Lipoprotein(a): The Genetic Cardiovascular Risk Factor You Should Test Once in Your Life
Lipoprotein(a), pronounced “lipoprotein little a” and written Lp(a), is an LDL-like particle with a distinctive extra protein called apolipoprotein(a) stitched to it. Lp(a) level is roughly 90 percent genetically determined, remains essentially stable across a lifetime, and confers independent cardiovascular risk that is not captured by any other standard test — including LDL cholesterol, ApoB, or blood pressure. An estimated one in five adults has elevated Lp(a) and most do not know it, because the test is not part of a routine lipid panel.
Elevated Lp(a) is a major risk factor for premature coronary artery disease, stroke, aortic stenosis, and peripheral artery disease. Because the level is stable, the American Heart Association, European Society of Cardiology, and major lipidology societies now recommend measuring Lp(a) at least once in every adult’s lifetime.
Table of Contents
- What Lp(a) Is
- How Lp(a) Drives Disease
- Interpreting Your Level
- Who Should Test
- What You Can Do If It’s High
- Emerging Targeted Therapies
- Connections
- Featured Videos
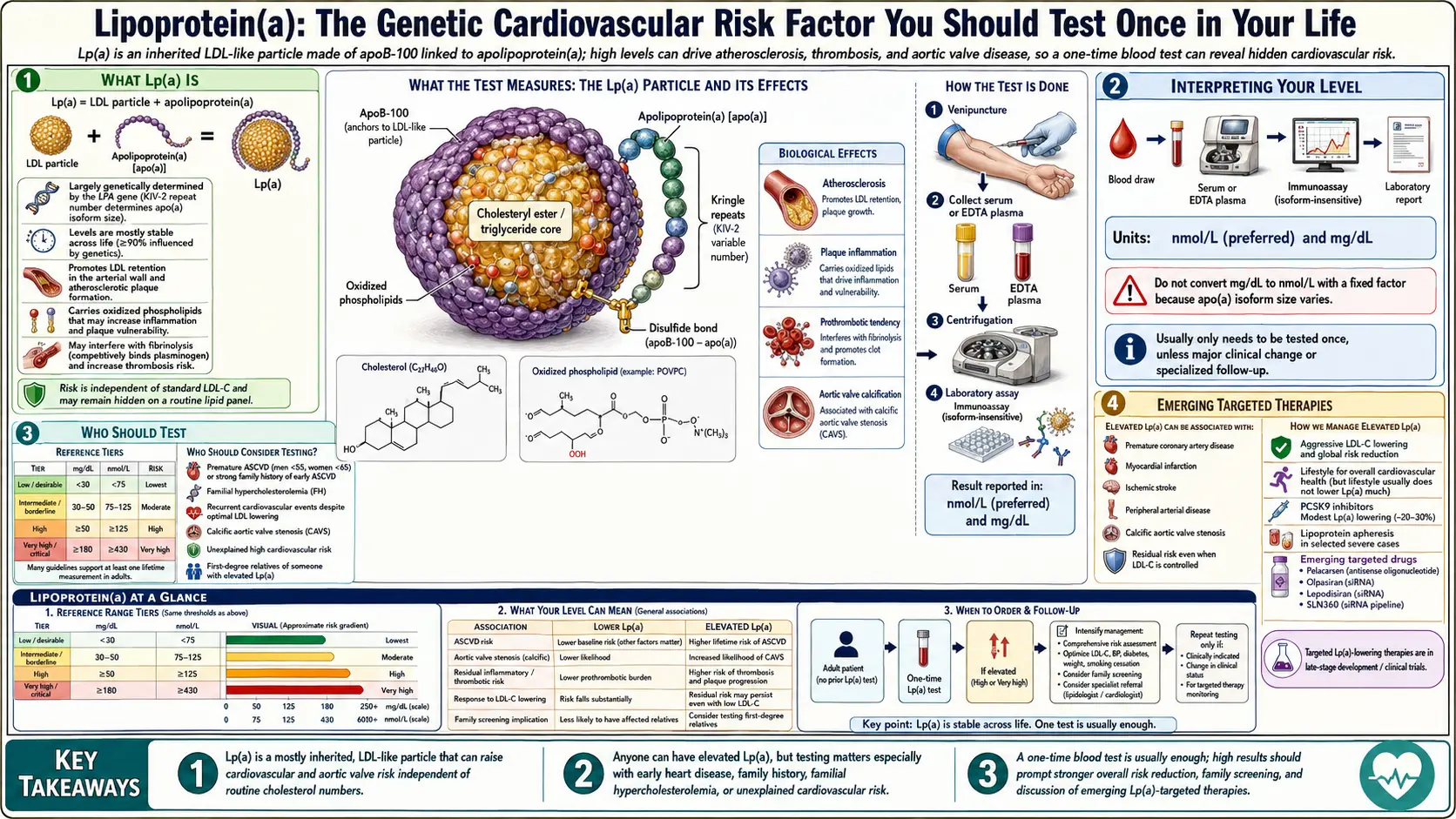
What Lp(a) Is
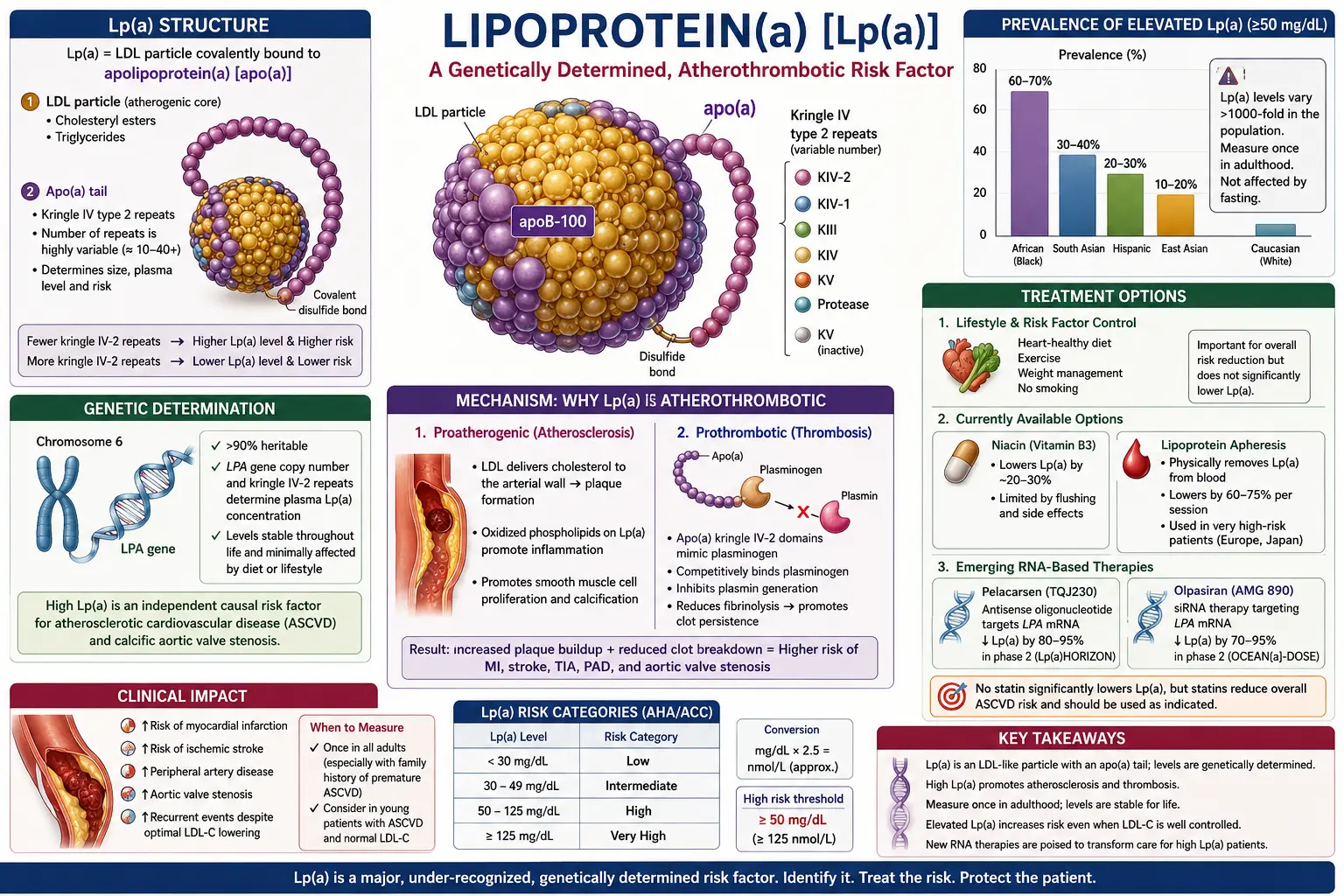
An Lp(a) particle is structurally similar to LDL — a single ApoB-100 molecule wraps a cholesterol-rich core — with one additional protein, apolipoprotein(a), bound by a disulfide bond. Apolipoprotein(a) is a highly variable protein encoded by the LPA gene; the number of kringle-IV repeats in it determines circulating Lp(a) level (shorter isoforms produce higher levels). Population levels span four orders of magnitude, from undetectable to over 300 mg/dL.
