CAC Zero: The Strongest "All Clear" in Preventive Cardiology
A coronary calcium score of zero is the single most powerful negative test result in preventive cardiology. In a 50-year-old with otherwise concerning risk factors, a CAC of zero translates to a 10-year cardiovascular event rate below 1% — lower than the average healthy 35-year-old's risk. The clinical effect of a zero score is so strong that current guidelines specifically allow physicians to downgrade statin or aspirin recommendations in patients whose ASCVD calculator suggests intermediate risk but whose CAC is zero. This page explores what zero actually rules out, what it doesn't, who the rare "zero-CAC heart attack" patients are, and how long the negative test result remains reliable.
Table of Contents
- What Zero Rules Out
- 10-Year Event Rate
- The "Warranty Period"
- Who Still Has Events?
- Zero in Younger Adults
- Zero in Older Adults
- Downgrading Therapy with a Zero Score
- When to Re-scan
- Research Papers and References
- Connections
- Featured Videos
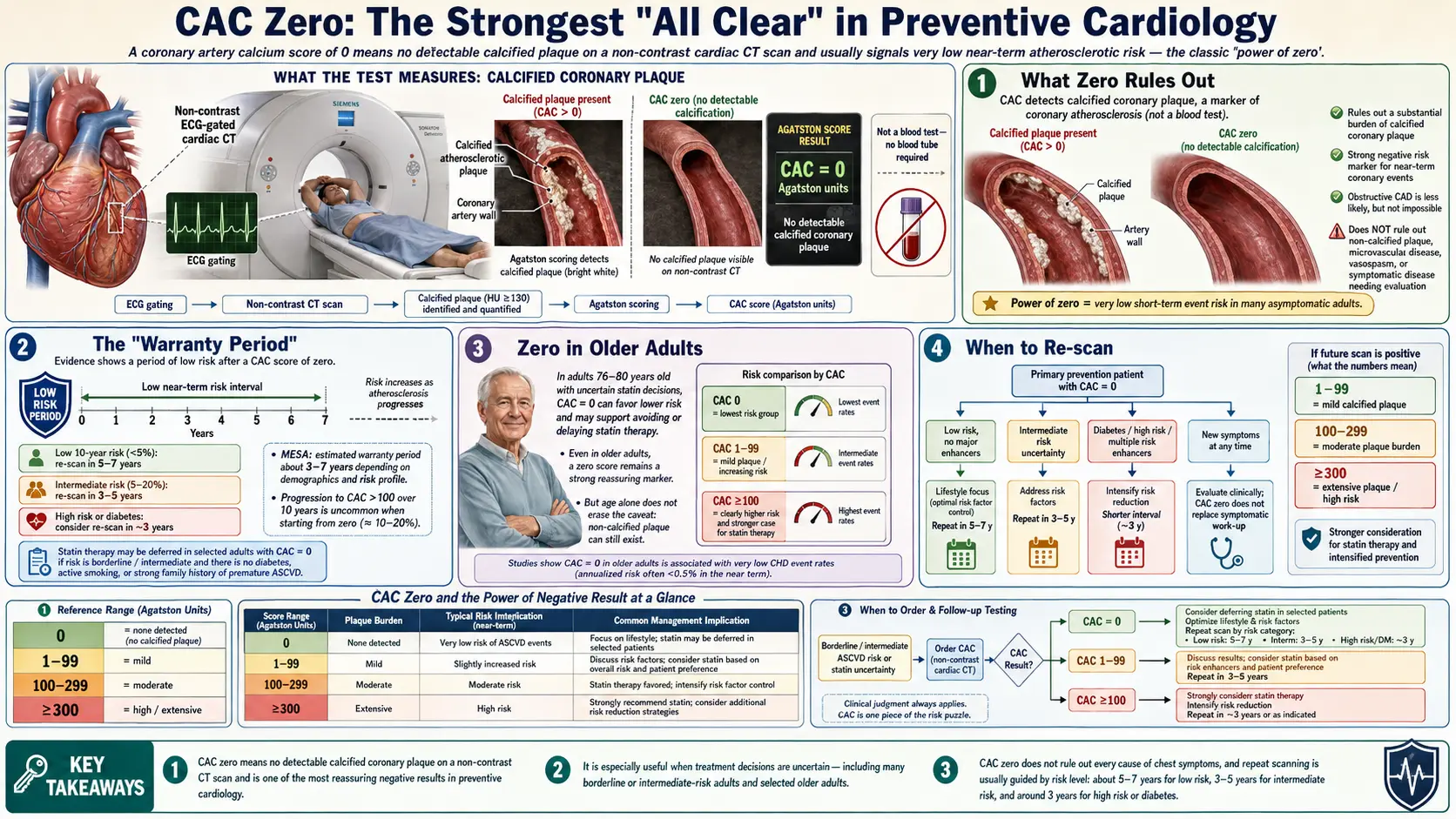
What Zero Rules Out
A CAC of zero rules out, with high confidence:
- Significant calcified atherosclerotic plaque
- Mature atherosclerosis of any duration
- The vast majority of clinically silent obstructive coronary disease
What it does not rule out:
- Soft (non-calcified) plaque, especially in younger patients early in the atherosclerotic process
- Vulnerable plaque (lipid-rich plaque with thin fibrous caps that can rupture without prior calcification)
- Coronary artery spasm, dissection, or microvascular dysfunction
- Non-atherosclerotic causes of cardiac symptoms (HCM, congenital, electrical)
For most middle-aged and older adults, the calcified component is what dominates risk, so CAC = 0 is highly reassuring. For younger adults with strong family history or markedly elevated Lp(a), a complementary CT coronary angiogram (CCTA) may be appropriate to rule out soft plaque. See the Soft Plaque page.
