oxidation: pyruvate dehydrogenase, α-ketoglutarate dehydrogenase, and transketolase. Without TPP, pyruvate cannot enter the Krebs cycle, lactic acid accumulates, and cells that depend on aerobic glucose metabolism — cardiac myocytes and neurons, above all — begin to fail.
- Small total-body stores. A term newborn carries roughly 25–30 mg of thiamine. With a daily turnover of 1–2 mg/day, complete depletion is possible within two to three weeks of zero intake.
- High glucose flux. The infant brain consumes about 60% of resting energy expenditure (versus 20% in adults), and that energy comes almost entirely from glucose. TPP demand per kilogram is therefore highest at this age.
- Rapid myelination. The first 12–24 months are the period of fastest white-matter growth. Thiamine is required for the synthesis of fatty acids that build myelin and for acetylcholine signalling at developing synapses.
- Limited reserve in breast milk. Breast milk reflects maternal thiamine status almost in real time. A mother eating a polished-rice or refined-flour diet, or recovering from hyperemesis gravidarum or bariatric surgery, can produce milk with thiamine far below the infant's daily requirement.
2. Causes of Infantile Thiamine Deficiency
- Defective infant formula. The single most catastrophic cause when it occurs. The 2003 Israeli outbreak from Remedia Super Soya 1 is the canonical modern example: the vitamin premix omitted thiamine, ~20 infants developed life-threatening deficiency, and 2 died of cardiomyopathy.
- Exclusive breastfeeding by a thiamine-deficient mother. Endemic in Karen refugee camps on the Thai–Burma border, in parts of rural Laos and Cambodia where polished white rice dominates the maternal diet, and historically in Japanese coastal populations before fortification. Infant beriberi has been called the leading single cause of infant death in some of these settings.
- Maternal hyperemesis gravidarum. Severe pregnancy vomiting can leave both mother and infant thiamine-depleted at delivery; the deficit accelerates once exclusive breastfeeding begins.
- Maternal bariatric surgery (Roux-en-Y gastric bypass, sleeve gastrectomy) without adequate vitamin replacement.
- Refeeding syndrome in malnourished or premature infants given carbohydrate-rich feeds without prior thiamine supplementation. Glucose loading without thiamine acutely worsens TPP-dependent enzyme failure and can precipitate Wernicke encephalopathy.
- Total parenteral nutrition (TPN) errors. Multivitamin shortages or compounding errors have caused infantile Wernicke in NICU and PICU settings.
- Biotin-thiamine-responsive basal ganglia disease (BTBGD). An autosomal-recessive mutation in SLC19A3 (the thiamine transporter) that mimics acquired deficiency but responds to high-dose oral thiamine plus biotin.
- Thiamine-responsive megaloblastic anaemia (TRMA / Rogers syndrome). Mutation in SLC19A2; presents in infancy with anaemia, sensorineural deafness, and diabetes.
3. The Three Clinical Forms
Infantile thiamine deficiency does not always present as the textbook Wernicke triad. In a cohort of 20 infants in the Remedia outbreak, three distinct presentations were recognized, often blending into one another as the deficit progressed:
- Cardiac (Shoshin) form — hyperacute heart failure with high-output collapse, lactic acidosis, cyanosis. Usually fatal within hours if thiamine is not given.
- Neurological (aphonic) form — insidious onset over days. The earliest and most specific sign is aphonia: a silent or hoarse cry. Hypotonia, lethargy, poor feeding, and vomiting follow.
- Encephalopathic (Wernicke) form — ophthalmoplegia, nystagmus, reduced consciousness, seizures. This is the form that produces the cross-eyed (esotropic) infant whose clinical photograph is widely used in paediatric neurology teaching.
4. Cardiac (Shoshin) Form
Shoshin beriberi takes its name from the Japanese shō (acute) + shin (heart). Onset is sudden and the trajectory is hours, not days.
- Pathophysiology. Cardiac myocytes are second only to neurons in their reliance on TPP-dependent aerobic glucose metabolism. When pyruvate dehydrogenase fails, pyruvate is shunted to lactate, producing severe lactic acidosis. Peripheral vasodilation drives a high-output state that overwhelms a metabolically failing heart.
- Clinical signs. Tachycardia, tachypnoea, cyanosis, hepatomegaly, cardiomegaly on chest film, gallop rhythm, and shock disproportionate to obvious cause. Pulse oximetry can be misleading: the failure is metabolic, not pulmonary.
