Thiamine Deficiency (Beriberi): Wernicke-Korsakoff Syndrome
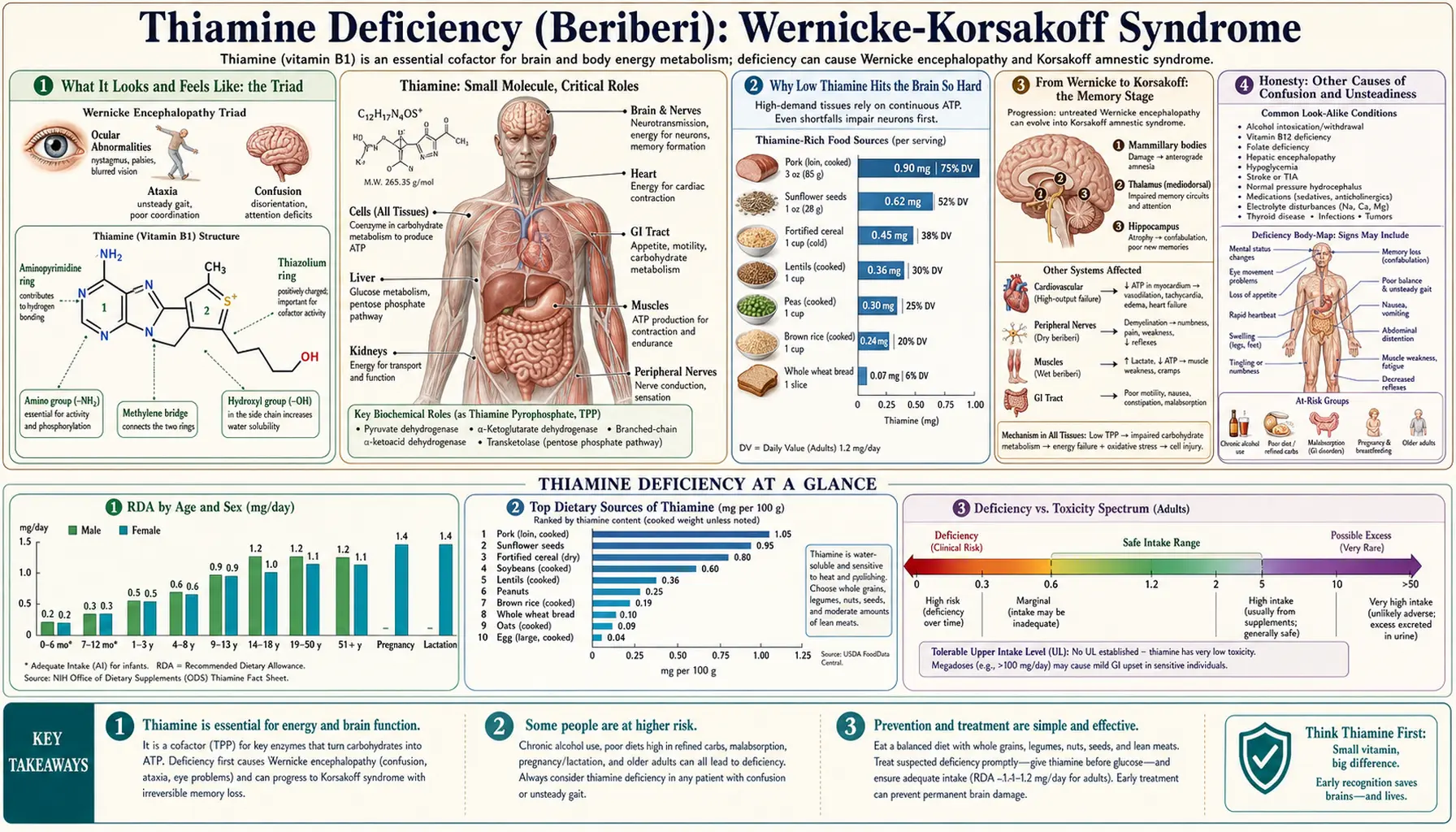
When the brain runs short of thiamine (vitamin B1), it can fail suddenly and dramatically. The acute crisis is called Wernicke encephalopathy — classically a triad of confusion, abnormal eye movements, and an unsteady, staggering walk — and it is a true medical emergency. Left untreated, it can slide into Korsakoff syndrome, a lasting, often permanent loss of the ability to form new memories. The two together are the Wernicke-Korsakoff syndrome. The single most important fact on this page is this: the treatment is intravenous thiamine, given urgently and given before any glucose, because sugar without thiamine can tip a vulnerable brain over the edge. This page explains what it feels like, why low B1 strikes the brain so hard, who is most at risk (heavy drinking and severe vomiting top the list), and why minutes matter.
