Milk Thistle for Antioxidant and Glutathione Support
Most herbal "antioxidants" provide modest direct free-radical scavenging and stop there. Silymarin is unusual because it operates through three distinct antioxidant mechanisms that together produce an effect far larger than direct scavenging chemistry can explain. First, silymarin replenishes glutathione (GSH) — the body's principal water-soluble intracellular antioxidant — by 35-50% in hepatic and intestinal tissue. Second, it activates the Nrf2 / antioxidant response element (ARE) master regulatory pathway, upregulating dozens of phase II detoxification and cytoprotective genes simultaneously. Third, it scavenges reactive oxygen species directly through its flavonolignan chemistry. The combined effect produces a clinically distinguishable hepatic-antioxidant footprint, and the GSH-replenishment mechanism in particular makes silymarin a useful complement to N-acetylcysteine (NAC), alpha-lipoic acid, and selenium in liver-support protocols. This page details each mechanism, the comparison with NAC, the documented synergies, and the clinical settings where silymarin's antioxidant profile produces the most benefit.
Table of Contents
- The Three Antioxidant Mechanisms
- Glutathione (GSH) Replenishment in the Liver
- Extrahepatic Glutathione Effects (Intestinal, Renal)
- Nrf2 / Antioxidant Response Element (ARE) Pathway
- Phase II Detoxification Enzymes Upregulated
- Direct Free-Radical Scavenging Chemistry
- Silymarin vs N-Acetylcysteine (NAC) Comparison
- Alpha-Lipoic Acid Synergy
- Selenium and Vitamin E Synergy
- Clinical Applications — Oxidative Stress Conditions
- Dosing and Cautions
- Key Research Papers
- Connections
- Featured Videos
The Three Antioxidant Mechanisms
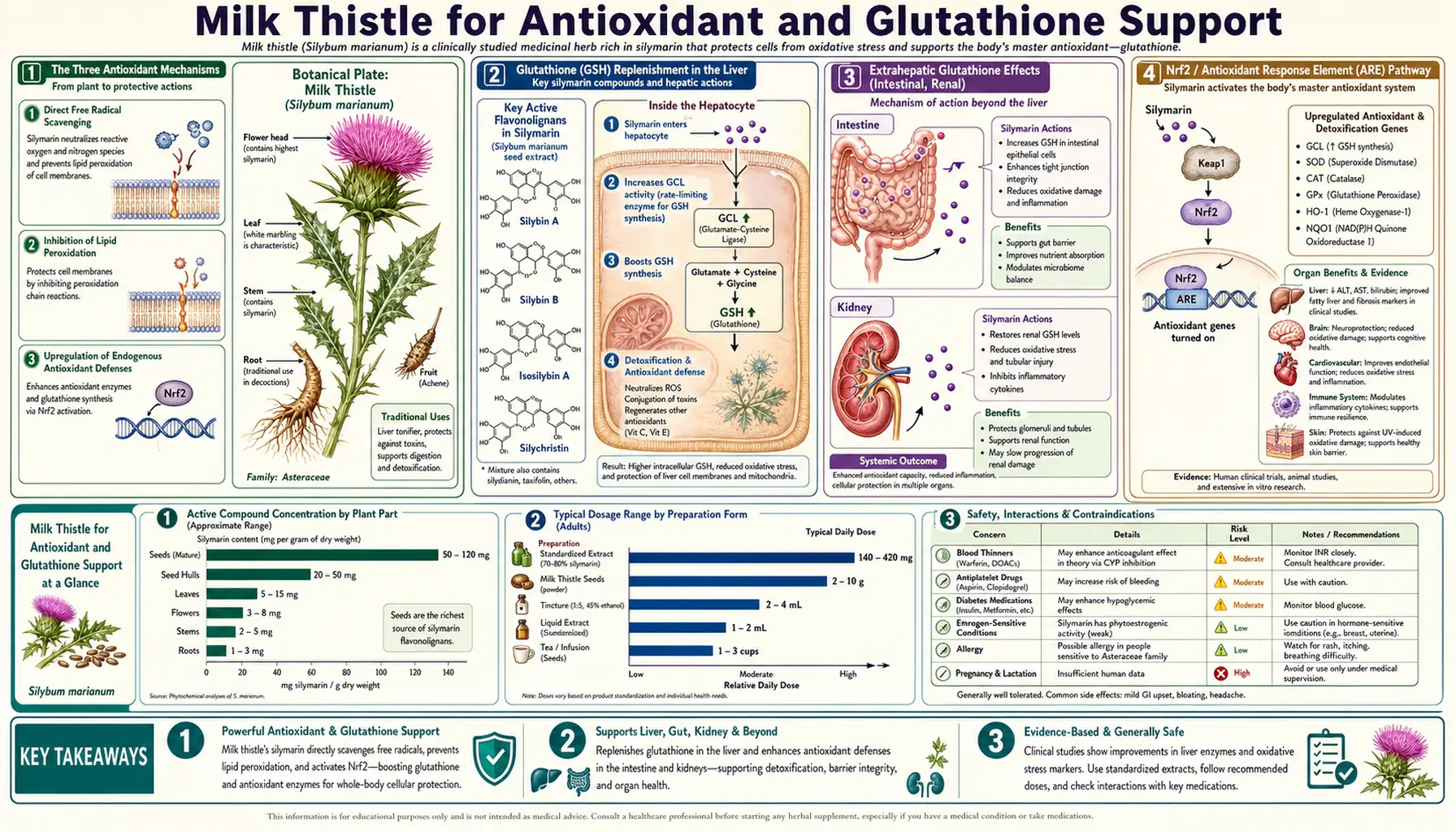
The antioxidant effect of silymarin is the most well-characterized of its biological activities and explains a substantial fraction of its clinical hepatoprotective benefit. Three distinct mechanisms operate in parallel:
- Glutathione replenishment — silymarin increases hepatic and intestinal glutathione (GSH) concentrations by 35-50% in deficient animals and patients, restoring the cell's principal endogenous water-soluble antioxidant. The mechanism is upregulation of glutamate-cysteine ligase (the rate-limiting enzyme in GSH synthesis) plus reduced GSH consumption from less oxidative stress.
