Aortic Stenosis
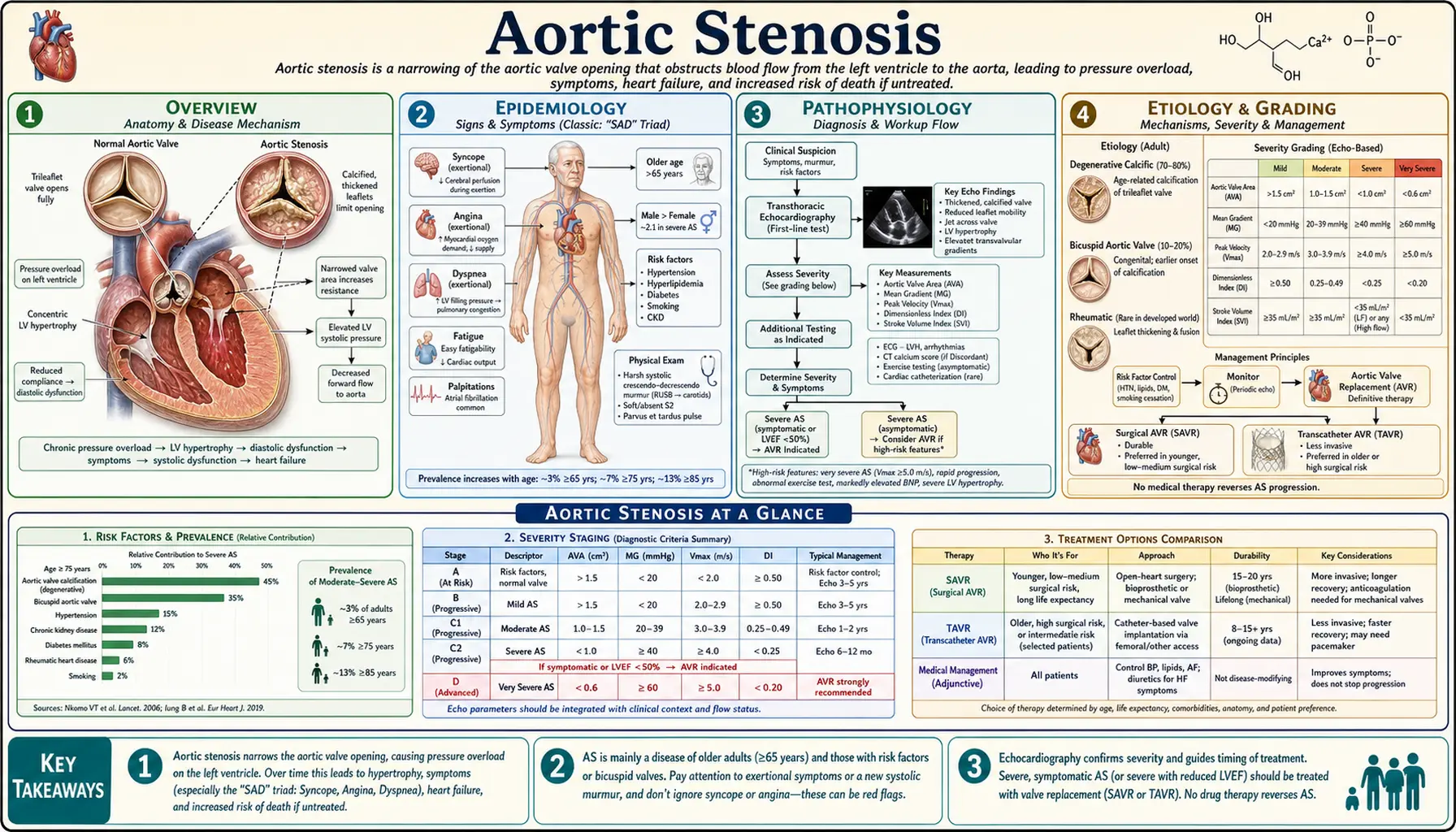
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Grading
- Classic Symptomatic Triad
- Diagnosis
- Medical Management
- TAVR (Transcatheter Aortic Valve Replacement)
- SAVR (Surgical Aortic Valve Replacement)
- Bicuspid Aortic Valve and Aortopathy
- Complications and Prognosis
- Research Papers
- Connections
- Featured Videos
1. Overview
Aortic stenosis (AS) is the most common valvular heart disease in developed countries and the most common valvular cause of cardiac surgery. It involves progressive narrowing of the aortic valve orifice, obstructing left ventricular (LV) outflow. The three primary etiologies are calcific/degenerative disease (adults >65), bicuspid aortic valve (BAV — adults 40–60, affecting 1–2% of the population), and rheumatic disease.
