Calcium — Benefits Deep Dive
Calcium is the most abundant mineral in the human body and the only mineral that simultaneously functions as the principal structural material of the skeleton, the universal trigger of muscle contraction, the master molecule of synaptic transmission, and the second messenger that translates extracellular signals into intracellular responses across virtually every cell type. Four benefit pages below explore the conditions where calcium produces the largest clinical effect — the bone health and osteoporosis story complete with the modern caveats from the Bolland calcium-supplement-cardiovascular-event meta-analyses, the cardiovascular dual role of calcium as both heartbeat trigger and atherosclerosis marker, the cellular machinery of muscle contraction across skeletal / cardiac / smooth tissues, and the synaptic and neuromuscular biology of calcium-triggered neurotransmitter release together with the seizure-threshold and channelopathy consequences when neuronal calcium signaling fails.
Deep-Dive Articles
Bone Health
The bone remodeling cycle (activation, resorption, reversal, formation, quiescence), osteoblast vs osteoclast cell biology, RANKL/OPG regulation, peak bone mass accrual through adolescence, osteoporosis prevention, vitamin D synergy for intestinal absorption, weight-bearing-exercise mechanotransduction via osteocytes and the Wnt/sclerostin axis, calcium absorption factors (oxalates, phytates, gastric acid, age), and age-related involutional plus menopausal bone loss. Modern Tai 2015 BMJ caveat: diminishing returns above ~800 mg/day.
Cardiovascular Health
Calcium's uncomfortable dual role: indispensable trigger of every heartbeat via calcium-induced calcium release (CICR) and L-type channels, AND structural marker of advanced atherosclerosis quantified by the coronary artery calcium (CAC) score. The vitamin K2 / Matrix Gla Protein axis that decides whether dietary calcium ends up in bone or in arteries, the Bolland 2010-2011 calcium supplement cardiovascular controversy in detail, and calcium channel blockers (amlodipine, verapamil) as pharmacological counterpoint.
Muscle Function
Excitation-contraction coupling in skeletal muscle (DHPR-RyR1 mechanical coupling), the troponin-tropomyosin regulatory system, sarcoplasmic reticulum release and SERCA reuptake, smooth muscle calmodulin-MLCK signaling and the RhoA/Rho-kinase calcium sensitization pathway, cardiac CICR and beta-adrenergic phosphorylation of phospholamban, voltage-gated calcium channel subtypes (L, T, N, P/Q, R), and the hypocalcemic tetany signs (Trousseau, Chvostek).
Nerve Transmission
The presynaptic calcium nanodomain, synaptotagmin C2 domains as the fast calcium sensor, SNARE-mediated vesicle fusion, P/Q-type and N-type calcium channels at active zones, the neuromuscular junction's safety factor, Lambert-Eaton myasthenic syndrome (anti-CaV2.1 antibodies), familial hemiplegic migraine (CACNA1A mutations), hypocalcemic seizure threshold, and the calcium hypothesis of neurodegeneration in Parkinson's and Alzheimer's.
Table of Contents
- Deep-Dive Articles
- Why Calcium Produces Effects Across So Many Systems
