Thiamine Deficiency: Beriberi and Wernicke-Korsakoff Syndrome
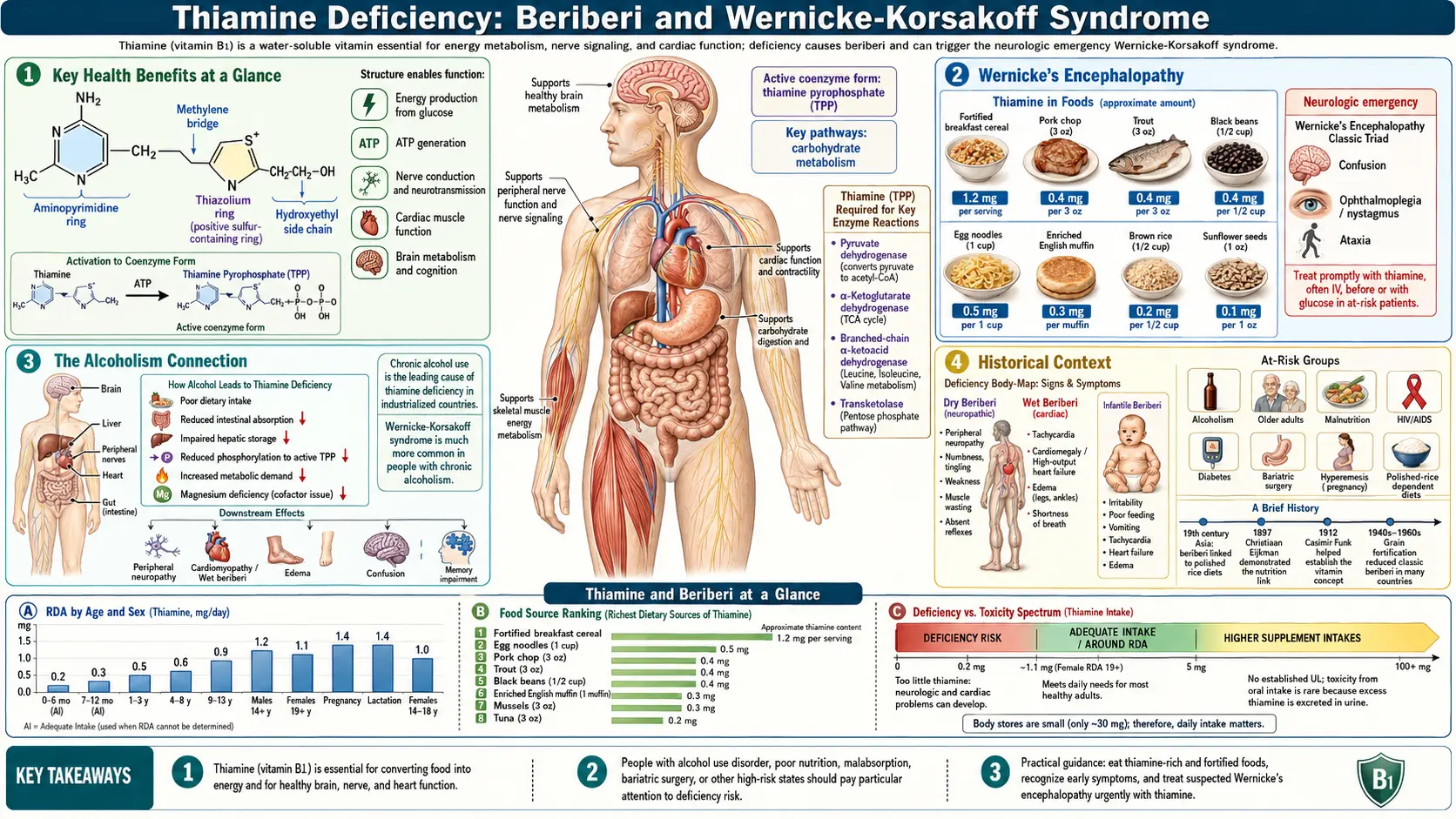
Thiamine (vitamin B1) is an essential water-soluble vitamin that serves as a cofactor for critical enzymes in carbohydrate metabolism and energy production. When thiamine intake is insufficient, the consequences can be severe and even fatal. The clinical syndromes of beriberi and Wernicke-Korsakoff syndrome represent the most dramatic manifestations of thiamine deficiency, affecting the cardiovascular and nervous systems with devastating efficiency. Beriberi ravaged 19th- and 20th-century Asia — driven by refined white rice — and its solution helped launch the modern science of vitamins. Today, Wernicke-Korsakoff remains a neuropsychiatric emergency in alcoholic and post-bariatric populations. Despite being well understood and entirely preventable, these conditions continue to affect populations worldwide.