Severe AS is defined by a valve area <1.0 cm², peak jet velocity ≥4 m/s, and mean gradient ≥40 mmHg. Once symptoms appear, clinical deterioration is rapid and survival is markedly reduced without intervention. Transcatheter aortic valve replacement (TAVR) has revolutionized management for patients across all surgical risk strata, transforming AS from a near-universally lethal condition in poor surgical candidates to one with broadly available effective treatment options.
2. Epidemiology
- Prevalence 2–5% in adults >65 years; rises to 8–9% in adults >85 years
- Bicuspid aortic valve (BAV) affects 1–2% of the general population; congenital defect but calcification and severe stenosis develops 20–30 years earlier than in patients with a normal tricuspid valve
- Approximately 100,000 TAVR procedures are performed per year in the United States; TAVR surpassed SAVR in annual volume around 2019
- Rheumatic AS remains prevalent in developing countries and virtually always occurs with mitral valve involvement
- 5-year incidence of aortic valve replacement doubled from 2000–2020, driven by an aging population and expanded TAVR access
- AS is the third most common cardiovascular disease after coronary artery disease and hypertension in the developed world
3. Pathophysiology
Calcific Aortic Stenosis
The pathogenesis of calcific AS shares features with atherosclerosis: endothelial injury leads to lipid infiltration, followed by local inflammation, oxidative stress, and progressive calcium deposition on valve leaflets. Risk factors overlap significantly with those for coronary artery disease — age, male sex, hypertension, hyperlipidemia, diabetes, and smoking all accelerate valve calcification.
Leaflet stiffening and reduced valve opening area create an increasing transvalvular pressure gradient. The LV compensates with concentric hypertrophy (pressure overload pattern): sarcomeres added in parallel increase wall thickness while cavity dimensions remain relatively unchanged, normalizing wall stress per the Laplace law. Over time, this compensatory hypertrophy leads to diastolic dysfunction (a stiff, non-compliant LV), and eventually to systolic dysfunction when afterload exceeds the LV's compensatory capacity — a phenomenon called afterload mismatch.
Concentric hypertrophy also reduces coronary reserve: thickened walls compress intramural coronary vessels, and the hypertrophied myocardial mass demands more oxygen than the coronary circulation can supply during stress. This explains why angina is common in severe AS even in the absence of obstructive coronary artery disease. When ventricular output falls critically, systemic vascular resistance rises and cardiogenic shock can ensue.
Bicuspid Aortic Valve (BAV)
BAV most commonly results from abnormal fusion of the right and left cusps (less often the right and non-coronary cusps). Turbulent, asymmetric transvalvular flow accelerates leaflet degeneration and calcium deposition, typically producing severe AS 10–20 years earlier than in patients with a tricuspid aortic valve (median age 60–65 vs. 75–80 years). BAV is also independently associated with aortopathy — medial degeneration of the aortic wall driven by abnormal NOTCH1 signaling and fibrillin-1 deficiency — not solely by hemodynamic turbulence.