- Nrf2 / ARE pathway activation — silymarin disrupts the Keap1-Nrf2 cytoplasmic complex, freeing Nrf2 to translocate to the nucleus and activate transcription of hundreds of cytoprotective genes through ARE binding sites in their promoters. This is the master regulatory mechanism that ties together many of the discrete antioxidant effects.
- Direct scavenging — silymarin flavonolignans donate hydrogen atoms or electrons to reactive oxygen species (ROS), neutralizing them. The chemistry is conventional flavonoid antioxidant chemistry — the same kind that explains the antioxidant activity of green tea catechins, quercetin, and resveratrol — but is the smallest of the three contributions to overall effect.
The clinical consequence of this multi-mechanism architecture is that silymarin produces a larger antioxidant footprint than its direct scavenging activity alone would predict. Conversely, in vitro radical-trapping assays (DPPH, ORAC, etc.) systematically underestimate silymarin's clinical antioxidant effect, because they capture only mechanism 3 and miss mechanisms 1 and 2.
Glutathione (GSH) Replenishment in the Liver
Glutathione is a tripeptide (glutamate-cysteine-glycine) that serves as the cell's principal intracellular water-soluble antioxidant and is also the universal cofactor for the phase II glutathione S-transferase (GST) conjugation reactions that detoxify xenobiotic compounds before urinary excretion. Hepatic GSH concentrations are normally 5-10 mM — among the highest of any cell type in the body — reflecting the liver's role as the principal site of phase II xenobiotic detoxification.
In conditions of acute or chronic hepatic insult (alcohol exposure, acetaminophen overdose, toxic mushroom poisoning, viral hepatitis, NAFLD), hepatic GSH is rapidly depleted — sometimes to 20-40% of normal within hours. GSH depletion is a key step in the cascade leading to hepatocellular necrosis: without GSH, the reactive metabolite N-acetyl-p-benzoquinoneimine (NAPQI) from acetaminophen overdose cannot be conjugated and instead covalently binds cellular proteins, killing the cell.