Table of Contents
- Key Health Benefits at a Glance
- Wet Beriberi: Cardiovascular Manifestations
- Dry Beriberi: Neurological Manifestations
- Wernicke’s Encephalopathy
- Korsakoff’s Psychosis
- The Alcoholism Connection
- Thiamine-Responsive Conditions
- Emergency Treatment
- Historical Context
- Research Papers and References
- Connections
- Featured Videos
Key Health Benefits at a Glance
The following is a high-level summary of why recognizing and preventing thiamine deficiency matters clinically. Each point ties back to a specific deficiency syndrome explored below, and the supporting papers are listed in the Research Papers section.
- Reverses wet beriberi heart failure – IV thiamine rapidly reverses the high-output cardiac failure of wet beriberi, often within 24–48 hours, a therapeutic response so dramatic it is practically diagnostic.
- Prevents Wernicke’s encephalopathy in at-risk patients – Prophylactic parenteral thiamine in alcohol-dependent or malnourished patients prevents the classic ocular/ataxia/confusion triad and the dreaded progression to Korsakoff amnesia.
- Averts the "glucose-before-thiamine" catastrophe – Administering IV dextrose to a thiamine-depleted patient without thiamine can precipitate acute Wernicke’s — a critical emergency-department lesson.
- Halts dry beriberi polyneuropathy – Early thiamine repletion can reverse the ascending sensorimotor neuropathy before it becomes permanent.
- Saves infant lives – Infantile beriberi in breastfed infants of deficient mothers responds dramatically to parenteral thiamine; without it, mortality is high.
- Treats Shoshin beriberi – The fulminant cardiac variant responds to immediate IV thiamine plus hemodynamic support; delay is usually fatal.
- Reduces risk in bariatric surgery patients – Thiamine supplementation mitigates the risk of post-operative Wernicke’s encephalopathy, especially in patients with persistent vomiting.
- Corrects TRMA – High-dose thiamine corrects megaloblastic anemia and diabetes in thiamine-responsive megaloblastic anemia (SLC19A2 mutation) — one of the few genetic diseases with a simple vitamin cure.
- Prevents Casimir Funk’s "vital amine" deficiency at scale – National grain-fortification programs for thiamine essentially eliminated endemic beriberi in the U.S. and Europe within a generation.
Wet Beriberi: Cardiovascular Manifestations
Wet beriberi is the cardiovascular form of thiamine deficiency, characterized by high-output cardiac failure with peripheral vasodilation and fluid retention. The pathophysiology centers on impaired myocardial energy metabolism and loss of vascular smooth muscle tone:
- High-output heart failure – Without adequate thiamine, the heart cannot efficiently generate ATP through oxidative phosphorylation. The myocardium attempts to compensate by increasing heart rate and stroke volume, leading to a hyperdynamic circulatory state. Cardiac output may be elevated to two or three times normal, but the heart eventually fails under the sustained workload.
- Peripheral vasodilation – Thiamine deficiency causes accumulation of pyruvate, lactate, and other metabolic intermediates that promote vasodilation. The resulting decrease in systemic vascular resistance compounds the cardiac burden and contributes to hypotension in advanced cases.
- Peripheral edema – Sodium and water retention, driven by activation of the renin-angiotensin-aldosterone system in response to reduced effective circulating volume, produces bilateral lower extremity edema. In severe cases, ascites and pleural effusions develop.
- Pulmonary congestion – As the left ventricle fails, pulmonary venous pressure rises, leading to dyspnea, orthopnea, and paroxysmal nocturnal dyspnea. Pulmonary edema can develop rapidly and is a leading cause of death in untreated wet beriberi.
