BNP and NT-proBNP: Cardiac Biomarker Guide
BNP (B-type natriuretic peptide) and NT-proBNP are cardiac biomarkers secreted by the heart in response to increased ventricular wall stress and volume overload. They are the cornerstone blood tests for diagnosing acute heart failure in the emergency department, estimating prognosis, and guiding long-term management of patients with established heart failure. A BNP below 100 pg/mL makes heart failure an unlikely cause of breathlessness, while markedly elevated levels confirm the diagnosis and help quantify severity. Understanding the differences between the two assays — their clearance routes, half-lives, and diagnostic cut-points — is essential for interpreting results correctly and for avoiding the two classic traps: false positives in kidney disease and false negatives in obesity.
Interactive Visualization The Heart & Circulation — watch a blood cell make the loop Trace a blood cell through all four chambers and both circuits, with a live ECG, chamber pressures, and an exercise mode. Launch →Table of Contents
- What are BNP and NT-proBNP?
- Biology: How and Why They Are Released
- BNP Diagnostic Thresholds
- NT-proBNP Age-Adjusted Thresholds
- BNP vs NT-proBNP: Key Differences
- Diagnosing Acute Heart Failure in the Emergency Department
- Factors That Affect Levels
- When BNP Is Falsely Low
- Clinical Uses: Diagnosis and Monitoring
- Prognostic Value and Serial Monitoring
- Biomarker-Guided Therapy and the GUIDE-IT Trial
- Interpreting Results in Kidney Disease
- Interpretation Pitfalls
- Research Papers
- Connections
- Featured Videos
What are BNP and NT-proBNP?
BNP (B-type natriuretic peptide) and NT-proBNP (N-terminal pro-B-type natriuretic peptide) are cardiac biomarkers released by the heart when it is under mechanical stress — specifically when the ventricles experience elevated wall tension due to pressure or volume overload. Both are derived from the same precursor molecule (proBNP), and both are measured from a routine blood draw. They are the most clinically useful biomarkers for diagnosing heart failure, particularly in the emergency setting when a patient presents with acute dyspnea.
BNP was first isolated from porcine brain tissue in 1988 — which is where the original name "brain natriuretic peptide" came from. The name is a historical misnomer: in humans the dominant source is the ventricular cardiomyocyte, not the brain. The designation was later revised to "B-type" to distinguish it from ANP (A-type natriuretic peptide), which is secreted mainly by the atria. When ventricular walls are stretched by increased pressure or volume — as happens in heart failure, cardiomyopathy, severe valve disease, or pulmonary hypertension — ventricular cells step up transcription of the BNP gene within minutes to hours.
Functionally, BNP is the heart's own distress signal: it relaxes blood vessels, promotes sodium and water excretion, suppresses the renin-angiotensin-aldosterone system, and damps down sympathetic activation. In other words, BNP is the heart trying to reduce its own workload. Measuring it gives a direct read on how much strain the heart is under, even when physical signs such as edema or a third heart sound are absent or equivocal.
First characterized in the 1980s and 1990s and adopted into routine practice in the early 2000s, natriuretic peptides transformed the evaluation of shortness of breath. Before their widespread adoption, distinguishing cardiac from pulmonary causes of dyspnea required clinical judgment, chest X-ray, and echocardiography — tools that are slow, operator-dependent, or unavailable after hours. A single BNP or NT-proBNP result can provide a rapid, objective answer in minutes.
Biology: How and Why They Are Released
The natriuretic peptide system is a counter-regulatory mechanism against volume and pressure overload:
- Stimulus: Increased wall stress (from elevated filling pressures, volume overload, or myocardial injury) triggers ventricular myocytes — primarily in the left ventricle, with smaller contributions from the right ventricle and atria — to transcribe the NPPB gene (chromosome 1p36). The initial product, preproBNP-134, is processed to proBNP (108 amino acids).