Silymarin restores hepatic GSH through two distinct mechanisms. First, it upregulates glutamate-cysteine ligase (GCLC), the rate-limiting enzyme in GSH biosynthesis from glutamate, cysteine, and glycine. This is the slow, sustained mechanism that produces durable GSH elevation with chronic dosing. Second, it reduces GSH consumption by lowering oxidative stress upstream of GSH demand — if the cell faces fewer ROS to neutralize, less GSH is consumed per unit time.
The combined effect is documented in animal studies and human trials: hepatic GSH increases approximately 35-50% with 2-4 weeks of silymarin 420 mg/day in CCl4-injured rats and in alcoholic liver disease patients. The magnitude is comparable to that achieved with high-dose oral NAC (the standard pharmaceutical GSH-precursor strategy) but with a different mechanism — NAC delivers cysteine (the rate-limiting amino acid in GSH synthesis), while silymarin upregulates the enzyme that uses cysteine.
See our Glutathione page for the broader role of GSH in detoxification, immunity, and antioxidant defense.
Extrahepatic Glutathione Effects (Intestinal, Renal)
While the liver is the dominant site of silymarin's GSH effect, two extrahepatic effects are clinically important.
Intestinal GSH: Because oral silymarin has poor systemic absorption (20-50%) but is fully exposed to the intestinal epithelium during transit, intestinal cells receive higher silymarin concentrations than hepatocytes. Silymarin elevates intestinal GSH in animal studies of intestinal injury (chemotherapy-induced enteritis, radiation enteritis, NSAID-induced enteropathy). This extrahepatic effect is being investigated as a possible adjunct to chemotherapy regimens to reduce mucositis — preliminary trials in pediatric oncology patients receiving cisplatin show reduced GI toxicity scores.
Renal GSH: Kidney tubule cells are second only to hepatocytes in baseline GSH concentration and in vulnerability to oxidant-driven injury (radiocontrast nephropathy, aminoglycoside nephrotoxicity, cisplatin nephrotoxicity). Silymarin reaches the kidney via the systemic circulation and may produce modest renal GSH elevation. Pilot trials in radiocontrast prophylaxis (where NAC has been the conventional intervention with mixed results) have included silymarin arms with suggestive but inconclusive benefit.
The skeptic's position: most of the strong GSH-elevation data is from hepatic tissue in animals at doses substantially above standard human dosing. Extrapolation to clinical effect on extrahepatic tissues at typical oral doses requires caution.
Nrf2 / Antioxidant Response Element (ARE) Pathway
Nrf2 (nuclear factor erythroid 2-related factor 2) is the master transcription factor regulating cellular antioxidant and cytoprotective gene expression. The Nrf2 pathway is now recognized as one of the central regulatory mechanisms of cellular antioxidant defense and has been the target of intensive drug discovery for the past two decades.
In the resting state, Nrf2 is sequestered in the cytoplasm bound to its inhibitor Keap1 (Kelch-like ECH-associated protein 1), which targets Nrf2 for proteasomal degradation. Oxidative stress, electrophilic stress, or specific phytochemical activators (sulforaphane from broccoli, curcumin from turmeric, silymarin from milk thistle) modify reactive cysteine residues on Keap1, disrupting the Keap1-Nrf2 complex. Freed Nrf2 then translocates to the nucleus, heterodimerizes with small Maf proteins, and binds antioxidant response elements (AREs) in the promoter regions of cytoprotective genes.
The downstream effect is broad. Several dozen genes are activated, including:
- NQO1 (NAD(P)H quinone oxidoreductase 1) — reduces quinones to less-reactive hydroquinones
- HO-1 (heme oxygenase 1) — degrades heme, producing the antioxidant bilirubin
- GCLC and GCLM (glutamate-cysteine ligase catalytic and modifier subunits) — rate-limiting enzymes in GSH biosynthesis
- GST (glutathione S-transferases) — phase II conjugation
- SOD1 (superoxide dismutase 1) — superoxide neutralization
- UGT (UDP-glucuronosyltransferases) — phase II glucuronidation
- SLC7A11 (cystine-glutamate antiporter) — cysteine uptake supporting GSH synthesis
Silymarin is a well-documented Nrf2 activator at concentrations achievable with oral dosing. The downstream upregulation of NQO1, HO-1, GCLC, and GST has been confirmed in hepatocyte cell lines, animal models, and human peripheral blood mononuclear cell ex vivo studies. This is the mechanism that ties together silymarin's GSH-elevation effect, its phase-II detoxification enhancement, and much of its broader cytoprotection.