4. Etiology and Grading
Etiology
- Degenerative/calcific (most common, ≥70 years): Progressive calcium deposition on a normal tricuspid valve; risk factors mirror atherosclerosis
- Bicuspid aortic valve (BAV, congenital): Presents as severe AS 10–20 years earlier than calcific AS; associated with aortopathy in up to 50%
- Rheumatic disease (post-streptococcal): Commissural fusion causing stenosis; virtually always combined with aortic regurgitation and mitral valve disease; still prevalent in developing countries
Grading by 2021 AHA/ACC Valvular Heart Disease Guideline
- Mild AS: Peak jet velocity (Vmax) 2.0–2.9 m/s, mean gradient <20 mmHg, aortic valve area (AVA) >1.5 cm²
- Moderate AS: Vmax 3.0–3.9 m/s, mean gradient 20–39 mmHg, AVA 1.0–1.5 cm²
- Severe AS: Vmax ≥4.0 m/s, mean gradient ≥40 mmHg, AVA ≤1.0 cm² (indexed AVA ≤0.6 cm²/m²)
- Very severe AS: Vmax ≥5.0 m/s, mean gradient ≥60 mmHg
- Low-flow low-gradient AS: AVA ≤1.0 cm² but mean gradient <40 mmHg due to depressed EF (classical) or small LV cavity with preserved EF (paradoxical low-flow); dobutamine stress echocardiography distinguishes true-severe AS (gradient rises with increased flow) from pseudo-severe AS (fixed low gradient with depressed contractility)
5. Classic Symptomatic Triad
The landmark natural history data established by Ross and Braunwald in 1968 define expected survival once each symptom of severe AS appears. Before symptoms develop, the prognosis is relatively good. Symptom onset signals LV decompensation and marks a critical inflection in prognosis:
- Angina: Mean survival approximately 5 years after onset. Mechanism: demand ischemia from concentric hypertrophy with reduced coronary flow reserve, independent of epicardial coronary artery disease.
- Syncope (exertional): Mean survival approximately 3 years after onset. Mechanism: fixed cardiac output cannot increase appropriately with exercise-induced peripheral vasodilation → cerebral hypoperfusion. Arrhythmias (AV block, ventricular tachycardia) are an additional cause.
- Dyspnea / Heart failure: Mean survival 1–2 years after onset. The most ominous symptom; reflects LV decompensation with elevated filling pressures and reduced forward output.
Physical Examination Findings
- Murmur: Harsh crescendo-decrescendo systolic ejection murmur, heard best at the right upper sternal border (2nd intercostal space), radiating to the carotids. Murmur intensity does not reliably correlate with severity — a soft or absent murmur in apparent AS may indicate severe stenosis with low cardiac output.
- Soft or absent A2: Calcified, immobile leaflets fail to produce a normal aortic closure sound; paradoxically split S2 can occur from prolonged LV ejection time.
- Pulsus parvus et tardus: Slow-rising, late-peaking, diminished amplitude carotid pulse — a classic bedside sign of severe AS.
- Sustained PMI: Reflects concentric LV hypertrophy and a hyperdynamic apex.
- S4 gallop: Common from the stiff, hypertrophied LV; S3 is less common and suggests advanced LV dysfunction.
6. Diagnosis
Echocardiography (Primary Diagnostic Tool)
Transthoracic echocardiography with Doppler is the standard first-line investigation. Key measurements include:
- Peak jet velocity (Vmax) via continuous-wave Doppler through the aortic valve
- Mean transvalvular gradient (derived from the velocity-time integral)
- Aortic valve area (AVA) calculated by the continuity equation: AVA = LVOT area × LVOT VTI / AV VTI
- LV wall thickness, chamber dimensions, and ejection fraction
- Diastolic function parameters (E/A ratio, E/e' ratio, LA volume index)
- Aortic root and ascending aorta dimensions (essential in BAV for aortopathy screening)
CT Calcium Scoring
Aortic valve calcium (AVC) scoring by CT is important for TAVR planning and for confirming severity in low-gradient AS. An Agatston score >3,000 in men or >1,600 in women strongly supports severe AS regardless of gradient. CT also provides annular sizing critical for TAVR prosthesis selection.
Cardiac Catheterization
Direct measurement of the transvalvular gradient via simultaneous aortic and LV pressure measurement is reserved for cases where echocardiography and CT are discordant, or for pre-SAVR coronary angiography. Coronary CT angiography (CCTA) is increasingly used for pre-TAVR coronary assessment to reduce procedural risk.