- Shoshin beriberi – This fulminant variant presents as acute cardiovascular collapse with severe lactic acidosis, tachycardia, and cardiogenic shock. Shoshin beriberi carries an extremely high mortality rate without immediate intravenous thiamine administration and hemodynamic support.
Dry Beriberi: Neurological Manifestations
Dry beriberi is the peripheral neurological form of thiamine deficiency, affecting the peripheral nerves with a characteristic pattern of ascending, symmetric polyneuropathy:
- Peripheral neuropathy – The earliest symptoms are typically paresthesias (tingling, burning, or numbness) in the feet and lower legs, progressing proximally in a stocking-glove distribution. Nerve conduction studies reveal axonal degeneration with reduced amplitudes and mildly decreased conduction velocities.
- Muscle weakness – Progressive weakness begins in the distal lower extremities, particularly the toe extensors and ankle dorsiflexors, leading to foot drop and a characteristic high-stepping gait. Without treatment, weakness ascends to involve the thighs, hands, and forearms.
- Muscle wasting – Denervation of skeletal muscle leads to neurogenic atrophy, with visible loss of muscle bulk in the calves and intrinsic muscles of the feet. Deep tendon reflexes, initially hyperactive, become diminished and eventually absent as the neuropathy progresses.
- Pain and tenderness – Calf tenderness on palpation (calf squeeze test) is a classic finding in dry beriberi. Patients may experience severe neuropathic pain, burning sensations, and hyperesthesia (painful sensitivity to light touch).
- Autonomic dysfunction – Involvement of autonomic nerve fibers can cause tachycardia, postural hypotension, gastrointestinal dysmotility, and anhidrosis (absence of sweating) in affected dermatomes.
Wernicke’s Encephalopathy
Wernicke’s encephalopathy (WE) is an acute neuropsychiatric emergency caused by thiamine deficiency affecting the central nervous system. The classic clinical triad consists of:
- Confusion and altered mental status – Patients present with global confusional state, disorientation, inattentiveness, and apathy. The degree of impairment ranges from mild lethargy to deep stupor or coma. The confusional state reflects metabolic dysfunction in the thalamus and mammillary bodies, which are exquisitely sensitive to thiamine depletion.
- Ataxia – Cerebellar dysfunction produces a wide-based, unsteady gait. Patients may be unable to stand or walk without assistance. Truncal ataxia (difficulty maintaining upright posture while seated) is common. The cerebellar vermis, particularly the anterior superior vermis, shows selective vulnerability to thiamine deficiency.
- Ophthalmoplegia – Ocular findings include nystagmus (horizontal more commonly than vertical), lateral rectus palsy (abducens nerve palsy) causing inability to abduct the eyes, and conjugate gaze palsies. Complete external ophthalmoplegia can develop in severe cases. These findings reflect involvement of the oculomotor, abducens, and vestibular nuclei in the brainstem.
Importantly, the complete classic triad is present in only approximately 16–33% of cases. Clinicians must maintain a high index of suspicion and initiate treatment empirically when any component of the triad is present in an at-risk patient. MRI findings characteristically show symmetric signal abnormalities in the medial thalami, mammillary bodies, periaqueductal gray matter, and tectal plate on T2-weighted and FLAIR sequences.
Korsakoff’s Psychosis
Korsakoff’s psychosis (Korsakoff’s syndrome) typically develops as Wernicke’s encephalopathy resolves, either spontaneously or with treatment. It represents the chronic, irreversible neuropsychiatric sequel of thiamine deficiency-induced brain damage:
- Anterograde amnesia – The hallmark feature is a profound inability to form new memories. Patients cannot learn new information or recall events that occurred after the onset of the syndrome. This results from destruction of the mammillary bodies and their projections via the mammillothalamic tract to the anterior thalamic nuclei, structures critical for memory consolidation.
- Retrograde amnesia – Variable loss of memories formed before the onset of illness, typically following a temporal gradient where recent memories are more severely affected than remote ones.
- Confabulation – Patients spontaneously generate false memories to fill gaps in their recall, often with remarkable confidence and detail. Confabulation is not deliberate lying; patients genuinely believe their fabricated accounts. This feature is most prominent in the early stages and tends to diminish over time.