- Lab clues. Profound lactic acidosis with normal or low pyruvate-to-lactate ratio in early disease; later, the ratio falls further. Cardiac enzymes may be modestly elevated.
- Echocardiogram. Dilated ventricles with depressed systolic function; in early disease, pre-existing structural cause is absent.
- Treatment is a stat dose of IV thiamine (50–100 mg in an infant) given before the diagnosis is confirmed. The cardiac response is often dramatic, with ejection fraction improving within hours. Without thiamine, glucose infusions worsen the picture.
5. Neurological (Aphonic) Form
The aphonic form develops more slowly than the cardiac form but is more easily missed because the early signs are non-specific.
- Aphonia — the infant cries without sound, or with a weak, husky, or hoarse voice. This reflects involvement of the laryngeal nerves (a branch of the vagus). In Lao and Karen refugee paediatric units, an aphonic infant is treated as having beriberi until proven otherwise.
- Hypotonia, head lag, and loss of motor milestones.
- Vomiting and poor feeding, often misattributed to gastroenteritis. Many Remedia infants were initially treated for viral illness.
- Constipation from autonomic dysfunction.
- Pseudo-meningitis presentation — bulging fontanelle, irritability, vomiting, and altered consciousness can mimic bacterial meningitis. Lumbar puncture is typically normal, and the clue is the failure to respond to antibiotics combined with eventual ocular signs.
6. Encephalopathic (Wernicke) Form
The full Wernicke encephalopathy syndrome — ophthalmoplegia, ataxia, and altered consciousness — is present in only about one-third of adult cases at first presentation. In infants, the encephalopathic form is even less complete: ataxia cannot be assessed before walking, and altered consciousness is hard to grade in a six-month-old. The most useful sign at the bedside is therefore the eye examination.
- Reduced level of consciousness — from lethargy to obtundation to coma. May be misread as post-ictal state.
- Seizures in roughly 15–30% of infantile cases. Often focal, often refractory until thiamine is given.
- Hypothermia from hypothalamic involvement.
- Apnoea and bradycardia from brainstem involvement — a terminal sign if untreated.
- Mammillary body and periaqueductal grey damage on MRI (see Section 8) confirms the diagnosis.
7. Ocular Signs: CN VI Palsy, Esotropia, Nystagmus
The eyes are the diagnostic window into infantile Wernicke encephalopathy. The clinical photograph of a cross-eyed, hypotonic infant in arms is iconic in paediatric neurology because the ocular findings appear early, are visually unmistakable, and reverse fastest with treatment.
- Abducens (cranial nerve VI) palsy. CN VI is the longest intracranial nerve and the most vulnerable to metabolic insult. Unilateral or bilateral CN VI palsy produces esotropia — the affected eye cannot abduct, so it sits in a medial (cross-eyed) position at rest. In an infant, the parent often notices "the new cross-eye" before the medical team does.
- Nystagmus. Horizontal or rotary nystagmus is common and reflects vestibular nuclei involvement in the dorsal pons.
- Ophthalmoplegia. In severe cases, additional cranial nerves (III and IV) are involved, producing complete or near-complete external ophthalmoplegia. Pupillary responses are usually preserved, distinguishing the picture from third-nerve compression.
- Ptosis. Bilateral lid droop from CN III involvement.
- Visual loss. Optic atrophy with reduced visual evoked potentials has been reported in long-term Remedia survivors; the lateral geniculate nucleus and visual cortex are both metabolically vulnerable in deficiency.
- Reversibility. Ocular signs typically begin to reverse within hours to a few days of IV thiamine. Persistent esotropia or strabismus beyond a few weeks usually indicates lasting brainstem injury and may need surgical correction.
8. Brain MRI Findings
Brain MRI is the single most useful confirmatory test when thiamine deficiency is suspected. The findings are bilateral, symmetric, and follow the distribution of TPP-dependent metabolism.
- Classic adult sites. Mammillary bodies, periaqueductal grey, dorsomedial thalamus, tectal plate.
- Infantile differences. Kornreich and colleagues, reporting the Remedia cohort, described prominent involvement of the basal ganglia (especially the putamen and caudate), the periaqueductal grey, and the frontal lobe white matter — a distribution that differs from the adult mammillary-body-dominant pattern.
- Signal characteristics. Symmetric T2 / FLAIR hyperintensity, restricted diffusion in the acute phase, with eventual volume loss and gliosis in survivors.
- Mammillary body atrophy on later follow-up MRI is essentially pathognomonic of a remote thiamine deficiency event.