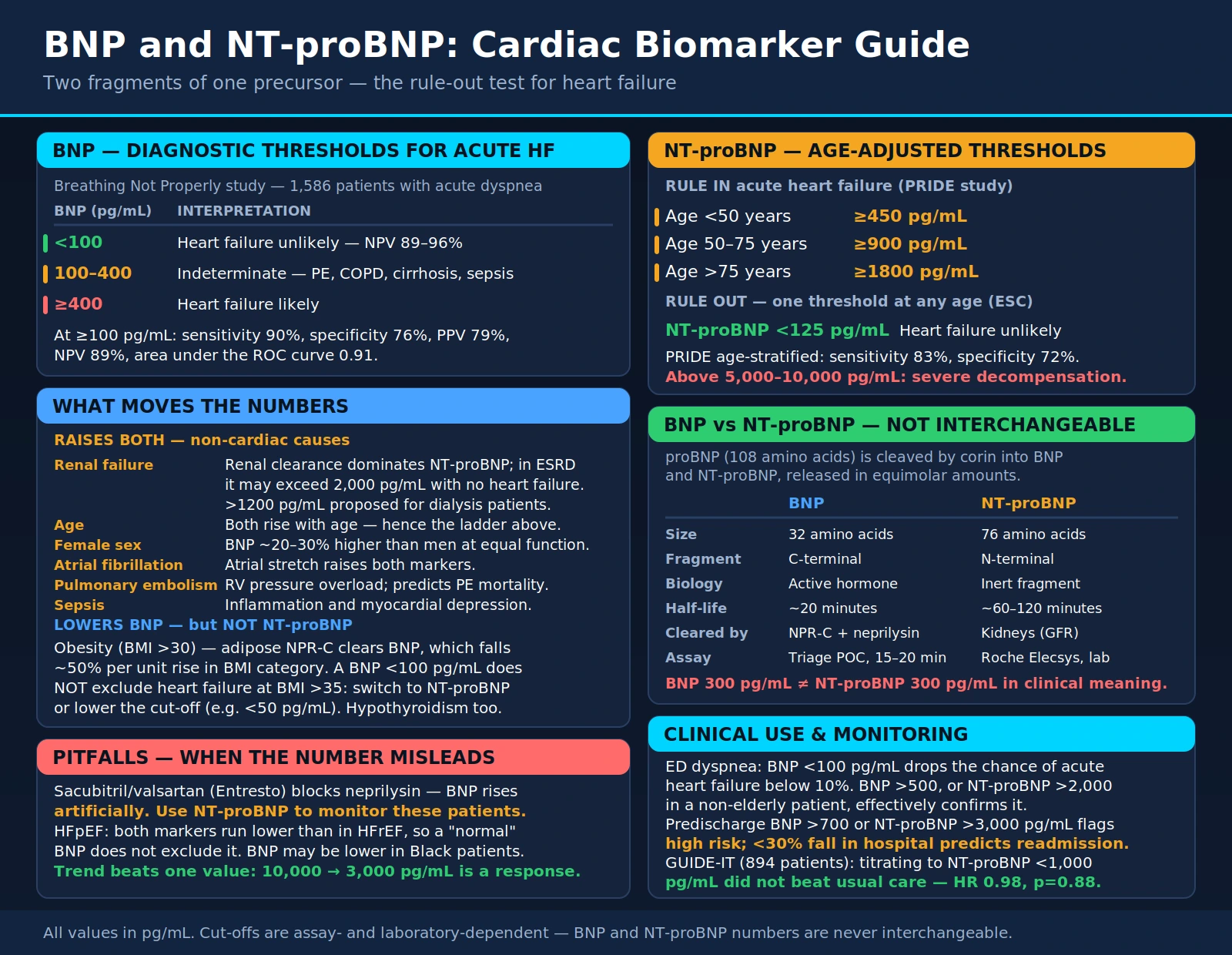
- Cleavage: The serine protease corin, with a contribution from the metalloprotease furin, cleaves proBNP into two fragments: the biologically active BNP-32 (32 amino acids; C-terminal) and the biologically inactive NT-proBNP (76 amino acids; N-terminal). Both fragments are released into the circulation in equimolar amounts.
- Biological effects of BNP: BNP-32 binds natriuretic peptide receptor A (NPR-A) on vascular smooth muscle and renal tubular cells, producing natriuresis (sodium and water excretion), vasodilation (reduced preload and afterload), suppression of the renin-angiotensin-aldosterone system (RAAS), and inhibition of sympathetic nervous system activation. These effects partially counteract the maladaptive neurohormonal activation of heart failure.
- Clearance: BNP is cleared by natriuretic peptide clearance receptor C (NPR-C), which internalizes and degrades it, and by enzymatic cleavage by neprilysin (neutral endopeptidase). NT-proBNP has no known clearance receptor and is eliminated almost exclusively by the kidneys via glomerular filtration.
The differential clearance pathways are clinically important in two directions: because NT-proBNP is renally cleared, its levels rise disproportionately in kidney disease; and because BNP is a neprilysin substrate, its levels rise when neprilysin is inhibited by sacubitril.
Stimulus-Response Kinetics
BNP gene transcription begins within about 30 minutes of acute ventricular stretch, and measurable BNP rises in blood within 1–2 hours of an acute hemodynamic insult. That responsiveness cuts both ways. It makes BNP an excellent real-time indicator of acute decompensation, and it makes levels fall quickly once the hemodynamic burden is relieved — for example after aggressive diuresis — so serial measurements track treatment response usefully. It also means a very early draw in a sudden catastrophe may be taken before the peptide has had time to rise. NT-proBNP, with its longer half-life, has a flatter plateau and slower decay, reflecting changes over roughly a 24–48 hour window rather than hour to hour.
BNP Diagnostic Thresholds
BNP thresholds for acute heart failure (AHF) diagnosis are well-validated across large multicenter studies. The landmark Breathing Not Properly Multinational Study (Maisel et al., 2002) enrolled 1,586 patients with acute dyspnea and produced the three-zone decision ladder still used at the bedside today.
The Three-Zone BNP Decision Ladder
| BNP Level | Interpretation | Clinical Action |
|---|---|---|
| <100 pg/mL | Heart failure unlikely | Look for non-cardiac causes of dyspnea |
| 100–400 pg/mL | Gray zone — indeterminate | Consider other cardiac conditions, pulmonary embolism, CKD; echocardiogram helpful |
| >400 pg/mL | Heart failure likely | Initiate heart failure therapy; echocardiogram to characterize |
- BNP <100 pg/mL: Heart failure unlikely (negative predictive value 89–96%). In this range, dyspnea is almost certainly non-cardiac in origin.