Table of Contents
- What It Looks and Feels Like: the Triad
- Why Low Thiamine Hits the Brain So Hard
- From Wernicke to Korsakoff: the Memory Stage
- Honesty: Other Causes of Confusion and Unsteadiness
- Clues That Point to Thiamine
- Who Gets It: Causes and High-Risk Situations
- How It Is Diagnosed
- Treatment: IV Thiamine Before Glucose
- Red Flags: When to Act Immediately
- Key Research Papers
- Connections
- Featured Videos
What It Looks and Feels Like: the Triad
Wernicke encephalopathy was described as a triad of three signs that appear over hours to a few days. It helps to know them, because recognizing even one in a person at risk is enough to act:
- Confusion (altered mental state). This is the most common feature. People become disoriented, slow to respond, drowsy, inattentive, or unable to keep track of where they are and what is happening. It is not always dramatic raving — often it is a quiet, foggy, “not quite right” state that family members notice before anyone else. Untreated, it can deepen toward stupor and coma.
- Eye-movement problems (ophthalmoplegia / nystagmus). The muscles that aim the eyes are unusually vulnerable. The eyes may jerk rhythmically (nystagmus), fail to move outward (a sixth-nerve palsy), or fail to move together, producing double vision or a sense that the world won't hold still. A person may also notice drooping or that their gaze feels “stuck.”
- Unsteady walking (ataxia). A wide-based, staggering, drunk-looking gait — the person sways, can't walk heel-to-toe, and may be unable to stand without help. Because it looks like intoxication, it is tragically easy to dismiss in someone who has been drinking.
Here is the crucial, life-or-death caveat that decades of autopsy studies revealed: most people never show all three at once. In one landmark series of cases confirmed at autopsy, the full classic triad was documented in only about one in six patients, and a substantial fraction had shown no classic signs at all while alive. The lesson clinicians drew is blunt — do not wait for the triad. In an at-risk person, unexplained confusion alone, or new eye signs alone, or new unsteadiness alone, should trigger treatment.
Other features can accompany the triad: a low body temperature, a fast heart rate, low blood pressure on standing (because thiamine deficiency also stresses the heart and autonomic nerves — see wet beriberi), and profound apathy. Many patients also have the burning, numb feet of dry beriberi at the same time, because the same deficiency damages peripheral nerves.
Why Low Thiamine Hits the Brain So Hard
To understand why a vitamin shortage produces such sudden brain failure, it helps to know what thiamine actually does. Inside cells, thiamine is converted to its active form, thiamine pyrophosphate (TPP), which is an essential helper (a coenzyme) for a small set of enzymes that sit at the heart of energy production: pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase (both gateways into the cell's main energy cycle), and transketolase (which the brain also uses to make and repair the fatty insulation, myelin, around nerves).
The brain is the body's most energy-hungry organ. Although it is only about 2 percent of body weight, it burns roughly 20 percent of the body's resting energy, almost entirely by metabolizing glucose — and that metabolism runs straight through the thiamine-dependent enzymes above. The brain also holds very little thiamine in reserve. Whole-body thiamine stores are small and turn over fast; the body can be functionally depleted in as little as two to three weeks of poor intake. So when thiamine runs out, the brain's power plants stall first.
An analogy. Picture the brain as a busy city whose power plants can only burn one fuel — glucose — and that fuel only ignites with a specific spark plug, thiamine. The city keeps almost no spare spark plugs on hand. As long as new plugs arrive in the daily mail (your diet), the lights stay on. Cut off the supply and within a couple of weeks the plugs wear out one by one. The most power-hungry, hardest-working districts — the ones controlling eye movements, balance, and memory — brown out first. That is exactly the pattern of Wernicke encephalopathy.