- Research Papers: Bone Health
- Research Papers: Cardiovascular
- Research Papers: Muscle Function
- Research Papers: Nerve Transmission
- Research Papers: Cross-Cutting (Mechanism, Status, Safety)
- External Authoritative Resources
- Connections
- Featured Videos
Why Calcium Produces Effects Across So Many Systems
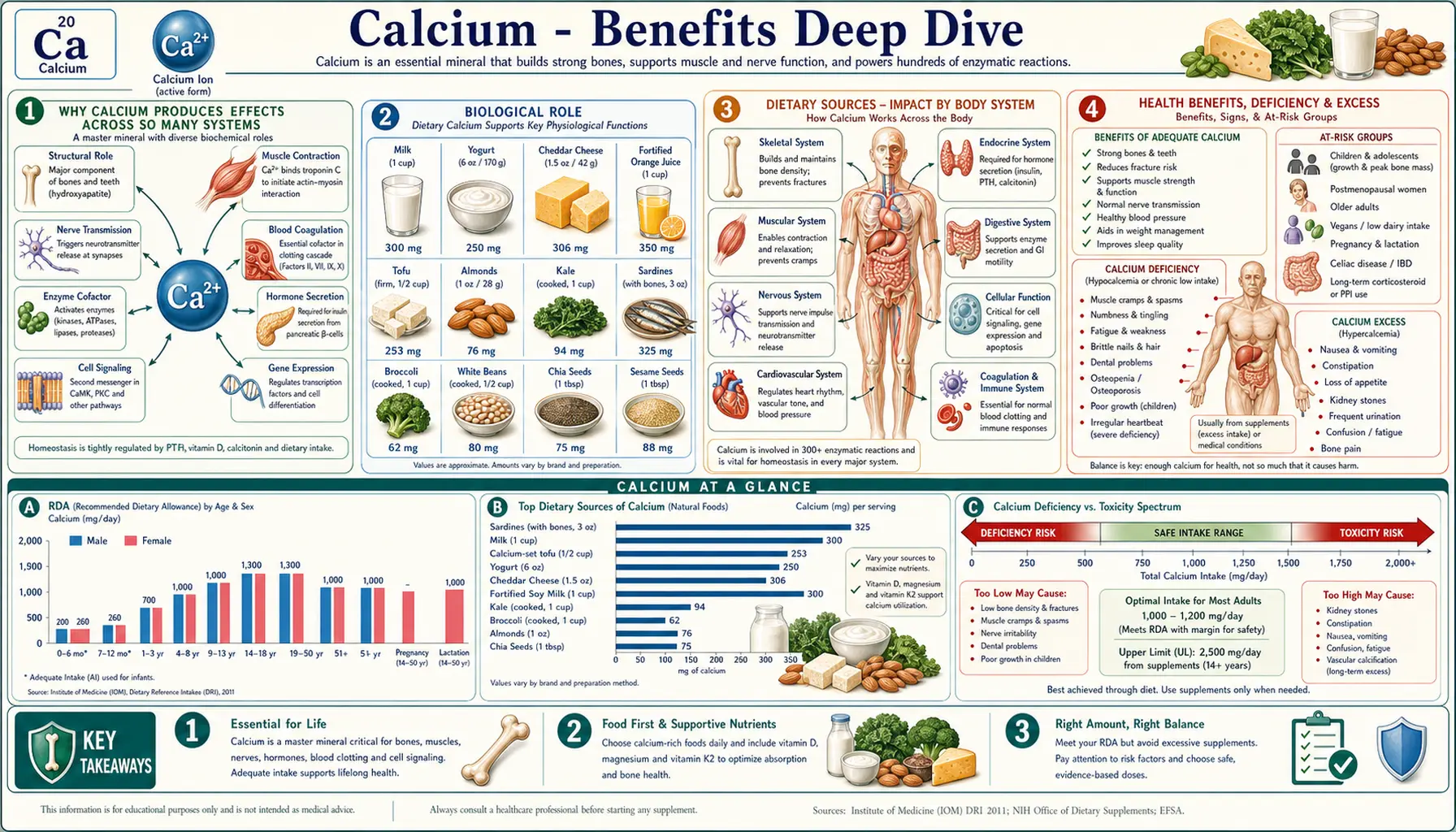
Most nutrients act through one principal mechanism (water-soluble cofactors typically donate a chemical group to a specific enzyme reaction; fat-soluble vitamins signal through one or two nuclear receptors). Calcium is unusual because it operates simultaneously in four fundamentally distinct roles, and each of those roles maps to a distinct category of clinical effect:
- Structural mineral – 99% of body calcium is locked into hydroxyapatite crystals (Ca10(PO4)6(OH)2) within the collagen matrix of bone and tooth enamel. This is the bulk structural role that supports the entire mechanical edifice of the human skeleton. The clinical consequences of inadequate structural calcium are osteoporosis, fragility fractures, rickets, and osteomalacia.
- Universal contraction trigger – Cytoplasmic Ca2+ is the final common signal for skeletal, cardiac, and smooth muscle activation through troponin-C, calmodulin-MLCK, and SR-RyR pathways. This mechanism drives the muscle-contraction effects and the cardiac CICR / heartbeat mechanism.
- Synaptic vesicle-fusion trigger – Presynaptic Ca2+ influx through P/Q-type and N-type voltage-gated channels binds synaptotagmin and catalyzes SNARE-mediated vesicle fusion, releasing neurotransmitter into the synaptic cleft. This is the molecular basis of all chemical synaptic transmission, every motor neuron action, every memory formation event, and every neuroendocrine secretion.
- Universal second messenger – Cytoplasmic Ca2+ activates calmodulin, CaMKII, calcineurin, calpains, PKC, phospholipase A2, and dozens of other downstream signaling proteins that regulate gene expression, hormone secretion (insulin, PTH, catecholamines), immune cell activation (T-cell receptor signaling through NFAT), and apoptosis. This is the unifying role that links calcium signaling to virtually every cellular process not covered by the first three roles.
The therapeutic complication is that these four roles overlap and pull in different directions when supplementation is considered. The same calcium supplement intended to support bone (role 1) raises serum ionized calcium acutely (potentially destabilizing role 2 cardiac rhythm in vulnerable patients), affects vascular smooth muscle tone (role 2), and may deposit ectopically in arterial walls if the vitamin K2 / Matrix Gla Protein axis is suboptimal. The Bolland 2010-2011 supplement-cardiovascular meta-analyses are the empirical signal that this trade-off is real, not theoretical. Modern best practice prioritizes dietary calcium from food matrices (which deliver the calcium more slowly and with co-nutrients magnesium and K2), uses supplements only to bridge documented dietary insufficiency, splits doses to no more than 500 mg per administration, and pairs supplementation with adequate vitamin D3 and vitamin K2 (MK-7).