- BNP 100–400 pg/mL: Indeterminate zone — heart failure possible but other causes must be considered (acute cor pulmonale from pulmonary embolism, COPD exacerbation with right heart strain, cirrhosis, sepsis). Clinical correlation essential.
- BNP ≥400 pg/mL: Heart failure likely.
- BNP ≥100 pg/mL (primary threshold): Sensitivity 90%, specificity 76%, positive predictive value 79%, negative predictive value 89% for AHF. Area under the ROC curve 0.91.
A note on the widely quoted "96% negative predictive value": in the Breathing Not Properly paper that figure belongs to BNP levels below 50 pg/mL, not below 100 pg/mL. At the 100 pg/mL cut-point the study reported an overall diagnostic accuracy of 83.4% and a negative predictive value of 89%. Both numbers are correct; they simply describe different operating points, and quoting 96% for the 100 pg/mL threshold overstates how safely that value excludes heart failure.
For ruling out heart failure, BNP <100 pg/mL is the most useful operating point due to its high sensitivity. For ruling in heart failure, higher thresholds (≥400–500 pg/mL) increase specificity.
NT-proBNP Age-Adjusted Thresholds
NT-proBNP thresholds are more complex because NT-proBNP levels increase with age even in healthy individuals (due to declining GFR and increased ventricular stiffness). The PRIDE study established the first two age tiers in a single-center cohort of 600 dyspneic patients, and the four-site International Collaborative of NT-proBNP (ICON) pooled analysis of 1,256 patients added the oldest tier and validated the full ladder.
Age-Stratified Cut-Points for Acute Heart Failure
| Age Group | Rule-In Threshold (HF Likely) | Rule-Out Threshold (HF Unlikely) |
|---|---|---|
| Under 50 years | >450 pg/mL | <300 pg/mL |
| 50–75 years | >900 pg/mL | <300 pg/mL |
| Over 75 years | >1,800 pg/mL | <300 pg/mL |
Used together, the three rule-in cut-points yielded 90% sensitivity and 84% specificity for acute heart failure in the ICON analysis. The rule-in values climb with age because NT-proBNP rises physiologically with aging — declining renal clearance plus age-related ventricular stiffening — even in people with no heart failure at all.
Rule-Out Thresholds
- Acute setting — NT-proBNP <300 pg/mL: A single age-independent threshold. In ICON it carried a 98% negative predictive value for excluding acute heart failure; in PRIDE the negative predictive value was 99%. Below 300 pg/mL, acute heart failure is effectively off the table regardless of the patient's age.
- Non-acute / outpatient setting — NT-proBNP <125 pg/mL: The European Society of Cardiology uses a lower threshold when heart failure is suspected in a stable ambulatory patient rather than an acutely breathless one, because chronic compensated heart failure produces smaller elevations than acute decompensation.
These two numbers are not in conflict — they answer different questions. Use 300 pg/mL to clear an acutely dyspneic patient in the emergency department; use 125 pg/mL to clear a stable outpatient being screened for chronic heart failure.
The higher the NT-proBNP, the more likely the diagnosis of AHF — values above 5,000–10,000 pg/mL indicate severe, decompensated disease with high short-term mortality risk. In the ICON cohort, a presenting NT-proBNP above 5,180 pg/mL was strongly predictive of death within 76 days.
Obesity Adjustment
Both BNP and NT-proBNP run lower in obese patients even when heart failure is unquestionably present, so standard cut-points lose sensitivity in exactly the population most likely to be short of breath. The Breathing Not Properly obesity analysis (Daniels et al., 2006) recalculated the BNP cut-point needed to preserve 90% sensitivity across body-mass strata:
- Lean patients: 170 pg/mL (a higher cut-point can be used here to gain specificity).
- Overweight and obese patients: 110 pg/mL.
- Severely or morbidly obese patients: 54 pg/mL.
The practical consequence is that a "normal" BNP in a severely obese, breathless patient is not reassuring. Mean BNP among patients with confirmed acute heart failure fell from 643 pg/mL in lean patients to 462 in the overweight/obese group and 247 in the severely/morbidly obese group in that same analysis.
BNP vs NT-proBNP: Key Differences
Comparison of Key Properties
| Property | BNP | NT-proBNP |
|---|---|---|
| Biological activity | Active hormone (vasodilatory, natriuretic) | Inactive fragment |
| Plasma half-life | ~20 minutes | ~60–120 minutes |
| Clearance route | NPR-C receptor + neprilysin | Renal glomerular filtration |
| Effect of sacubitril/valsartan | Artificially elevated (neprilysin inhibited) | Unaffected — preferred for monitoring on Entresto |
| Effect of CKD/ESRD | Mildly elevated (clearance less GFR-dependent) | Markedly elevated — adjust interpretation with eGFR |
| Effect of obesity | Suppressed — use ~54 pg/mL cut-point in severe obesity | Also suppressed; similar caution applies |
| Rule-out cut-off | 100 pg/mL (single threshold) | 300 pg/mL acute; 125 pg/mL non-acute |
| Rule-in cut-off | 400 pg/mL | Age-stratified (450 / 900 / 1,800 pg/mL) |
| Stability in sample | Less stable (short half-life) | More stable — better for delayed processing |
Biological Activity
- BNP: Biologically active hormone; exerts natriuretic, vasodilatory, and neurohumoral effects. Its own activity means levels can be lower in compensated heart failure than expected.