This also explains the most dangerous detail in the whole subject. The cells that govern eye movement, balance, and short-term memory sit in deep, midline brain structures — the mammillary bodies, the tissue around the third and fourth ventricles, the thalamus, and the cerebellum — and these are precisely the regions with the highest thiamine-dependent metabolism. When the spark plugs fail there, those cells can't make enough energy to keep their internal balance of salts and water, they swell, lactic acid builds up, and if the shortage isn't fixed, they die. Early on, the injury is reversible. After a window of hours to days, it becomes permanent — which is why this is treated as an emergency rather than a clinic appointment.
From Wernicke to Korsakoff: the Memory Stage
Wernicke encephalopathy and Korsakoff syndrome are two stages of the same disease. Wernicke is the acute, potentially reversible emergency. Korsakoff is the chronic, often permanent aftermath that develops in a large share of people whose Wernicke episode was missed, treated too late, or treated with too little thiamine. The hallmark of Korsakoff is a striking, selective amnesia:
- Anterograde amnesia — the inability to lay down new memories. The person can hold a normal conversation, but minutes later has no recollection of it. They may read the same page repeatedly, or ask the same question again and again, with no memory of having asked.
- Retrograde amnesia — loss of memories from before the illness, often patchy, frequently worse for recent years than for the distant past.
- Confabulation — perhaps the most poignant feature. To fill the gaps, the person unconsciously and sincerely invents plausible accounts of events that never happened. This is not lying; they genuinely believe what they say. It tends to fade as the condition stabilizes.
What makes Korsakoff so distinctive is how preserved everything else can be. Attention, language, general intelligence, and old well-learned skills often remain largely intact, while the machinery for stamping in new experiences is gone. People can appear superficially normal in a brief chat, which is one reason the severity is underappreciated.
The reason the damage settles into memory specifically is anatomy: the memory circuit that runs from the mammillary bodies through the thalamus (part of what's called the Papez circuit) overlaps almost exactly with the regions that thiamine deficiency injures first. When those structures are scarred, the door to forming new long-term memories is essentially shut. Some recovery is possible with sustained thiamine, abstinence from alcohol, and good nutrition, but many people are left needing supervised or supported living. That bleak-to-permanent trajectory is precisely why catching the Wernicke stage and treating it hard is so important — it is the only reliable way to prevent Korsakoff.
Honesty: Other Causes of Confusion and Unsteadiness
It is important to be honest: the signs of Wernicke encephalopathy are not unique to thiamine deficiency. Confusion, abnormal eye movements, and an unsteady gait are among the most common and least specific findings in all of medicine, and most of the time the cause is something else entirely. The same picture — or pieces of it — can come from:
- Alcohol itself — intoxication and withdrawal both cause confusion, tremor, and an unsteady walk, which is exactly why Wernicke is so often missed in people who drink: everyone assumes it's “just the alcohol.”
- Infection — a urinary infection, pneumonia, or meningitis can cause acute confusion (delirium), especially in older adults.
- Other metabolic problems — low or high blood sugar, low sodium, high blood ammonia from liver disease, kidney failure, and thyroid disorders.
- Stroke or bleeding in the brain — particularly when eye signs or imbalance come on abruptly.
- Medications and other toxins — sedatives, opioids, lithium toxicity, and many others.
- Low vitamin B12 — longstanding B12 deficiency causes its own confusion, balance loss, and nerve damage, and can coexist with thiamine deficiency in the same malnourished person.
So the eye signs, the stagger, and the foggy mind do not by themselves prove thiamine deficiency. What they should do is put thiamine deficiency firmly on the list whenever the person has a risk factor — because of all these causes, this one is fixable in minutes with a cheap, safe vitamin, and devastating if missed. That asymmetry (low cost to treat, catastrophic cost to overlook) is the reason clinicians give thiamine empirically rather than waiting for certainty.
Clues That Point to Thiamine
While no single sign is proof, several features together raise the probability that confusion or unsteadiness is from thiamine deficiency rather than another cause:
- A high-risk background. Heavy or chronic alcohol use, weeks of vomiting (including gut conditions that limit eating and severe pregnancy sickness), recent bariatric (weight-loss) surgery, prolonged IV feeding without vitamins, or any state of severe malnutrition. The presence of one of these is the strongest clue of all.