The Nrf2 mechanism is shared with curcumin, sulforaphane, and (to a lesser extent) green tea catechins, which is the rationale for combining these phytochemicals in liver-support and antioxidant protocols. Empirical evidence for additive or synergistic effect from combinations is preliminary but consistent.
Phase II Detoxification Enzymes Upregulated
"Phase II" detoxification refers to the conjugation reactions in the liver that take phase-I-oxidized intermediates and attach water-soluble groups (glutathione, glucuronic acid, sulfate, glycine, taurine, acetyl, methyl), rendering the compound water-soluble enough for urinary or biliary excretion. The phase II reactions are catalyzed by several distinct enzyme families, most of which are Nrf2-regulated and upregulated by silymarin.
The clinically most important phase II reactions and their silymarin response:
- Glutathione S-transferase (GST) conjugation — GST conjugates glutathione to electrophilic phase-I intermediates. Several GST isoforms (alpha, mu, pi, theta) are upregulated by Nrf2 activation. Silymarin produces modest GST induction in human and animal studies.
- UDP-glucuronosyltransferase (UGT) glucuronidation — UGT attaches glucuronic acid to hydroxyl, carboxyl, and amine groups. UGT1A1 (handling bilirubin), UGT1A6 (handling acetaminophen), and UGT2B7 (handling morphine, NSAIDs) are all upregulated by Nrf2. Silymarin shows modest UGT induction.
- Sulfotransferase (SULT) sulfation — SULT attaches sulfate. The Nrf2 effect on sulfation is smaller than on glutathione conjugation and glucuronidation.
- NAD(P)H quinone oxidoreductase 1 (NQO1) — reduces toxic quinones to less-reactive hydroquinones. Strongly Nrf2-regulated and strongly silymarin-inducible.
The clinical translation: in patients with high xenobiotic burden (medication-heavy elderly, environmental-toxin-exposed workers, smokers, alcohol drinkers), enhanced phase II capacity should improve detoxification of xenobiotics, drugs, and endogenous oxidized metabolites. This is part of the rationale for milk thistle in general "liver support" protocols.
Direct Free-Radical Scavenging Chemistry
The third antioxidant mechanism — direct free-radical scavenging — is the most chemically straightforward but produces the smallest contribution to overall clinical effect. Silymarin flavonolignans have multiple hydroxyl groups (on the chroman and phenolic rings of silybin) that can donate hydrogen atoms to neutralize ROS.
In standard in vitro radical-trapping assays:
- DPPH (1,1-diphenyl-2-picrylhydrazyl) radical scavenging — silybin shows IC50 approximately 8-15 µM, comparable to quercetin and somewhat less potent than vitamin E or epigallocatechin gallate (EGCG)
- ABTS (azinobis-3-ethylbenzothiazoline) radical scavenging — similar potency profile
- Hydroxyl radical scavenging — silybin is moderately effective
- Singlet oxygen quenching — modest activity
- Lipid peroxidation chain termination — effective at micromolar concentrations
The clinical limitation of direct-scavenging chemistry is that the achievable serum concentrations of silybin are typically in the low micromolar range (1-5 µM peak with standard oral dosing, somewhat higher with Siliphos), which is below the IC50 for many of the direct scavenging assays. The clinical antioxidant effect is therefore not primarily driven by direct scavenging but by GSH elevation and Nrf2 induction, which produce sustained protective gene expression at lower silymarin concentrations.
The exception is the gastrointestinal lumen, where silymarin concentrations during absorption are much higher than circulating levels. Direct scavenging in the gut lumen may contribute to the intestinal-mucosal protective effect documented in chemotherapy-mucositis and NSAID-enteropathy models.