Research Papers: Bone Health
- Tai V, Leung W, Grey A, Reid IR, Bolland MJ (2015). Calcium intake and bone mineral density: systematic review and meta-analysis. BMJ. — DOI: 10.1136/bmj.h4183
- Weaver CM, Alexander DD, Boushey CJ, et al. (2016). Calcium plus vitamin D supplementation and risk of fractures: an updated meta-analysis from the National Osteoporosis Foundation. Osteoporosis International. — DOI: 10.1007/s00198-015-3386-5
- Chapuy MC, Arlot ME, Duboeuf F, et al. (1992). Vitamin D3 and calcium to prevent hip fractures in elderly women. NEJM. — DOI: 10.1056/NEJM199212033272305
- Boonen S, Lips P, Bouillon R, et al. (2007). Need for additional calcium to reduce the risk of hip fracture with vitamin D supplementation. JCEM. — PubMed
- Heaney RP (2006). Calcium intake and bone health throughout the life course. AJCN. — PubMed
- Bonewald LF (2011). The amazing osteocyte. JBMR. — DOI: 10.1002/jbmr.320
- Boyle WJ, Simonet WS, Lacey DL (2003). Osteoclast differentiation and activation. Nature. — DOI: 10.1038/nature01658
- Reid IR, Bolland MJ (2020). Calcium and/or vitamin D supplementation for the prevention of fragility fractures: who needs it? Nutrients. — DOI: 10.3390/nu12041011
- Jackson RD, LaCroix AZ, Gass M, et al. (2006). Calcium plus vitamin D supplementation and the risk of fractures (WHI). NEJM. — DOI: 10.1056/NEJMoa055218
- WHO Scientific Group on the prevention and management of osteoporosis — PubMed
Research Papers: Cardiovascular
- Bolland MJ, Avenell A, Baron JA, et al. (2010). Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ. — DOI: 10.1136/bmj.c3691
- Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR (2011). Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the WHI dataset and meta-analysis. BMJ. — DOI: 10.1136/bmj.d2040
- Geleijnse JM, Vermeer C, Grobbee DE, et al. (2004). Dietary intake of menaquinone and reduced coronary heart disease (Rotterdam Study). Journal of Nutrition. — DOI: 10.1093/jn/134.11.3100
- Schurgers LJ, Cranenburg EC, Vermeer C (2008). Matrix Gla-protein: the calcification inhibitor in need of vitamin K. Thrombosis and Haemostasis. — PubMed
- Detrano R, Guerci AD, Carr JJ, et al. (2008). Coronary calcium as a predictor of coronary events in four racial or ethnic groups (MESA). NEJM. — DOI: 10.1056/NEJMoa072100
- Greenland P, Blaha MJ, Budoff MJ, et al. (2018). Coronary calcium score and cardiovascular risk. JACC. — DOI: 10.1016/j.jacc.2017.10.099
- Bers DM (2002). Cardiac excitation-contraction coupling. Nature. — DOI: 10.1038/415198a
- Eisner DA, Caldwell JL, Kistamas K, Trafford AW (2017). Calcium and excitation-contraction coupling in the heart. Circulation Research. — DOI: 10.1161/CIRCRESAHA.117.310230
- Reid IR, Bristow SM, Bolland MJ (2015). Calcium supplements: benefits and risks. Journal of Internal Medicine. — DOI: 10.1111/joim.12394
- Beulens JW, Bots ML, Atsma F, et al. (2009). High dietary menaquinone intake and reduced coronary calcification. Atherosclerosis. — DOI: 10.1016/j.atherosclerosis.2008.07.010
Research Papers: Muscle Function
- Berridge MJ, Lipp P, Bootman MD (2000). The versatility and universality of calcium signalling. Nature Reviews Molecular Cell Biology. — DOI: 10.1038/35036035
- Endo M (2009). Calcium-induced calcium release in skeletal muscle. Physiological Reviews. — DOI: 10.1152/physrev.00040.2008
- Gordon AM, Homsher E, Regnier M (2000). Regulation of contraction in striated muscle. Physiological Reviews. — DOI: 10.1152/physrev.2000.80.2.853
- Somlyo AP, Somlyo AV (2003). Ca2+ sensitivity of smooth muscle and nonmuscle myosin II. Physiological Reviews. — DOI: 10.1152/physrev.00023.2003
- MacLennan DH, Kranias EG (2003). Phospholamban: a crucial regulator of cardiac contractility. Nature Reviews Molecular Cell Biology. — DOI: 10.1038/nrm1151