10-Year Event Rate
The published 10-year cardiovascular event rates with CAC = 0 are remarkable for their consistency across cohorts and decades:
- MESA cohort, 10-year CV death/MI — ~1.0% in CAC = 0 patients
- Heinz Nixdorf Recall, 10-year CV events — ~1.5% in CAC = 0
- CONFIRM registry, 5-year mortality — 0.5% in CAC = 0 (despite the cohort being symptomatic referrals)
- Intermediate-risk subgroups — CAC = 0 reduces predicted event rates by 50–70% across most ASCVD risk strata
To put 1% over 10 years in context: that's roughly 0.1% per year, similar to the risk of unintentional injury death in middle-aged adults. Practically speaking, a CAC of zero says: cardiovascular disease is unlikely to be the thing that gets you in the next decade.
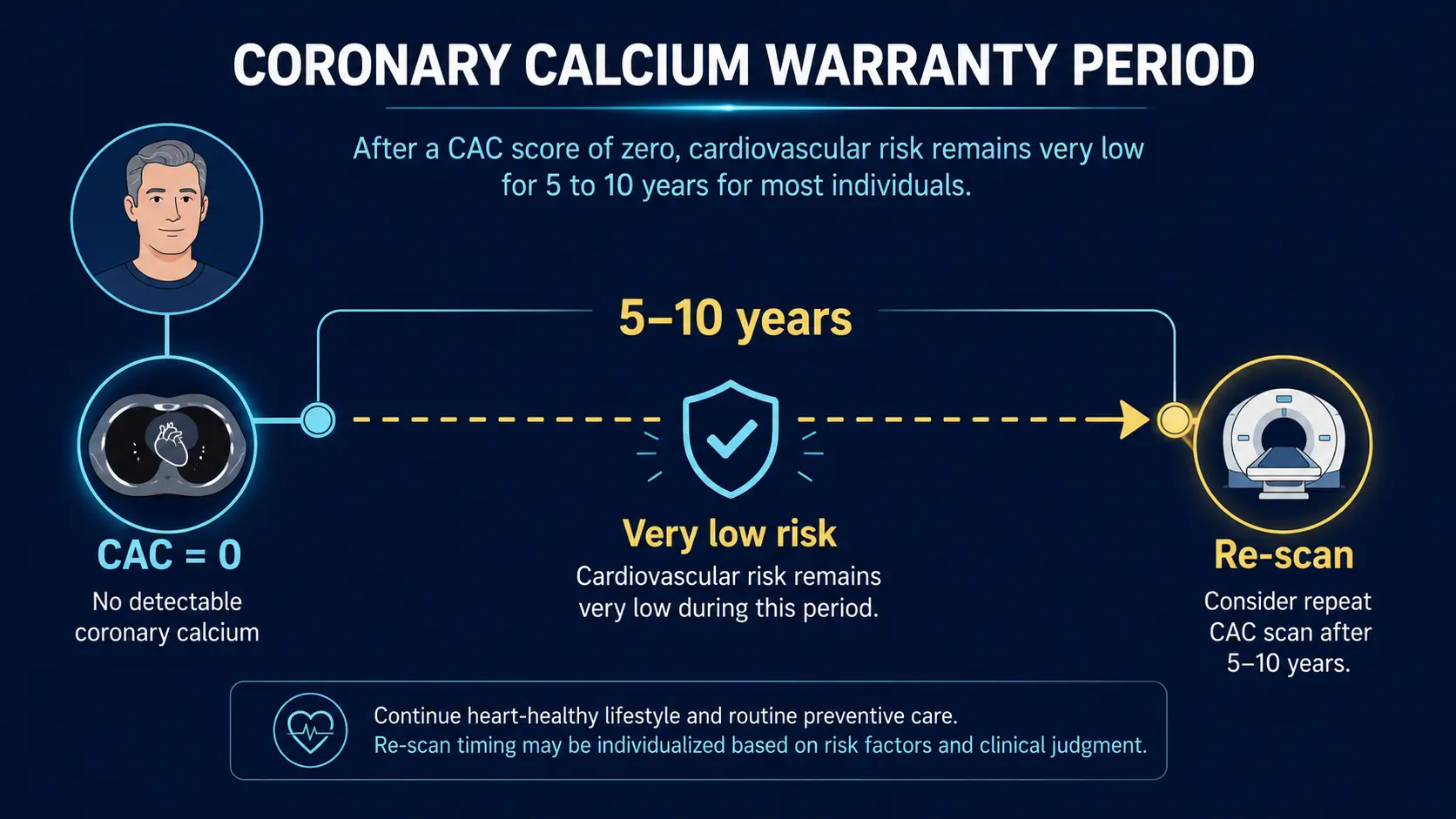
The "Warranty Period"
The phrase "warranty period" refers to the duration over which a CAC of zero remains a reliable negative result. Several key observations:
- The conversion rate from CAC = 0 to CAC > 0 averages 25–30% over 5 years in middle-aged adults with risk factors
- Among those who convert, only a small fraction develop high scores quickly — most go to scores of 1–10 over 5 years
- Annual progression slope is faster in patients with diabetes, family history, or untreated dyslipidemia
- The clinical event-rate "protection" of CAC = 0 attenuates over 10–15 years — useful, but not permanent
Practical interpretation: a CAC of zero is reliably reassuring for 5–10 years in most patients. After that interval, re-imaging is reasonable, especially in patients with persistent risk factors.