Cardiac MRI (CMR)
CMR quantifies LV fibrosis via late gadolinium enhancement — a predictor of post-intervention recovery and long-term outcomes. CMR also provides precise aortic root and ascending aortic dimensions in BAV aortopathy and accurate AVA planimetry when echocardiography is technically limited.
Additional Studies
- Chest X-ray: May show cardiomegaly (late), pulmonary vascular congestion, or a calcified aortic valve on the lateral projection
- ECG: LV hypertrophy voltage criteria, ST-T changes in lateral leads, left bundle branch block in advanced disease
- Exercise stress testing: Can unmask symptoms in apparently asymptomatic severe AS; performed only in selected asymptomatic patients under close supervision — contraindicated in symptomatic severe AS
- Dobutamine stress echo: Used in low-flow low-gradient AS to distinguish true-severe from pseudo-severe; flow augmentation with dobutamine reveals whether the gradient rises appropriately
- BNP/NT-proBNP: Elevated levels correlate with symptom burden and predict outcomes; useful for serial monitoring of asymptomatic severe AS
7. Medical Management
There is currently no proven pharmacologic therapy that slows AS progression or improves outcomes in asymptomatic severe AS. Management is focused on cardiovascular risk factor control, monitoring for symptom onset, and optimal timing of valve intervention.
- Hypertension: Treat aggressively; ACE inhibitors and ARBs are appropriate but should be started at low doses and titrated carefully to avoid precipitous blood pressure drops across a fixed outflow obstruction
- Statins: Observational data suggested statins might slow AS progression (shared mechanism with atherosclerosis), but two randomized controlled trials — SEAS (rosuvastatin) and SALTIRE (atorvastatin) — showed no benefit on AS progression or clinical events. Statins should NOT be initiated specifically to slow AS progression, though they remain indicated for concurrent coronary artery disease.
- Heart failure management: Diuretics for volume overload are appropriate; ACE inhibitors and vasodilators must be used very cautiously in symptomatic severe AS due to the risk of profound hypotension from fixed cardiac output against a reduced afterload
- Atrial fibrillation: Rate and rhythm control are important; loss of atrial contribution to LV filling is poorly tolerated in the stiff, hypertrophied ventricle of severe AS
- Antibiotic endocarditis prophylaxis: Not routinely recommended for native AS; indicated only for patients with prior infective endocarditis or a prosthetic valve
- Activity restriction: Strenuous exercise should be avoided in severe symptomatic AS; asymptomatic severe AS with normal exercise testing may participate in low-to-moderate intensity activity
Echocardiographic Surveillance Intervals
- Mild AS: every 3–5 years
- Moderate AS: every 1–2 years
- Severe asymptomatic AS: every 6–12 months; immediate evaluation if symptoms develop
8. TAVR (Transcatheter Aortic Valve Replacement)
TAVR involves percutaneous delivery and deployment of a bioprosthetic valve within the diseased native aortic valve, eliminating the need for open-heart surgery. The PARTNER (Placement of Aortic Transcatheter Valves) trial series has provided the definitive evidence base across all surgical risk groups:
- PARTNER 1B (2010, PMID 20961243) — Inoperable patients: TAVR reduced 1-year all-cause mortality from 50.7% to 30.7% vs. standard medical therapy (NNT approximately 5). This landmark trial established TAVR as the standard of care for patients with no surgical option.
- PARTNER 1A (2011, PMID 21639811) — High surgical risk: TAVR non-inferior to SAVR for all-cause mortality at 1 year (24.2% vs. 26.8%), with more strokes but fewer major bleeding events with TAVR.
- PARTNER 2A (2016, PMID 26989201) — Intermediate surgical risk: TAVR non-inferior to SAVR at 2 years; transfemoral TAVR was superior to SAVR in subgroup analysis.
- PARTNER 3 (2019, PMID 30882175) — Low surgical risk: TAVR superior to SAVR at 1 year for the composite endpoint of death, stroke, or rehospitalization (8.5% vs. 15.1%, P<0.001). This trial opened TAVR to the full spectrum of surgical risk.