- NT-proBNP: Biologically inert fragment; reflects cardiac stress more directly without the complicating feedback of its own physiological activity.
Half-Life
- BNP: ~20 minutes. Levels change rapidly with hemodynamic changes or treatment — useful for real-time monitoring during acute hospitalization.
- NT-proBNP: ~60–120 minutes. More stable; useful for monitoring over days to weeks; less susceptible to short-term fluctuations. Its longer survival in the circulation also means it accumulates to higher absolute concentrations than BNP in the same patient at the same moment.
Effect of Neprilysin Inhibition (Sacubitril/Valsartan)
Sacubitril/valsartan (Entresto) — the cornerstone GDMT drug for HFrEF — works by inhibiting neprilysin, which is one of the clearance pathways for BNP. This means BNP levels rise substantially in patients taking sacubitril/valsartan and cannot be used to monitor disease severity or guide titration. NT-proBNP is cleared by the kidneys (not neprilysin) and therefore remains a valid monitoring biomarker in patients on sacubitril/valsartan.
Clinical rule: Always use NT-proBNP (not BNP) to monitor heart failure severity in patients taking sacubitril/valsartan.
Assay Availability
- BNP: Primarily measured by Biosite/Alere Triage point-of-care and laboratory immunoassays; result in 15–20 minutes at bedside.
- NT-proBNP: Primarily Roche Elecsys immunoassay; requires laboratory processing but is widely available in hospitals.
Clinical Bottom Line on Test Selection
Use whichever assay your institution runs, and do not order both at once — dual testing adds cost and creates interpretive confusion without adding information. For patients on sacubitril/valsartan, always use NT-proBNP. For patients with advanced CKD (eGFR <30 mL/min) both tests are elevated, but BNP is somewhat easier to interpret because its clearance is less renally dependent. For serial monitoring, stay with the same assay throughout a patient's care: the two tests are not interchangeable numerically — a BNP of 300 pg/mL and an NT-proBNP of 300 pg/mL mean very different things — and switching mid-course invalidates the trend.
Diagnosing Acute Heart Failure in the Emergency Department
The landmark application of natriuretic peptide testing was the emergency evaluation of acute breathlessness. In the Breathing Not Properly Multinational Study, BNP measurement was more accurate on its own than any single item of history, physical examination, or routine laboratory testing for identifying heart failure as the cause of dyspnea, and it added significant independent predictive power on top of the clinician's assessment.
Differential Diagnosis of Dyspnea: Where BNP Fits
Acute dyspnea has a broad differential: acute decompensated heart failure (ADHF), COPD exacerbation, asthma, pneumonia, pulmonary embolism, anemia, and anxiety. A natriuretic peptide is used as a rapid triage tool that pushes the workup toward or away from a cardiac cause:
- BNP <100 pg/mL: Cardiac dyspnea is very unlikely. Focus the workup on pulmonary, thromboembolic, hematologic, or musculoskeletal causes.
- BNP 100–400 pg/mL: Indeterminate. Could reflect mild or treated heart failure, heart failure with preserved ejection fraction, right heart strain from pulmonary embolism, cor pulmonale, or a non-cardiac cause of elevation. Echocardiogram is the next step.
- BNP >400 pg/mL: ADHF is the most likely diagnosis. Begin diuresis and obtain an echocardiogram to characterize systolic versus diastolic dysfunction.
Heart Failure with Preserved Ejection Fraction (HFpEF)
HFpEF — diastolic heart failure — is increasingly common and diagnostically awkward because the ejection fraction is normal (≥50%) on echocardiogram. Natriuretic peptide levels in HFpEF are typically lower than in HFrEF at a comparable symptom burden, but they are still usually elevated above the 100 pg/mL threshold during acute decompensation. The practical rule: do not use a BNP in the 100–300 pg/mL range to exclude HFpEF in a clinically suggestive presentation. NT-proBNP performed well for HFpEF in the PRIDE cohort once age-stratified cut-points were applied.
Acute Flash Pulmonary Edema — A Special Case
In acute severe mitral regurgitation — ruptured chordae tendineae, or papillary muscle rupture complicating a myocardial infarction — flash pulmonary edema can develop within minutes. BNP may be paradoxically normal or only mildly elevated in the first few hours, because ventricular wall stress has not yet had time to drive enough peptide synthesis. This is the one presentation where the clinical picture, chest X-ray, and emergent echocardiography must drive management rather than waiting on a biomarker. A repeat measurement 6–12 hours later will usually show a dramatic rise, by which point the diagnosis should already have been made on other grounds.
Factors That Affect Levels
An elevated natriuretic peptide is not synonymous with heart failure. Many conditions raise BNP and NT-proBNP through ventricular wall stress, impaired clearance, or inflammatory cytokine-driven upregulation of the BNP gene — and several non-disease factors shift the baseline.