Silymarin vs N-Acetylcysteine (NAC) Comparison
N-Acetylcysteine (NAC) is the conventional pharmaceutical agent for raising hepatic glutathione — it is the FDA-approved antidote for acetaminophen overdose and is widely used as a mucolytic and as a general glutathione precursor in integrative medicine. Comparing silymarin to NAC is the most useful framework for understanding when to use each (and when to use both).
| Property | NAC | Silymarin |
|---|---|---|
| Mechanism | Cysteine precursor (rate-limiting amino acid for GSH synthesis) | Upregulates GCLC enzyme; Nrf2 activation |
| Onset of GSH elevation | Hours (rapid) | Days to weeks (slower) |
| Magnitude of GSH elevation | Large with IV or high-dose oral | 35-50% with sustained oral |
| Oral bioavailability | Modest (4-10%) | Modest (20-50%) |
| Acetaminophen antidote | FDA-approved, definitive (within 8-10 hours) | Not standard; supportive |
| Amanita antidote | Adjunctive; lower-tier | IV Legalon SIL: standard of care in Europe |
| Chronic liver support | Standard 600-1,200 mg/day | Standard 420 mg/day |
| Cost | Inexpensive | Inexpensive to moderate |
| Tolerability | Sulfur odor; some GI upset | Generally excellent |
| Pulmonary use | Mucolytic (nebulized or oral) | No respiratory indication |
The pragmatic conclusion: for acute hepatic insult (acetaminophen overdose, the first 6-12 hours of amanita exposure), NAC is faster-acting and has more robust acute-care evidence. For chronic liver-support and oxidative-stress management (chronic alcohol exposure, NAFLD, environmental toxin exposure, recovery from past hepatic injury), silymarin offers the better mechanistic profile because it upregulates GSH-synthesizing capacity rather than merely providing precursor.
The two can be used together — the mechanisms are complementary, not redundant — and integrative liver-support protocols commonly combine NAC 600 mg twice daily with silymarin 420 mg/day. There is no documented antagonism, and the cysteine-precursor + enzyme-induction combination provides both rapid and sustained GSH elevation. See our NAC page for the broader NAC story.
Alpha-Lipoic Acid Synergy
Alpha-lipoic acid (ALA) is a sulfur-containing fatty acid that is both water- and lipid-soluble, allowing it to function as an antioxidant in both aqueous and membrane compartments. Its principal antioxidant role is recycling oxidized vitamin C and vitamin E back to their reduced active forms, indirectly extending the antioxidant lifetime of those vitamins. ALA also chelates transition metals, enhances insulin sensitivity, and supports mitochondrial bioenergetics.
The ALA-silymarin combination has been studied most extensively in mushroom poisoning and in chronic hepatitis C. The classic American protocol for Amanita phalloides poisoning developed by Dr. Todd Mitchell at Dominican Hospital in Santa Cruz, California (the largest U.S. center for amanita treatment) combines IV silibinin (Legalon SIL) with high-dose alpha-lipoic acid, NAC, penicillin G (which competes with amanitin for OATP1B3 transport), and supportive care. Mortality with this combined protocol has dropped to under 10% in published Mitchell series.
Outside acute toxicity, the ALA + silymarin combination is used in chronic liver disease management. The mechanism rationale is multi-layered: ALA recycles vitamin C and E, ALA chelates iron in iron-overloaded livers (relevant in hemochromatosis and chronic HCV-associated iron accumulation), silymarin elevates GSH and activates Nrf2, and the two together produce broader oxidative-stress coverage than either alone.
Typical dosing in chronic liver support protocols: silymarin 420 mg/day plus alpha-lipoic acid 300-600 mg/day in divided doses.
See our Antioxidants section for the broader antioxidant landscape and how individual agents complement each other.
Selenium and Vitamin E Synergy
Selenium is the central atom in selenoenzymes including glutathione peroxidase (GPx), the enzyme that uses GSH to reduce hydrogen peroxide to water. Without adequate selenium, GPx activity drops and oxidative stress increases regardless of GSH availability. Selenium deficiency is common in regions with selenium-poor soils (much of Europe, parts of China, parts of New Zealand).
The clinical logic for combining selenium with silymarin: silymarin elevates GSH, and selenium ensures that the GSH is being efficiently utilized by glutathione peroxidase. Selenium supplementation alone in low-selenium populations has been associated with reduced liver cancer incidence in observational studies. The combination is part of many integrative chronic-HCV and chronic-HBV protocols, typically at selenium 100-200 µg/day (selenomethionine or yeast-bound forms).