Who Still Has Events?
The 1% who do have events with CAC = 0 cluster into recognizable patterns:
- Heavy smokers — smoking accelerates plaque rupture independent of plaque burden
- Cocaine users — vasospastic and pro-thrombotic effects
- Diabetics with poor glycemic control — despite CAC = 0, microvascular and accelerated soft-plaque disease
- Patients with elevated Lp(a) — pro-thrombotic / pro-inflammatory effects on top of any calcium burden
- Familial hypercholesterolemia — can have soft plaque early; CAC = 0 less reassuring in young FH patients
- Connective tissue disease — lupus, RA accelerate plaque rupture
- Acute coronary syndromes from non-atherosclerotic causes — SCAD, vasospasm, cocaine, embolism
These groups warrant additional evaluation despite a CAC = 0. The clinical history matters more than the test result.
Zero in Younger Adults
For an adult under 50 with a CAC of zero:
- The absolute reassurance is stronger than at any other age — 10-year event risk well under 0.5%
- The warranty may be shorter because there is more time for plaque to develop. Re-scan at 5–7 year intervals if risk factors persist
- For very young adults with strong family history (premature CAD before 55 in male first-degree relatives, before 65 in female first-degree relatives) or markedly elevated Lp(a) (>100 nmol/L), CAC = 0 should be supplemented by ApoB and Lp(a) testing, and consideration of CCTA to rule out soft plaque if other risk factors are extreme
Zero in Older Adults
A CAC of zero in someone over 70 is an unusually clean cardiovascular bill of health:
- The absolute event rate is exceptionally low — below the median for adults of any age
- The warranty is longer in absolute terms because the patient has already passed through the highest-risk decade for atherosclerotic events
- Statin therapy in primary prevention can often be deferred or de-escalated
- Aspirin use should be reconsidered — the bleeding risk from aspirin tends to outweigh benefit in CAC = 0 elderly
- The score is a strong argument against assuming "old age = inevitable cardiovascular disease"
Downgrading Therapy with a Zero Score
The 2018 ACC/AHA cholesterol guideline and subsequent updates explicitly support using CAC = 0 to defer statin therapy in adults at intermediate baseline ASCVD risk who would otherwise meet treatment criteria. The pathway:
- Patient has 10-year ASCVD risk between 5% and 19.9% by the pooled cohort equation
- Statin recommendation is "consider with risk discussion" — a borderline call
- CAC scoring is performed
- If CAC = 0, statin can be reasonably deferred and re-evaluation done in 5–10 years
- If CAC > 0, statin is initiated; the higher the score, the more aggressive the management
This pathway is one of the strongest practical reasons to obtain a CAC: it can either confirm the need for therapy or justifiably remove the medication conversation for a substantial portion of patients.
When to Re-scan
General intervals for follow-up CAC after an initial zero result:
- Low baseline risk, clean lifestyle — re-scan in 7–10 years
- Intermediate risk, controlled risk factors — re-scan in 5–7 years
- Diabetes, family history, elevated Lp(a) — re-scan in 3–5 years
- Onset of new risk factor (new diabetes, sustained hypertension, weight gain) — consider earlier re-imaging
- Onset of cardiac symptoms — do not rely on a prior CAC; obtain new evaluation (stress test, CCTA, or troponin as appropriate)
Routine annual or biennial re-imaging is not recommended for CAC = 0 — the calcification process is too slow to track meaningfully on that timeline, and the radiation exposure adds up.
Research Papers and References
- CAC = 0 and 10-year events — PubMed search
- CAC warranty period — PubMed search
- CAC = 0 and statin deferral — PubMed search
- Zero CAC and MI — PubMed search
- Heinz Nixdorf Recall study — PubMed search
Connections
- Coronary Calcium Score
- Soft Plaque and CAC Limitations
- Agatston Score Calculation and Interpretation
- MESA Risk Calculator and Age Percentiles
- Statin Threshold and CAC
- CAC vs Other Cardiac Tests
- CAC in Women and Younger Adults
- Reversal Plaque Stabilization and Lifestyle
- Insurance Cost and Access
- ApoB
- Lipoprotein(a)
- Lipid Panel
- Cardiovascular Disease
- Atherosclerosis
- Calcium
- Full Body MRI