- Lack of insight – Patients are typically unaware of or unconcerned about their memory deficits (anosognosia). They may appear superficially pleasant and conversational, masking the severity of their cognitive impairment.
- Preserved other cognition – Unlike dementia, general intelligence, attention, language, and procedural memory are relatively preserved. Patients can carry on conversations, perform routine tasks, and recall well-established remote memories.
The Alcoholism Connection
Chronic alcohol use disorder is the most common cause of Wernicke-Korsakoff syndrome in developed countries. The relationship between alcoholism and thiamine deficiency is multifactorial:
- Inadequate dietary intake – Individuals with severe alcohol use disorder frequently derive the majority of their caloric intake from alcohol, which provides energy but no thiamine. Dietary neglect and poverty further limit access to thiamine-rich foods.
- Impaired intestinal absorption – Chronic alcohol exposure directly damages the intestinal mucosa and inhibits the active transport system for thiamine absorption in the jejunum. Absorption can be reduced by as much as 70% in chronic alcoholics.
- Reduced hepatic storage and phosphorylation – Alcohol-related liver disease impairs the liver’s ability to store thiamine and convert it to its active form, thiamine pyrophosphate (TPP). Hepatic thiamine stores in alcoholic patients may be reduced to less than half of normal levels.
- Increased metabolic demand – Ethanol metabolism generates acetaldehyde, which increases oxidative stress and thiamine utilization. Additionally, alcohol-induced magnesium depletion impairs thiamine-dependent enzyme function, since magnesium is a required cofactor for TPP-dependent reactions.
- Glucose loading risk – Administration of intravenous dextrose to malnourished patients without concurrent thiamine supplementation can precipitate acute Wernicke’s encephalopathy by exhausting remaining thiamine reserves in the processing of the glucose load. This is a critical consideration in emergency departments.
Thiamine-Responsive Conditions
Beyond classic beriberi and Wernicke-Korsakoff syndrome, several other conditions are associated with thiamine deficiency or respond to thiamine supplementation:
- Infantile beriberi – Breastfed infants of thiamine-deficient mothers can develop acute cardiac beriberi, presenting with rapid-onset heart failure, aphonia (inability to cry), and cyanosis. This remains a significant cause of infant mortality in parts of Southeast Asia.
- Gastrointestinal beriberi – Nausea, vomiting, abdominal pain, and lactic acidosis can occur as thiamine-deficient forms of beriberi affecting the gastrointestinal tract. These symptoms often precede cardiac or neurological manifestations.
- Thiamine-responsive megaloblastic anemia (TRMA) – A rare autosomal recessive disorder caused by mutations in the SLC19A2 gene encoding a high-affinity thiamine transporter, presenting with megaloblastic anemia, diabetes mellitus, and sensorineural hearing loss.
- Post-bariatric surgery deficiency – Patients who have undergone gastric bypass or sleeve gastrectomy are at increased risk due to reduced gastric acid production, bypassed absorption sites, and persistent vomiting in the postoperative period.
Emergency Treatment
Suspected Wernicke’s encephalopathy is a medical emergency requiring immediate intervention:
- Intravenous thiamine – The standard emergency treatment is intravenous thiamine hydrochloride, typically 500 mg administered three times daily for 2–3 days, followed by 250 mg daily for an additional 3–5 days. Intramuscular administration is an acceptable alternative if IV access is unavailable.
- Before glucose – Thiamine must always be administered before or simultaneously with any glucose-containing intravenous fluids. Glucose administration without thiamine can precipitate or worsen Wernicke’s encephalopathy by consuming the last remaining thiamine stores.
- Magnesium repletion – Concurrent magnesium supplementation is essential, as hypomagnesemia (common in alcoholic patients) renders thiamine-dependent enzymes non-functional even when thiamine is repleted. Magnesium sulfate 2 grams IV is typically administered.
- Response monitoring – Ocular signs typically improve within hours to days of thiamine administration. Ataxia resolves more slowly over days to weeks. Confusional state may take weeks to clear. Korsakoff’s amnesia, once established, recovers only partially in approximately 20% of patients.