Cardiac Conditions Other Than Heart Failure
- Atrial fibrillation: Atrial stretch and rapid ventricular rate elevate both markers even without structural heart disease. BNP in atrial fibrillation is typically two to three times normal but rarely exceeds 400 pg/mL unless heart failure coexists.
- Acute myocardial infarction: Myocardial necrosis and the resulting wall motion abnormalities drive BNP up within 24 hours of infarction. Peak post-MI BNP correlates with infarct size and the severity of left ventricular dysfunction.
- Myocarditis: Inflammatory injury to cardiomyocytes produces an acute rise that mirrors the degree of ventricular dysfunction.
- Hypertrophic cardiomyopathy: Chronically elevated filling pressures and outflow tract obstruction raise BNP; baseline values often sit in the 200–600 pg/mL range.
- Cardiac tamponade and constrictive pericarditis: External compression of the ventricles alters wall stress signaling.
Pulmonary and Vascular Conditions
- Pulmonary embolism: Acute right ventricular strain from a large PE elevates BNP substantially, often above 400 pg/mL. BNP above roughly 90 pg/mL in confirmed PE predicts adverse in-hospital outcomes such as right ventricular dysfunction and the need for thrombolysis. This is a leading source of false positives in the emergency dyspnea workup.
- Pulmonary arterial hypertension: Chronic right heart pressure overload produces persistent elevation. Serial BNP is used as an endpoint in PAH treatment trials.
- ARDS: Severe acute lung injury with hypoxia causes right ventricular stress and cytokine-mediated release.
- High-altitude exposure: Hypoxic pulmonary vasoconstriction raises right ventricular afterload, elevating BNP in climbers ascending above roughly 4,500 meters.
Systemic and Renal Conditions
- Renal failure (CKD/ESRD): NT-proBNP rises steeply with declining GFR because renal clearance is its dominant elimination pathway. Dialysis patients commonly run five to ten times the normal upper limit with no heart failure at all, and NT-proBNP may exceed 2,000 pg/mL in that setting. A GFR-adjusted rule-in threshold of NT-proBNP >1,200 pg/mL has been validated for patients with eGFR below 60 mL/min/1.73 m². BNP is less affected because its clearance is not primarily renal, but it is still modestly elevated.
- Sepsis and critical illness: Septic cardiomyopathy and the inflammatory cytokine surge of critical illness — particularly interleukin-6 and TNF-alpha — stimulate BNP gene expression in cardiomyocytes even without primary cardiac dysfunction.
- Thyrotoxicosis: Excess thyroid hormone raises cardiac output and heart rate, loading the ventricles and elevating BNP. Hypothyroidism can push levels the other way.
- Liver cirrhosis with ascites: Portal hypertension with splanchnic vasodilation increases effective cardiac output and wall stress.
Demographic Factors
- Age: Both biomarkers increase with age; the age-adjusted NT-proBNP thresholds above exist precisely to handle this.
- Female sex: Women have ~20–30% higher BNP levels than men at comparable cardiac function. Estrogen upregulates BNP gene expression while testosterone suppresses it, and post-menopausal women — particularly those not on hormone therapy — fall in between. Sex-specific diagnostic thresholds have been proposed but are not yet in general guideline use.
- Race and ethnicity: BNP levels may be lower in Black patients than in White patients at equivalent cardiac function; the mechanism is incompletely understood.
The Framingham Heart Study analysis by Vasan and colleagues showed that natriuretic peptides are elevated in community-dwelling people with asymptomatic left ventricular hypertrophy and systolic dysfunction — a reminder that an unexplained elevation may reflect genuine subclinical cardiac disease long before symptoms appear, rather than a spurious result.
When BNP Is Falsely Low
Recognizing false positives matters, but the more dangerous error is a falsely reassuring result — a value below the diagnostic threshold in a patient who genuinely has heart failure.
Obesity — the Most Important Pitfall
The single most clinically significant cause of a falsely low BNP is obesity. Adipose tissue expresses natriuretic peptide clearance receptors (NPR-C) that actively strip BNP out of the circulation, and adipose-derived humoral factors may additionally suppress cardiac BNP gene expression. Mehra and colleagues found that obese patients with confirmed systolic heart failure carried BNP values roughly 40–50% lower than lean patients with equivalent hemodynamic severity. The clinical implication is direct: do not apply the standard 100 pg/mL BNP rule-out threshold to an obese patient. Use the body-mass-adjusted cut-points above, or switch to NT-proBNP — which is suppressed in obesity as well, though less severely and by a less well-characterized mechanism.
Early or Compensated Heart Failure
Patients with mild, stable, well-compensated chronic heart failure on optimal therapy — particularly RAAS inhibitors and beta-blockers — may sit below 100 pg/mL while hemodynamically stable. This is not really a false negative. BNP reports real-time wall stress; when therapy is working, wall stress is low and BNP falls toward normal even though the underlying structural disease persists. It does mean a single normal value cannot be used to say a patient never had heart failure.
Flash Pulmonary Edema from Acute Valvular Catastrophe
As above: in sudden severe mitral or aortic regurgitation the ventricle has not had time to mount a full response in the first 2–4 hours. A BNP drawn in the first hour of presentation can be misleadingly low.