Current Indications (2021 AHA/ACC Guideline)
- TAVR is recommended (Class I) for symptomatic severe AS in patients with high or prohibitive surgical risk
- TAVR is reasonable (Class IIa) for intermediate-risk patients ≥65 years and low-risk patients ≥65 years who prefer TAVR
- SAVR is preferred for low-risk patients <65 years due to durability concerns (prosthetic lifetime considerations and valve-in-valve implications for future reintervention)
- Transfemoral access is strongly preferred over alternative access routes (transapical, transaxillary, transcaval) due to consistently superior outcomes
TAVR Complications
- Stroke: 1–3% peri-procedural; cerebral embolic protection devices are increasingly used but evidence for routine use remains mixed
- Paravalvular leak (PVL): Even mild PVL increases late mortality; a major driver of the learning curve and prosthesis iteration. Moderate or severe PVL is an indication for reintervention.
- Permanent pacemaker implantation: 15–25% with self-expanding valves (Evolut platform); 3–8% with balloon-expandable valves (SAPIEN platform); driven by conduction injury from oversizing or deep implantation
- Vascular access complications: Hematoma, pseudoaneurysm, arteriovenous fistula at the femoral access site; rates declining with smaller delivery systems and ultrasound guidance
- Coronary obstruction: Rare (<1%) but life-threatening; valve leaflets displaced toward coronary ostia during deployment; pre-procedural CT planning identifies at-risk anatomy. "Coronary protection" with guidewires is performed prophylactically in high-risk cases.
- Valve thrombosis: Subclinical leaflet thrombosis detected on CT in 10–15%; clinical valve thrombosis is rare (<1%); responds to anticoagulation
TAVR Durability
Long-term structural valve deterioration (SVD) data are accumulating. Five-year outcomes from PARTNER trials show low rates of clinically significant SVD. Landmark 10-year TAVR durability data — including the FRANCE TAVI and CoreValve/Evolut registries — demonstrate generally favorable durability for patients with intermediate or high surgical risk. For younger patients requiring longer valve lifetimes, valve durability remains an area of active investigation.
9. SAVR (Surgical Aortic Valve Replacement)
Surgical aortic valve replacement via median sternotomy and cardiopulmonary bypass remains the gold standard for:
- Low surgical risk patients <65 years (mechanical valve option avoids structural deterioration; lifetime anticoagulation accepted)
- Bicuspid aortic valve AS with concurrent aortopathy requiring root or ascending aortic repair (Bentall or David procedure)
- Multi-valve disease requiring combined procedures (e.g., AS with mitral valve disease)
- Patients with anatomic contraindications to TAVR (small annulus, unfavorable LVOT geometry, severe aortic regurgitation without calcification)
- Patients requiring concurrent procedures (coronary artery bypass grafting, septal myectomy for HCM)
- Failed TAVR requiring open reintervention
Prosthesis Choice
- Bioprosthetic (tissue) valves: No long-term anticoagulation required; structural deterioration at 15–20 years (accelerated in younger, more active patients); "valve-in-valve" TAVR can treat future degeneration percutaneously, avoiding redo sternotomy
- Mechanical valves: Lifelong warfarin anticoagulation (INR 2.0–3.0 for aortic position); no structural deterioration; preferred in young patients who can reliably anticoagulate
- Valve-in-valve TAVR: TAVR deployed within a failed bioprosthetic SAVR ring is increasingly used to avoid high-risk redo sternotomy; annular sizing constraints and higher gradients than native-valve TAVR are important limitations
10. Bicuspid Aortic Valve and Aortopathy
BAV is the most common congenital cardiac malformation, present in 1–2% of the population. Its clinical importance extends beyond valve disease to thoracic aortic aneurysm and dissection risk. Aortopathy affects up to 50% of BAV patients and is driven by intrinsic aortic wall weakness from NOTCH1 pathway mutations and abnormal smooth muscle cell function — independent of hemodynamic turbulence from the valve itself.