- MR spectroscopy can show an elevated lactate peak in the affected regions, confirming the metabolic origin of the lesions.
9. Diagnosis — Don't Wait for the Lab
Confirmatory laboratory testing exists but is too slow to drive treatment decisions in a hyperacute case. Empirical IV thiamine is both diagnostic (rapid clinical response) and therapeutic.
- Whole-blood thiamine by HPLC — normal range varies by laboratory; values are often dramatically depressed in symptomatic deficiency. Send before the first dose if logistically possible, but never delay treatment for the result.
- Erythrocyte transketolase activity with TPP effect — a TPP activation coefficient >1.25 indicates functional thiamine deficiency. Less commonly available than whole-blood thiamine today.
- Serum / CSF lactate — elevated in both blood and cerebrospinal fluid in active deficiency.
- Brain MRI — the single most useful confirmatory test when the diagnosis is suspected and the infant is stable enough to be scanned.
- Don't load with glucose first. A 10% dextrose bolus in a thiamine-deficient infant accelerates TPP-dependent enzyme failure and can precipitate fulminant Wernicke encephalopathy. Give thiamine before, or at the same time as, any carbohydrate-rich infusion in suspected cases.
10. Emergency Treatment
- IV or IM thiamine 50–100 mg as a single empirical dose at first suspicion, regardless of which clinical form is present. Adverse events from a single parenteral dose are exceedingly rare (anaphylaxis is reported but rare and usually responds to standard management).
- Follow-on dosing. 25–50 mg/day IV/IM for several days, then 10–25 mg/day orally until full recovery and dietary correction.
- Supportive care. Cardiac form — inotropic support, treat lactic acidosis (acidosis usually resolves rapidly once thiamine is on board). Seizures — standard anticonvulsant management; persistent refractory seizures usually settle within 24–48 hours of thiamine.
- Co-supplementation. Other B vitamins (especially B6 and B12), magnesium (a cofactor for converting thiamine to TPP — deficiency can blunt the response), and folate.
- Treat the source. Switch off the offending formula. Test maternal thiamine status if breastfeeding. Screen siblings who may have received the same product.
- Reporting. If a defective commercial product is suspected, immediate reporting to the national regulator and to other clinicians is essential. The Remedia outbreak was halted by an alert clinician at Schneider Children's Medical Center who pattern-recognized a cluster within weeks.
11. Long-Term Sequelae in Survivors
The Remedia cohort, followed for over a decade by Fattal-Valevski and colleagues, demonstrated that even early-treated and clinically recovered infants can carry lifelong neurodevelopmental sequelae. The pattern of impairment reflects the brain regions most vulnerable to TPP-dependent enzyme failure.
- Language impairment. The most consistent finding in Remedia survivors: expressive language is more affected than receptive language, and the deficit can be present even in children with normal non-verbal IQ. The left hemisphere language network appears to be selectively vulnerable.
- Epilepsy. Roughly one-quarter of long-term survivors developed epilepsy, often with focal onset and frequently refractory to standard antiepileptics.
- Motor deficits. Spastic diplegia or quadriplegia in the most severely affected; subtler fine-motor and coordination deficits in milder cases.
- Visual deficits. Persistent strabismus, optic atrophy, and reduced visual acuity in a subset.
- Autistic-like features and behavioural problems. Reported in several Remedia survivors, plausibly related to early thalamic and basal ganglia injury.
- Cognitive variability. Some Remedia children have global cognitive impairment; others have normal overall IQ with isolated language or motor weakness. Outcome correlates strongly with how quickly thiamine was given after symptom onset.
12. Prevention
- Mandatory thiamine fortification of infant formula at a minimum of 60 μg per 100 kcal (Codex Alimentarius standard), with mandatory batch-level analytical testing of finished product, not just of the vitamin premix.
- Routine thiamine supplementation for pregnant and lactating women in populations with polished-rice or refined-flour staple diets. The WHO recommends 1.4 mg/day during pregnancy and lactation; in refugee settings, supplemental tablets to mothers reduce infant beriberi mortality dramatically.
- Universal thiamine before glucose in any unwell infant of uncertain feeding history — an inexpensive insurance against precipitating Wernicke encephalopathy in an unrecognised deficient state.
- Hyperemesis gravidarum management — parenteral thiamine for any pregnant woman with prolonged vomiting before IV dextrose is given.
- Maternal post-bariatric surveillance — structured vitamin supplementation and serum testing through pregnancy and lactation.
- Clinician education. Aphonia, cross-eyes in a previously normal infant, and unexplained lactic acidosis in an infant should all trigger empirical IV thiamine while diagnostics are arranged.