- The combination, not the single sign. Confusion plus new eye-movement trouble, or confusion plus a staggering gait, is far more suggestive than any one alone. Modern criteria recommend treating when at least two of four features are present (dietary deficiency, eye signs, cerebellar/gait signs, or altered mental state/memory impairment) in someone at risk.
- It got worse after a sugary drink or IV fluids. A dramatic, classic clue: a malnourished person who becomes acutely confused after receiving glucose-containing IV fluids or a big carbohydrate load. Burning the sugar consumes the last of the brain's thiamine and can precipitate Wernicke — the single most important reason thiamine is always given first.
- It responds to thiamine. Eye signs in particular often begin to improve within hours of a thiamine dose. That rapid reversal is both treatment and confirmation.
- Company it keeps. Coexisting numb, burning feet (dry beriberi), breathlessness or leg swelling from a strained heart (wet beriberi), or the early fatigue and appetite loss of low B1 all point in the same direction.
For a fuller picture of what thiamine does for the brain and how depletion unfolds, see Thiamine and Brain Health and the deficiency hub at Thiamine Deficiency (Beriberi).
Who Gets It: Causes and High-Risk Situations
Because the body stores so little thiamine, any prolonged combination of poor intake, increased loss, or increased demand can empty the tank within weeks. The major settings are:
- Alcohol-use disorder — by far the most common cause in wealthy countries. Heavy drinking depletes thiamine through several routes at once: alcohol displaces food (poor intake), it directly impairs thiamine absorption in the gut, it reduces the liver's ability to store and activate it, and it increases its loss through the kidneys. The result is a chronically near-empty tank that a single carbohydrate load can push into crisis. This is why every person with alcohol-use disorder who presents confused, intoxicated, withdrawing, or malnourished is given thiamine.
- Persistent vomiting — including hyperemesis gravidarum. Severe pregnancy sickness that prevents eating for weeks is a classic and tragic cause of Wernicke encephalopathy in young, otherwise healthy women, and it can also harm the pregnancy. Any cause of prolonged vomiting — cancer chemotherapy, gut obstruction, an eating disorder — carries the same risk.
- Bariatric (weight-loss) surgery. After procedures that reduce stomach size or bypass part of the intestine, vomiting plus reduced absorption can produce thiamine deficiency, sometimes within weeks of surgery. Wernicke after bariatric surgery is well documented, which is why lifelong vitamin supplementation and prompt treatment of post-operative vomiting are essential.
- Severe malnutrition and starvation. Anorexia nervosa, advanced cancer, dialysis, AIDS, and famine all deplete thiamine. The refeeding period is especially dangerous: when a starved person is suddenly fed carbohydrate, the demand for thiamine to burn it spikes and can trigger acute Wernicke unless thiamine is given first.
- Prolonged IV feeding or IV dextrose without vitamins. Giving glucose calories to a depleted patient without adding thiamine is a recognized iatrogenic (treatment-caused) trigger.
- Other contributors. Magnesium deficiency (magnesium is needed to convert thiamine to its active form, so low magnesium can make thiamine treatment fail until corrected), some diuretics that increase thiamine loss, and chronic liver disease.
The common thread is that this is largely a preventable disease. In countries that add thiamine to flour and rice, and in hospitals that give thiamine routinely to at-risk patients, severe cases are far less common than they would otherwise be.
How It Is Diagnosed
The most important thing to understand about diagnosing Wernicke encephalopathy is that it is, first and foremost, a clinical diagnosis made on suspicion — and that treatment must never wait for a test. There is no quick bedside blood test that confirms it in time to matter. The diagnostic steps support and refine the picture, but the decision to treat is made the moment the suspicion arises:
- Clinical criteria. Widely used operational criteria recommend a presumptive diagnosis in an at-risk person who has any two of four: a dietary deficiency, eye-movement signs, cerebellar/gait dysfunction, and altered mental state or memory impairment. Meeting just one in a high-risk person is still enough to treat empirically.
- Blood thiamine status. Thiamine can be measured — usually as whole-blood thiamine or by an older red-cell “transketolase activation” assay — but the results take time, are not available everywhere, and must be drawn before giving thiamine. They are used to confirm the diagnosis after the fact, never to decide whether to treat.