Patients on Sacubitril/Valsartan
Sacubitril inhibits neprilysin and therefore raises BNP — but in the context of effective therapy, the higher BNP does not signal worsening heart failure. NT-proBNP, which neprilysin does not degrade, typically falls on effective sacubitril/valsartan therapy. This is not a false low in the strict sense, but it is the same failure mode in reverse: reading BNP in an ARNI-treated patient produces a number that does not mean what it appears to mean.
Clinical Uses: Diagnosis and Monitoring
1. Acute Dyspnea — Emergency Department Diagnosis
The primary indication. When a patient arrives in the ED with shortness of breath, BNP or NT-proBNP rapidly stratifies probability of acute heart failure. A BNP <100 pg/mL reduces the likelihood of AHF to <10%, allowing focus on pulmonary, thromboembolic, or other causes. A markedly elevated value (BNP >500, NT-proBNP >2,000 in a non-elderly patient) in the correct clinical context effectively confirms AHF and allows prompt diuresis.
2. Prognostication in Established Heart Failure
Persistently elevated or rising natriuretic peptides predict adverse outcomes (hospitalization, death). Failure to achieve at least a 30% reduction in BNP/NT-proBNP during AHF hospitalization portends higher 30-day readmission risk. Predischarge BNP >700 pg/mL or NT-proBNP >3,000 pg/mL identifies high-risk patients who benefit from intensified follow-up.
3. Guiding GDMT Titration
Serial NT-proBNP (preferred over BNP in GDMT-treated patients) guides titration of evidence-based therapies (ACEi/ARB/ARNI, beta-blockers, MRAs, SGLT2 inhibitors). Goal-directed medical therapy reduces natriuretic peptides over weeks to months; target NT-proBNP <1,000 pg/mL is a reasonable clinical endpoint in HFrEF outpatients.
4. Screening for Asymptomatic LV Dysfunction
Population screening data suggest elevated NT-proBNP in asymptomatic individuals identifies those at higher risk of incident heart failure and cardiovascular events. The STOP-HF trial demonstrated that BNP-guided screening and multidisciplinary care reduced incident heart failure compared to usual care. The Framingham Heart Study made the same point observationally a decade earlier, showing that plasma natriuretic peptides could pick out community-dwelling adults with left ventricular hypertrophy and systolic dysfunction before any symptoms appeared.
Prognostic Value and Serial Monitoring
BNP and NT-proBNP are among the most powerful prognostic biomarkers in cardiovascular medicine. Across cohort studies and randomized trials, higher levels at admission for acute decompensated heart failure independently predict:
- Longer length of hospital stay
- Higher 30-day and 1-year mortality
- Higher risk of heart failure re-hospitalization within 60 days
- Need for ICU-level care, mechanical circulatory support, or transplant evaluation
Predischarge BNP as a Discharge Safety Check
Logeart and colleagues studied 190 patients hospitalized for decompensated heart failure and found that predischarge BNP was the strongest predictor of readmission and death at six months — stronger than clinical signs of congestion or NYHA class at discharge. Patients sent home with a BNP still above 700 pg/mL carried roughly two and a half times the risk of an adverse event within six months compared with those discharged below 350 pg/mL. Many centers now treat a predischarge natriuretic peptide as a discharge safety criterion after an admission for acute decompensation.
Trend Beats Absolute Value
A falling number in a patient who feels better is good news even when it is still nominally abnormal. A patient whose NT-proBNP drops from 10,000 to 3,000 pg/mL over a hospitalization is responding to treatment, notwithstanding that 3,000 pg/mL remains "elevated." Conversely, a plateau or rise during diuresis should prompt reassessment rather than reassurance.
Biomarker-Guided Therapy and the GUIDE-IT Trial
A natural question follows from the prognostic data: if a high natriuretic peptide predicts bad outcomes, does treating to a target level improve them? Several trials have tested titrating heart failure therapy against an NT-proBNP goal versus usual symptom-guided care, with genuinely mixed results.
The Earlier Guided-Therapy Trials
- Troughton et al., 2000 (Christchurch pilot): The original proof-of-concept trial. Titrating therapy against plasma N-BNP concentrations reduced total cardiovascular events compared with clinical guidance in patients with impaired systolic function. Small, single-center, but influential.
- PRIMA (Eurlings et al., 2010): Managed chronic heart failure against each patient's own individually-set NT-proBNP target. The primary endpoint — days alive outside hospital — did not differ significantly from clinically guided care.
- SIGNAL-HF (Persson et al., 2010): Tested NT-proBNP-guided management in Swedish primary care. Doses of beta-blockers and RAAS blockers were pushed toward target in both arms, and the composite primary endpoint showed no significant difference (p=0.28). The authors concluded that education plus structured guideline-based treatment achieved as much as biomarker guidance added on top.
- PROTECT (Januzzi et al., 2011): A single-center trial of 151 patients with heart failure from LV systolic dysfunction, randomized to standard care versus standard care plus a goal of reducing NT-proBNP to ≤1,000 pg/mL. Total cardiovascular events were significantly lower in the NT-proBNP arm — 58 versus 100 events (p=0.009; logistic odds for events 0.44) — with better quality of life and more favorable left ventricular remodeling.