13. Research Papers and References
- Fattal-Valevski A, Kesler A, Sela BA, Nitzan-Kaluski D, Rotstein M, Mesterman R, Toledano-Alhadef H, Stolovitch C, Hoffmann C, Globus O, Eshel G. Outbreak of life-threatening thiamine deficiency in infants in Israel caused by a defective soy-based formula. Pediatrics. 2005;115(2):e233–e238. PMID: 15687431.
- Kornreich L, Bron-Harlev E, Hoffmann C, Schwarz M, Konen O, Schoenfeld T, Straussberg R, Nahum E, Ibrahim AK, Eshel G, Horev G. Thiamine deficiency in infants: MR findings in the brain. AJNR Am J Neuroradiol. 2005;26(7):1668–1674. PMID: 16091511.
- Fattal-Valevski A, Bloch-Mimouni A, Kivity S, Heyman E, Brezner A, Strausberg R, Inbar D, Kramer U, Goldberg-Stern H. Epilepsy in children with infantile thiamine deficiency. Neurology. 2009;73(11):828–833. PMID: 19571253.
- Fattal-Valevski A, Azouri-Fattal I, Greenstein YJ, Guindy M, Blau A, Zelnik N. Delayed language development due to infantile thiamine deficiency. Dev Med Child Neurol. 2009;51(8):629–634. PMID: 19416328.
- Mimouni-Bloch A, Goldberg-Stern H, Strausberg R, Brezner A, Heyman E, Inbar D, Kivity S, Zvulunov A, Sztarkier I, Fogelman R, Fattal-Valevski A. Thiamine deficiency in infancy: long-term follow-up. Pediatr Neurol. 2014;51(3):311–316. PMID: 25160535.
- Sechi G, Serra A. Wernicke's encephalopathy: new clinical settings and recent advances in diagnosis and management. Lancet Neurol. 2007;6(5):442–455. PMID: 17434099.
- Vasconcelos MM, Silva KP, Vidal G, Silva AF, Domingues RC, Berditchevsky CR. Early diagnosis of pediatric Wernicke's encephalopathy. Pediatr Neurol. 1999;20(4):289–294. PMID: 10328280.
- Luxemburger C, White NJ, ter Kuile F, Singh HM, Allier-Frachon I, Ohn M, Chongsuphajaisiddhi T, Nosten F. Beri-beri: the major cause of infant mortality in Karen refugees. Trans R Soc Trop Med Hyg. 2003;97(2):251–255. PMID: 14584384.
- McGready R, Simpson JA, Cho T, Dubowitz L, Changbumrung S, Bohm V, Munger RG, Sauberlich HE, White NJ, Nosten F. Postpartum thiamine deficiency in a Karen displaced population. Am J Clin Nutr. 2001;74(6):808–813. PMID: 11722963.
- Soukaloun D, Kounnavong S, Pengdy B, Boupha B, Durondej S, Olness K, Newton PN, White NJ. Dietary and socio-economic factors associated with beriberi in breastfed Lao infants. Ann Trop Paediatr. 2003;23(3):181–186. PMID: 14567832.
- Ortigoza-Escobar JD, Pérez-Dueñas B. Genetic defects of thiamine transport and metabolism. Pediatr Neurol. 2018;87:5–14. PMID: 30343745.
- Tabarki B, Al-Shafi S, Al-Shahwan S, Azmat Z, Al-Hashem A, Al-Adwani N, Biary N, Al-Zawahmah M, Khan S, Zuccoli G. Biotin-responsive basal ganglia disease revisited: clinical, radiologic, and genetic findings. Neurology. 2013;80(3):261–267. PMID: 23269594.
Live PubMed Searches
- Infantile thiamine deficiency
- Infantile beriberi
- Wernicke encephalopathy infant
- Shoshin beriberi
- Thiamine infant formula
- Biotin-thiamine-responsive basal ganglia disease
- Abducens palsy infant thiamine
- Mammillary body atrophy thiamine
Connections
- Remedia Soy Formula Outbreak (2003)
- Vitamin B1 (Thiamine) Main
- Thiamine and Beriberi (Adult)
- Thiamine and Brain Health
- Wernicke-Korsakoff Syndrome
- Cognitive Function and Alzheimer's
- Beriberi and Cardiac
- Magnesium
- Vitamin B12
- Vitamin B6
- Neurology
- Epilepsy
- Heart Failure
- Peripheral Neuropathy
- Lab Tests