Aortopathy Screening and Management
- TTE at diagnosis to measure aortic root, sinotubular junction, and ascending aorta
- Annual imaging if the ascending aorta is >4.0 cm; CT angiography or CMR for precise measurement
- Surgical repair threshold: 5.5 cm (or 5.0 cm if growth rate >0.5 cm/year, family history of dissection, or valve surgery is being performed for another indication)
- Beta-blockers reduce the rate of aortic dilation; losartan is used in Marfan-related aortopathy but data in isolated BAV are less robust
Genetics and Family Screening
BAV is heritable with an autosomal dominant pattern with variable penetrance; 5–10% of first-degree relatives have BAV. Echocardiographic screening of all first-degree relatives is recommended at diagnosis. Genetic testing for NOTCH1, GATA5, and ROBO4 mutations is emerging but not yet standard of care outside research settings. TAVR in BAV-AS is technically more challenging (asymmetric annulus, leaflet morphology) and historically excluded from major trials, though contemporary data and dedicated BAV TAVR techniques show increasingly favorable results.
11. Complications and Prognosis
Natural History Without Intervention
Untreated symptomatic severe AS carries an extremely poor prognosis: approximately 50% 2-year mortality and 75% 5-year mortality from symptom onset. Sudden cardiac death accounts for approximately 15% of AS-related deaths and can occur even in previously asymptomatic patients, particularly those with very severe gradients or rapid hemodynamic progression.
Post-Intervention Prognosis
With successful TAVR or SAVR, survival approaches age-matched population norms in intermediate- and high-risk patients. In PARTNER 3 (low-risk patients), 5-year outcomes confirm durable survival benefit for both TAVR and SAVR over prior medical therapy benchmarks. The primary determinants of long-term post-intervention prognosis include pre-existing LV dysfunction, degree of LV reverse remodeling (regression of hypertrophy and recovery of EF), and comorbidities (AF, chronic kidney disease, frailty).
Major Complications
- Heart failure: Most common cause of death in unrepaired AS; late post-TAVR HF driven by residual LV dysfunction, paravalvular leak, or structural valve deterioration
- Atrial fibrillation: Affects 30–40% of patients with severe AS; LA hypertension from impaired LV filling drives atrial remodeling; worsened by the loss of atrial kick in a stiff ventricle
- Infective endocarditis: Risk on native calcified valve (low) and prosthetic valve (1–3%/year); prophylaxis recommended for prosthetic valves per guidelines
- Paravalvular regurgitation (TAVR > SAVR): Even mild paravalvular leak after TAVR is associated with reduced long-term survival; newer-generation devices have significantly reduced this complication
- Structural valve deterioration (SVD): Long-term concern for bioprosthetic valves in SAVR and TAVR; time to SVD is accelerated in younger, more metabolically active patients
- Stroke and systemic embolism: Valve calcification, AF, and prosthetic valve thrombosis all contribute to embolic risk
- Anticoagulation-related hemorrhage: Relevant for patients on warfarin for mechanical valves or AF
- Conduction disease: High-degree AV block requiring permanent pacemaker after TAVR (especially with oversized self-expanding valves or deep implant depth)
Research Papers
The following PubMed topic searches return current peer-reviewed literature relevant to aortic stenosis. Each link opens a live PubMed query.
- Aortic stenosis treatment
- TAVR PARTNER trial
- Transcatheter aortic valve replacement outcomes
- Aortic stenosis natural history
- Calcific aortic valve disease
- Bicuspid aortic valve
- TAVR vs SAVR low risk
- Aortic valve replacement complications
- Aortic stenosis echocardiography
- Aortic stenosis guidelines
- Aortic stenosis pathophysiology
- TAVR long-term durability
Connections
- Cardiology
- Valvular Heart Disease
- Hypertrophic Cardiomyopathy
- Heart Failure
- Cardiomyopathy
- Atrial Fibrillation
- Coronary Artery Disease
- Endocarditis
- Arrhythmia
- Hypertension
- Chest Pain
- Shortness of Breath
- Fatigue
- Magnesium
- Omega-3 Fatty Acids