GUIDE-IT — The Definitive Trial
The GUIDE-IT trial (Guiding Evidence-Based Therapy Using Biomarker Intensified Treatment in Heart Failure) was the large multicenter test of the strategy. It planned to randomize 1,100 patients with HFrEF (EF ≤40%), recent elevated natriuretic peptides, and a prior heart failure event across 45 sites in the United States and Canada, to:
- NT-proBNP-guided therapy: Titration of GDMT targeting NT-proBNP <1,000 pg/mL.
- Usual care: Guideline-based management with emphasis on titrating proven neurohormonal therapies, without specific biomarker targets.
Primary finding: The data and safety monitoring board stopped the trial for futility after 894 patients had been enrolled and followed for a median of 15 months. The primary composite endpoint of time-to-first heart failure hospitalization or cardiovascular death occurred in 164 patients (37%) in each arm (adjusted HR 0.98, 95% CI 0.79–1.22; p=0.88). No secondary endpoint differed, and the reduction in NT-proBNP over time was similar in both groups.
Key lesson: Biomarker-guided titration did not outperform usual care when both arms received adequate GDMT intensification. The trial does not negate the prognostic value of NT-proBNP — patients who achieved NT-proBNP <1,000 pg/mL in either arm had significantly better outcomes. Rather, it suggests that achieving NT-proBNP reduction is a marker of successful GDMT titration, not an independent driver when titration is already aggressive. NT-proBNP remains a valuable monitoring tool, and the <1,000 pg/mL target continues to be used clinically.
Where the Guidelines Landed
The 2022 ACC/AHA/HFSA heart failure guideline gives natriuretic peptide-guided therapy a Class IIa recommendation — "reasonable" — for reducing hospitalization in selected outpatients with HFrEF, alongside Class I recommendations for using natriuretic peptides to diagnose or exclude heart failure and to establish prognosis. That is a deliberate downgrade in enthusiasm relative to the pre-GUIDE-IT era: the biomarker is firmly established for diagnosis and risk stratification, and merely optional as a titration target.
Interpreting Results in Kidney Disease
Kidney disease is the most common reason a natriuretic peptide is elevated in a patient who is not in heart failure, and it is where interpretation goes wrong most often.
The Breathing Not Properly renal sub-analysis (McCullough et al., 2003) stratified 1,452 dyspneic patients by estimated GFR and showed that the optimal BNP cut-point climbs as kidney function falls — approximately 70 pg/mL at eGFR ≥90, 104 pg/mL at eGFR 60–89, 201 pg/mL at eGFR 30–59, and 225 pg/mL at eGFR <30 mL/min/1.73 m². Discrimination remained good throughout (area under the ROC curve 0.81–0.91), which is the important point: BNP does not stop working in CKD, it simply needs a higher bar. The correlation between BNP and eGFR is real but weak, so renal impairment alone does not account for a markedly elevated value.
NT-proBNP is more strongly affected, because the kidney is essentially its only exit route. The PRIDE renal analysis (Anwaruddin et al., 2006) found that the standard age-based cut-points of 450 and 900 pg/mL performed well (85% sensitivity, 88% specificity) in patients with eGFR ≥60, but that a substantially higher cut-point of 1,200 pg/mL was needed once eGFR fell below 60 mL/min/1.73 m² (89% sensitivity, 72% specificity). Even so, NT-proBNP remained the strongest independent predictor of 60-day mortality in that cohort, including among the patients with reduced GFR. In dialysis-dependent patients, values of several thousand pg/mL can be the individual's baseline; only a substantial rise above that patient's own established norm should raise concern for superimposed decompensation.
Interpretation Pitfalls
- Obesity and low BNP: Do not use BNP <100 pg/mL to exclude heart failure in patients with BMI >35. Switch to NT-proBNP or lower the exclusion threshold to the body-mass-adjusted value (approximately 54 pg/mL in severe obesity).
- Sacubitril/valsartan and BNP: BNP is artificially elevated; always use NT-proBNP in these patients.
- Renal failure and NT-proBNP: Even modest CKD (eGFR 30–60) significantly elevates NT-proBNP. Use the higher GFR-adjusted threshold, or BNP, in CKD patients.
- Race/ethnicity: BNP levels may be lower in Black patients than White patients at equivalent cardiac function; mechanism incompletely understood.
- Preserved vs reduced EF: Both BNP and NT-proBNP are typically lower in HFpEF than HFrEF at comparable symptom burden — a BNP within the "normal" range does not exclude HFpEF.
- Very early presentation: In flash pulmonary edema from an acute valvular catastrophe, a first-hour BNP can be normal. Do not let it override the clinical picture.
- Mixing assays: Never compare a BNP value against an NT-proBNP value, or switch assays mid-course, and expect the trend to mean anything.
- Do not use single absolute values alone: Trend (serial measurements) and clinical context are as important as any single threshold. A patient whose NT-proBNP falls from 10,000 to 3,000 during hospitalization is responding to therapy even though 3,000 pg/mL is still "elevated."
Research Papers
The peer-reviewed studies below established the diagnostic, prognostic, and treatment-guiding roles of BNP and NT-proBNP. Every PMID has been checked against PubMed.
- Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347(3):161–167. PMID 12124404
- Januzzi JL Jr, Camargo CA, Anwaruddin S, et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol. 2005;95(8):948–954. PMID 15820160
- Januzzi JL, van Kimmenade R, Lainchbury J, et al. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256 patients (ICON). Eur Heart J. 2006;27(3):330–337. PMID 16293638
- Daniels LB, Clopton P, Bhalla V, et al. How obesity affects the cut-points for B-type natriuretic peptide in the diagnosis of acute heart failure. Results from the Breathing Not Properly Multinational Study. Am Heart J. 2006;151(5):999–1005. PMID 16644321
- Mehra MR, Uber PA, Park MH, et al. Obesity and suppressed B-type natriuretic peptide levels in heart failure. J Am Coll Cardiol. 2004;43(9):1590–1595. PMID 15120816
- Krauser DG, Lloyd-Jones DM, Chae CU, et al. Effect of body mass index on natriuretic peptide levels in patients with acute congestive heart failure: a ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) substudy. Am Heart J. 2005;149(4):744–750. PMID 15990762
- McCullough PA, Duc P, Omland T, et al. B-type natriuretic peptide and renal function in the diagnosis of heart failure: an analysis from the Breathing Not Properly Multinational Study. Am J Kidney Dis. 2003;41(3):571–579. PMID 12612980
- Anwaruddin S, Lloyd-Jones DM, Baggish A, et al. Renal function, congestive heart failure, and amino-terminal pro-brain natriuretic peptide measurement: results from the PRIDE Study. J Am Coll Cardiol. 2006;47(1):91–97. PMID 16386670
- Logeart D, Thabut G, Jourdain P, et al. Predischarge B-type natriuretic peptide assay for identifying patients at high risk of re-admission after decompensated heart failure. J Am Coll Cardiol. 2004;43(4):635–641. PMID 14975475
- Troughton RW, Frampton CM, Yandle TG, et al. Treatment of heart failure guided by plasma aminoterminal brain natriuretic peptide (N-BNP) concentrations. Lancet. 2000;355(9210):1126–1130. PMID 10791374
- Eurlings LW, van Pol PE, Kok WE, et al. Management of chronic heart failure guided by individual N-terminal pro-B-type natriuretic peptide targets: results of the PRIMA study. J Am Coll Cardiol. 2010;56(25):2090–2100. PMID 21144969
- Persson H, Erntell H, Eriksson B, et al. Improved pharmacological therapy of chronic heart failure in primary care: a randomized Study of NT-proBNP Guided Management of Heart Failure (SIGNAL-HF). Eur J Heart Fail. 2010;12(12):1300–1308. PMID 20876734
- Januzzi JL Jr, Rehman SU, Mohammed AA, et al. Use of amino-terminal pro-B-type natriuretic peptide to guide outpatient therapy of patients with chronic left ventricular systolic dysfunction (PROTECT). J Am Coll Cardiol. 2011;58(18):1881–1889. PMID 22018299
- Felker GM, Anstrom KJ, Adams KF, et al. Effect of natriuretic peptide-guided therapy on hospitalization or cardiovascular mortality in high-risk patients with heart failure and reduced ejection fraction: a randomized clinical trial (GUIDE-IT). JAMA. 2017;318(8):713–720. PMID 28829876
- Vasan RS, Benjamin EJ, Larson MG, et al. Plasma natriuretic peptides for community screening for left ventricular hypertrophy and systolic dysfunction: the Framingham Heart Study. JAMA. 2002;288(10):1252–1259. PMID 12215132
- Ledwidge M, Gallagher J, Conlon C, et al. Natriuretic peptide-based screening and collaborative care for heart failure: the STOP-HF randomized trial. JAMA. 2013;310(1):66–74. PMID 23821090
- Lam CS, Lyass A, Kraigher-Krainer E, et al. Influence of sex and hormone status on circulating natriuretic peptides. J Am Coll Cardiol. 2011;58(6):618–626. PMID 21798425
- McKie PM, Burnett JC Jr. B-type natriuretic peptide as a biomarker beyond heart failure: speculations and opportunities. Mayo Clin Proc. 2005;80(8):1029–1036. PMID 16092582
Live PubMed Searches
The following links run current searches on PubMed and return literature published since this page was written.
- Breathing Not Properly study
- Obesity and BNP suppression
- GUIDE-IT and guided therapy
- ACC/AHA heart failure guidelines
- ESC heart failure guidelines
- NT-proBNP and neprilysin inhibition
- NT-proBNP age-stratified thresholds
- STOP-HF screening trial
- BNP and incident heart failure risk
- BNP thresholds in renal failure
- Natriuretic peptides in HFpEF
- BNP in pulmonary embolism
Connections
- All Lab Tests
- The Heart & Circulation — interactive animation
- Cardiac Troponin (Troponin I & T)
- Kidney Function Tests
- Complete Blood Count
- Comprehensive Metabolic Panel
- Inflammatory Markers
- High-Sensitivity CRP
- Coagulation Panel
- Cortisol Test
- Coronary Calcium Score
- Cardiology Diseases
- Heart Failure
- Atrial Fibrillation
- Cardiomyopathy
- Cardiovascular Disease
- Pulmonary Hypertension
- Pulmonary Embolism
- Kidney Disease
- Hypertension
- Coronary Artery Disease
- Shortness of Breath
- Aortic Stenosis
- Hypothyroidism