How Lp(a) Drives Disease
- Atherosclerosis. Like LDL, Lp(a) can enter the artery wall and deposit cholesterol.
- Thrombosis. Apolipoprotein(a) resembles plasminogen and can interfere with fibrinolysis, promoting clot formation.
- Inflammation. Lp(a) carries oxidized phospholipids, potent drivers of vascular inflammation.
- Aortic valve calcification. Lp(a) is the dominant causal risk factor for calcific aortic stenosis.
Mendelian-randomization studies — which use genetic variation to establish causality — confirm that lifetime Lp(a) exposure causally drives coronary disease and aortic stenosis.
Interpreting Your Level
- <30 mg/dL (<75 nmol/L): Low risk attributable to Lp(a).
- 30–50 mg/dL (75–125 nmol/L): Moderate risk.
- 50–100 mg/dL (125–250 nmol/L): High risk.
- >100 mg/dL (>250 nmol/L): Very high risk; cardiovascular prevention should be intensified.
Units matter: nmol/L is increasingly preferred because it reflects particle concentration. Mass units (mg/dL) can mislead because particle size varies.
Who Should Test
- Every adult, at least once.
- Anyone with a personal or family history of premature cardiovascular disease (<55 in men, <65 in women).
- Anyone with unexplained cardiovascular events despite normal standard risk factors.
- First-degree relatives of a person with elevated Lp(a) — the trait is inherited.
What You Can Do If It’s High
There is no approved drug that specifically targets Lp(a) yet (though several are in late-stage trials — see below). Current management focuses on aggressively reducing every other modifiable cardiovascular risk factor:
- Lower ApoB and LDL-C aggressively — high-intensity statin, ezetimibe, and PCSK9 inhibitors where indicated.
- Blood pressure <120/80.
- Control diabetes, smoking, and insulin resistance.
- Consider low-dose aspirin in very-high-risk individuals after clinician discussion.
- Maintain Mediterranean-style diet, regular exercise, and weight optimization.
- Pursue imaging (coronary calcium, CT angiography, carotid ultrasound) to refine overall risk.
Statins do not lower Lp(a); niacin modestly lowers it but without outcomes benefit. PCSK9 inhibitors lower Lp(a) by roughly 20–30%. Lipoprotein apheresis can acutely lower Lp(a) and is used in extreme cases.
Emerging Targeted Therapies
Three candidate drugs are in phase-3 cardiovascular-outcomes trials:
- Pelacarsen — an antisense oligonucleotide, reduces Lp(a) by 80–90%.
- Olpasiran — a siRNA, similar reductions with infrequent dosing.
- Muvalaplin — an oral small molecule that blocks apolipoprotein(a) assembly.
Results over the coming years will determine whether lowering Lp(a) translates into proportional event reduction.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for Lipoprotein(a) testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Lipoprotein(a) cardiovascular risk — PubMed literature search
- Lp(a) genetics — PubMed literature search
- Lp(a) and atherosclerosis — PubMed literature search
- Lp(a) and aortic stenosis — PubMed literature search
- Pelacarsen Lp(a) lowering trial — PubMed literature search
- Lp(a) assay standardization — PubMed literature search
- PCSK9 inhibitors and Lp(a) — PubMed literature search
- Niacin and Lp(a) — PubMed literature search
- Lp(a) population screening — PubMed literature search
- Lp(a) Mendelian randomization — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- ApoB
- Lipid Panel
- Coronary Calcium Score
- Atherosclerosis
- Coronary Artery Disease
- Cardiovascular Disease
- Stroke
- Peripheral Artery Disease
- Insulin Resistance
- Diabetes
- Omega-3 Fatty Acids
- Anti-Inflammatory Diet
- Calcium
- Full Body MRI
- Soft Plaque and CAC Limitations
- Statin Threshold and CAC
- CAC Zero and the Power of Negative Result
- MESA Risk Calculator and Age Percentiles