- Oral maintenance – Following acute treatment, long-term oral thiamine supplementation (100–300 mg daily) is recommended, along with a balanced diet and alcohol abstinence support.
Historical Context
The history of beriberi and its connection to thiamine is a landmark chapter in the history of nutritional science:
- Asian rice epidemics – Beriberi was endemic in Asian populations subsisting primarily on polished (white) rice, which has the thiamine-rich bran and germ removed during milling. The disease caused devastating epidemics in the 19th and early 20th centuries, killing hundreds of thousands in Japan, the Philippines, and Indonesia.
- Christiaan Eijkman – In the 1890s, Dutch physician Christiaan Eijkman observed that chickens fed polished rice developed polyneuritis resembling beriberi, while those fed unpolished rice remained healthy. This groundbreaking observation, which earned him the Nobel Prize in 1929, established the concept that disease could result from the absence of an essential dietary factor.
- Casimir Funk – In 1912, Polish biochemist Casimir Funk isolated an anti-beriberi factor from rice bran and coined the term “vitamine” (vital amine) to describe it. Although the compound he isolated was actually nicotinic acid rather than thiamine, his concept of essential dietary amines launched the era of vitamin discovery.
- Robert R. Williams – The chemical structure of thiamine was determined by Robert R. Williams in 1936, enabling its synthesis and widespread use in food fortification programs that have largely eradicated beriberi in developed nations.
- Modern persistence – Despite fortification, beriberi and Wernicke-Korsakoff syndrome persist in vulnerable populations including chronic alcoholics, refugees and displaced persons, prisoners, and patients receiving prolonged parenteral nutrition without adequate supplementation.
Thiamine deficiency syndromes remain an important consideration in clinical practice. Maintaining awareness of the risk factors, recognizing the early clinical signs, and initiating prompt treatment with parenteral thiamine can prevent irreversible neurological damage and save lives. The historical lesson of beriberi reminds us that even in an era of nutritional abundance, deficiency diseases continue to affect those most marginalized by poverty, addiction, and inadequate healthcare access.
Research Papers and References
The following are landmark and frequently cited research papers underpinning the claims on this page. Links resolve to the publisher DOI or PubMed record.
Foundational Reviews
- Lonsdale D. A review of the biochemistry, metabolism and clinical benefits of thiamin(e) and its derivatives. Evid Based Complement Alternat Med. 2006;3(1):49-59.
- PubMed — Thiamine deficiency: clinical and biochemical review
Wernicke-Korsakoff Syndrome and Alcoholism
- PubMed — Wernicke encephalopathy: diagnostic criteria and alcoholic populations
- PubMed — Korsakoff syndrome, mammillary body pathology and amnesia
- PubMed — Parenteral thiamine dosing in suspected Wernicke encephalopathy
Beriberi (Wet, Dry, Shoshin, Infantile)
- PubMed — Wet beriberi, high-output heart failure and thiamine response
- PubMed — Shoshin (fulminant) beriberi case series
- PubMed — Infantile beriberi in breastfed infants of deficient mothers
Post-Bariatric, TRMA, and Other At-Risk Populations
- PubMed — Thiamine deficiency and Wernicke after bariatric surgery
- PubMed — SLC19A2 mutations and thiamine-responsive megaloblastic anemia (TRMA)
Historical and Public-Health Milestones
- PubMed — Eijkman’s polyneuritis-rice experiments: historical reviews
- PubMed — Casimir Funk and the “vitamine” concept
External Authoritative Resources
- NIH Office of Dietary Supplements — Thiamin Fact Sheet for Health Professionals
- Linus Pauling Institute Micronutrient Information Center — Thiamin
- Harvard T.H. Chan School — Nutrition Source: B Vitamins
- PubMed — Thiamine deficiency research
Connections
- All Vitamins
- Vitamin B1
- Thiamine and Brain Health
- Magnesium
- Heart Failure
- Vitamin B3
- Vitamin B6
- Vitamin B12
- Vitamin B2
- Depression
- Alzheimer's Disease
- Anemia
- Edema
- Peripheral Neuropathy
- Stroke
- Diabetes
- Pellagra and Niacin Deficiency