- Magnesium and a metabolic panel. A comprehensive metabolic panel checks blood sugar, sodium, kidney and liver function (to find or exclude other causes of confusion), and a magnesium level matters because low magnesium blunts the response to thiamine.
- Other bloods. A complete blood count and liver function tests help characterize a malnourished or heavy-drinking patient, and a vitamin B12 level is reasonable because B12 deficiency can mimic or accompany the picture.
- Brain MRI. Magnetic resonance imaging can show the characteristic swelling in the deep midline structures (around the third ventricle, the mammillary bodies, and the thalamus). When positive it is highly suggestive, but a normal MRI does not rule Wernicke out — many patients with the disease have a normal scan. Imaging confirms; it never excludes.
The take-home is that diagnosis here is a clinical judgment backed by tests that arrive too slowly to gate treatment. The safe, evidence-based default is: suspect it, treat it, then confirm.
Treatment: IV Thiamine Before Glucose
Two principles define the treatment of Wernicke encephalopathy, and both are matters of urgency:
1. Give thiamine before any glucose. This is the most important rule in the entire subject. In a thiamine-depleted person, supplying glucose — whether a sugary drink, a meal, or (most dangerously) an IV bag of dextrose — forces the brain to burn fuel through enzymes that need thiamine it doesn't have. That can consume the last traces of thiamine and precipitate or worsen Wernicke encephalopathy within hours. So in any at-risk, confused, or collapsed patient, thiamine is given first, or at the same time, never after glucose alone.
2. Treat early, treat parenterally, and treat with enough. Oral thiamine is poorly absorbed and is not adequate for an acute Wernicke crisis. The standard of care is intravenous (or intramuscular) thiamine in high doses — guidelines commonly recommend on the order of 500 mg IV three times daily for the first two to three days in established Wernicke encephalopathy, followed by lower daily doses for several more days, then a maintenance oral dose. (Exact regimens vary; this is given by clinicians, not self-administered.) Parenteral thiamine is remarkably safe; serious reactions are very rare, and the risk of giving it when it turns out not to be needed is negligible compared with the risk of withholding it.
Alongside thiamine, treatment includes:
- Correcting magnesium — because magnesium is a required cofactor for activating thiamine, replacing low magnesium is part of making the thiamine work.
- Replacing other B vitamins and nutrients — deficiencies rarely travel alone in a malnourished or heavy-drinking person.
- Treating the underlying cause — managing alcohol withdrawal safely, controlling vomiting, supporting nutrition, and following up after bariatric surgery.
- Rehabilitation — if Korsakoff memory impairment has set in, supportive care, structured environments, and sustained abstinence give the best chance of partial recovery.
The reward for speed is large. Eye signs often improve within hours of IV thiamine, and the staggering gait and confusion can resolve over days. The tragedy of delay is equally large: once the deep brain structures are scarred, the resulting Korsakoff amnesia is frequently permanent. Prevention is better still — giving thiamine routinely to at-risk patients, and never giving glucose to a depleted person without it, prevents most cases entirely.
Red Flags: When to Act Immediately
Wernicke-Korsakoff syndrome is one of the situations where minutes and hours genuinely change the outcome. Call emergency services or get to an emergency department immediately — and say the words “could this be thiamine deficiency / Wernicke encephalopathy?” — if a person who drinks heavily, has been vomiting for days, has had weight-loss surgery, or is severely malnourished develops any of the following:
- New confusion, drowsiness, or disorientation — especially if it is worsening, and most urgently if it came on or worsened after a sugary drink, a big meal, or IV fluids.
- New eye problems — double vision, eyes that jerk or won't move together, or a sense that vision won't hold still.
- A new staggering, unsteady, or drunk-looking walk in someone who has not just been drinking enough to explain it — or who has, since intoxication is precisely what hides this diagnosis.
- Profound apathy, stupor, or unresponsiveness.
- Inability to form new memories, or repeating the same questions — a sign the condition may already be progressing toward Korsakoff and still needs urgent thiamine.
One practical, potentially life-saving point for families and caregivers: if someone at risk is acutely unwell, do not push them to eat or drink large amounts of sugar, and tell paramedics and hospital staff about the risk so they give thiamine first. In any genuine emergency, of course, call for professional help rather than attempting to manage it at home — high-dose IV thiamine and monitoring are hospital treatments. But naming the risk out loud can prompt the one cheap, safe intervention that prevents lifelong amnesia.