- Catterall WA (2011). Voltage-gated calcium channels. Cold Spring Harbor Perspectives in Biology. — DOI: 10.1101/cshperspect.a003947
- Maughan RJ, Shirreffs SM (2019). Muscle cramping during exercise: causes and solutions. Sports Medicine. — DOI: 10.1007/s40279-019-01162-1
- Lehnart SE, Mongillo M, Bellinger A, et al. (2008). Leaky Ca2+ release channel/ryanodine receptor 2 causes seizures and sudden cardiac death. JCI. — DOI: 10.1172/JCI35346
- Lakatta EG, Maltsev VA, Vinogradova TM (2010). A coupled system of intracellular Ca2+ clocks and surface membrane voltage clocks controls the heart's pacemaker. Circulation Research. — DOI: 10.1161/CIRCRESAHA.109.206078
- Schneider MF, Chandler WK (1973). Voltage dependent charge movement of skeletal muscle. Nature. — DOI: 10.1038/242244a0
Research Papers: Nerve Transmission
- Sudhof TC (2012). Calcium control of neurotransmitter release. Cold Spring Harbor Perspectives in Biology. — DOI: 10.1101/cshperspect.a011353
- Katz B, Miledi R (1967). The timing of calcium action during neuromuscular transmission. Journal of Physiology. — PubMed
- Augustine GJ (2001). How does calcium trigger neurotransmitter release? Current Opinion in Neurobiology. — DOI: 10.1016/S0959-4388(00)00219-6
- Brose N, Petrenko AG, Sudhof TC, Jahn R (1992). Synaptotagmin: a calcium sensor on the synaptic vesicle surface. Science. — DOI: 10.1126/science.1589771
- Ophoff RA, Terwindt GM, Vergouwe MN, et al. (1996). Familial hemiplegic migraine and episodic ataxia type-2 from CACNL1A4 mutations. Cell. — DOI: 10.1016/S0092-8674(00)81373-2
- Vincent A, Lang B, Newsom-Davis J (1989). Autoimmunity to the voltage-gated calcium channel underlies LEMS. Trends in Neurosciences. — DOI: 10.1016/0166-2236(89)90123-3
- Cooper MS, Gittoes NJ (2008). Diagnosis and management of hypocalcaemia. BMJ. — DOI: 10.1136/bmj.39582.589433.BE
- Surmeier DJ, Schumacker PT (2013). Calcium and neuronal vulnerability in Parkinson's disease. JBC. — DOI: 10.1074/jbc.R112.410530
- Berridge MJ (1998). Neuronal calcium signaling. Neuron. — DOI: 10.1016/S0896-6273(00)80510-3
- Cooper EC, Jan LY (1999). Ion channel genes and human neurological disease. PNAS. — DOI: 10.1073/pnas.96.9.4759
Research Papers: Cross-Cutting (Mechanism, Status, Safety)
- Calcium-sensing receptor (CaSR) and parathyroid set-point regulation — PubMed
- Vitamin D and intestinal calcium absorption (TRPV6, calbindin-D9k, PMCA1b) — PubMed
- Magnesium and calcium interaction (PTH secretion and action) — PubMed
- Vitamin K2 / Matrix Gla Protein axis — PubMed
- Boron and calcium retention / bone density — PubMed
- Hypocalcemia clinical diagnosis and management — PubMed
- Hypercalcemia of malignancy and primary hyperparathyroidism — PubMed
- Calcium / phosphate / FGF23 axis in chronic kidney disease — PubMed
- Calcium oxalate kidney stones and dietary calcium — PubMed
- Milk-alkali syndrome — PubMed
External Authoritative Resources
- Linus Pauling Institute — Calcium Micronutrient Information Center — the most authoritative scientific summary of calcium biology, regularly updated
- NIH Office of Dietary Supplements — Calcium Fact Sheet (Health Professionals)
- Harvard T.H. Chan School of Public Health — The Nutrition Source: Calcium
- MedlinePlus — Calcium
- American Heart Association — Coronary Calcium Scan
- PubMed — All calcium / nutrition research (~270,000+ papers)
Connections
- Calcium (Main Page)
- Calcium for Bone Health
- Calcium for Cardiovascular Health
- Calcium for Muscle Function
- Calcium for Nerve Transmission
- All Minerals
- Vitamin D3
- Vitamin K2
- Magnesium
- Phosphorus
- Boron
- Silicon
- Manganese
- Potassium
- Osteoporosis
- Atherosclerosis
- Hypertension
- Arrhythmia
- Hyperparathyroidism
- Kidney Disease
- Collagen
- Milk
- Cramp Prevention
- Magnesium Replenishment