Key Research Papers
- Sechi G, Serra A (2007). Wernicke's encephalopathy: new clinical settings and recent advances in diagnosis and management. The Lancet Neurology;6(5):442-455. — DOI: 10.1016/S1474-4422(07)70104-7
- Galvin R, Brathen G, Ivashynka A, et al. (2010). EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. European Journal of Neurology;17(12):1408-1418. — DOI: 10.1111/j.1468-1331.2010.03153.x
- Caine D, Halliday GM, Kril JJ, Harper CG (1997). Operational criteria for the classification of chronic alcoholics: identification of Wernicke's encephalopathy. Journal of Neurology, Neurosurgery & Psychiatry;62(1):51-60. — DOI: 10.1136/jnnp.62.1.51
- Harper CG, Giles M, Finlay-Jones R (1986). Clinical signs in the Wernicke-Korsakoff complex: a retrospective analysis of 131 cases diagnosed at necropsy. Journal of Neurology, Neurosurgery & Psychiatry;49(4):341-345. — DOI: 10.1136/jnnp.49.4.341
- Donnino MW, Vega J, Miller J, Walsh M (2007). Myths and misconceptions of Wernicke's encephalopathy: what every emergency physician should know. Annals of Emergency Medicine;50(6):715-721. — DOI: 10.1016/j.annemergmed.2007.02.007
- Thomson AD, Marshall EJ (2006). The natural history and pathophysiology of Wernicke's encephalopathy and Korsakoff's psychosis. Alcohol and Alcoholism;41(2):151-158. — PubMed
- Cook CC, Hallwood PM, Thomson AD (2000). Mechanisms of vitamin deficiency in chronic alcohol misusers and the development of the Wernicke-Korsakoff syndrome. Alcohol and Alcoholism;35(Suppl 1):2-7. — DOI: 10.1093/alcalc/35.supplement_1.2
- Latt N, Dore G (2014). Thiamine in the treatment of Wernicke encephalopathy in patients with alcohol use disorders. Internal Medicine Journal;44(9):911-915. — DOI: 10.1111/imj.12522
- Aasheim ET (2008). Wernicke encephalopathy after bariatric surgery: a systematic review. Annals of Surgery / Neurology;249(5):714-720. — DOI: 10.1212/01.wnl.0000278895.59835.68
- Kopelman MD, Thomson AD, Guerrini I, Marshall EJ (2009). The Korsakoff syndrome: clinical aspects, psychology and treatment. Alcohol and Alcoholism;44(2):148-154. — DOI: 10.1093/alcalc/agn118
- Arts NJM, Walvoort SJW, Kessels RPC (2017). Korsakoff's syndrome: a critical review. Neuropsychiatric Disease and Treatment;13:2875-2890. — DOI: 10.2147/NDT.S130078
- Whitfield KC, Bourassa MW, Adamolekun B, et al. (2018). Thiamine deficiency disorders: diagnosis, prevalence, and a roadmap for global control programs. Annals of the New York Academy of Sciences;1430(1):3-43. — DOI: 10.1111/nyas.13919
- Sechi G, Sechi E, Fois C, Kumar N (2023). Observations on the clinical features of the Wernicke-Korsakoff syndrome. Journal of Clinical Medicine;12(19):6310. — DOI: 10.3390/jcm12196310
PubMed Topic Searches
- PubMed — Wernicke encephalopathy triad and diagnosis
- PubMed — Korsakoff syndrome, amnesia, and confabulation
- PubMed — Thiamine before glucose in Wernicke encephalopathy
- PubMed — Hyperemesis gravidarum and Wernicke encephalopathy
- PubMed — Bariatric surgery, thiamine deficiency, and Wernicke
Connections
- Thiamine Deficiency Hub
- Wet Beriberi (Heart)
- Dry Beriberi (Nerves)
- Fatigue & Appetite Loss
- Vitamin B1 (Thiamine) Overview
- Thiamine and Brain Health
- Thiamine and Beriberi
- Vitamin B12
- Liver Disease
- SIBO & Malabsorption
- Comprehensive Metabolic Panel
- Magnesium Test
- Complete Blood Count
- Liver Function Tests
- Vitamin B12 Test