Vitamin E (alpha-tocopherol) is the principal lipid-phase antioxidant, terminating lipid peroxidation chain reactions in cell membranes. Vitamin E is consumed (oxidized to the alpha-tocopheroxyl radical) when it performs this function and must be recycled back to its reduced form, traditionally via vitamin C and ALA. In NAFLD/NASH, vitamin E 800 IU/day has demonstrated histologic improvement (PIVENS trial 2010) and is one of the few interventions with FDA-recognized NASH benefit. Combining vitamin E with silymarin in NASH is mechanistically sensible (membrane-phase antioxidant + GSH/Nrf2 enhancement) and is a common integrative protocol.
Typical NASH protocol combination: silymarin 420 mg/day + vitamin E 400-800 IU/day + selenium 100-200 µg/day.
Clinical Applications — Oxidative Stress Conditions
Beyond classic liver disease, silymarin's antioxidant profile makes it useful in several broader conditions characterized by significant oxidative stress:
- Type 2 diabetes — chronic hyperglycemia drives mitochondrial ROS production and AGE formation. Silymarin trials in T2D (e.g., Huseini 2006) show modest reductions in fasting glucose and HbA1c, plus improvements in lipid panel and oxidative stress markers (MDA, GSH). The effect is small and would not replace metformin, but silymarin is a reasonable adjunct, particularly in T2D patients with concurrent NAFLD.
- Beta-thalassemia and iron overload — iron-overloaded patients have severe chronic oxidative stress as iron catalyzes Fenton-reaction generation of hydroxyl radicals. Silymarin trials in transfusion-dependent thalassemia (Gharagozloo 2009, Hagag 2013) show reduced serum ferritin, reduced lipid peroxidation markers, and improved hepatic function. Combined with iron chelation therapy (deferoxamine or deferasirox), silymarin is part of an integrated approach.
- Drug-induced hepatotoxicity prophylaxis — pretreatment with silymarin before known hepatotoxic drug courses (anti-tuberculosis regimens with isoniazid + rifampin + pyrazinamide, chemotherapy with methotrexate or cisplatin, statins) is supported by animal data and small pilot trials. Standard dose 420 mg/day starting 1-2 weeks before exposure.
- Environmental toxin exposure — chronic occupational or environmental exposure to solvents, pesticides, heavy metals, or mycotoxins increases oxidative stress and depletes GSH. Silymarin is widely used in occupational-medicine integrative protocols for this population.
- Recovery from prolonged alcohol consumption — once a patient has achieved alcohol abstinence, silymarin during the first 6-12 months of recovery may accelerate hepatic regeneration and reduce residual oxidative stress markers.
- Mold/mycotoxin illness (CIRS, ochratoxin, aflatoxin exposure) — the Toxins section covers mycotoxin chemistry; silymarin is one of several agents used in detoxification-phase protocols. See Mold and Mycotoxins for the broader picture.
Dosing and Cautions
Standard antioxidant/GSH-support dose: 420 mg/day standardized silymarin in three divided doses (140 mg three times daily) is the canonical European hepatology dose and the dose most studied in the GSH-elevation literature.
Combined GSH-support protocols:
• Silymarin 420 mg/day + NAC 600 mg twice daily (basic protocol)
• Silymarin 420 mg/day + NAC 600 mg twice daily + ALA 300-600 mg/day (intermediate)
• Silymarin 420 mg/day + NAC 600 mg twice daily + ALA 300-600 mg/day + Selenium 200 µg/day + Vitamin E 400 IU/day (full NASH or chronic-hepatitis adjunct)
Take with a meal containing fat to improve oral absorption. Avoid taking with high-fiber meals.
Duration: 3-12 months for most clinical applications. Indefinite long-term use is generally regarded as safe but should be periodically reassessed.
Cautions specific to the antioxidant role:
• Pro-oxidant paradox at very high doses — like many flavonoids, silymarin can switch from antioxidant to pro-oxidant behavior at supraphysiologic concentrations in vitro. The clinical relevance at oral doses is uncertain, but doses above 2,100 mg/day of standard silymarin have no documented additional benefit and should not be used routinely.
• Chemotherapy interaction caution — some chemotherapy agents work by inducing oxidative stress in tumor cells (doxorubicin, cisplatin, bleomycin). Concurrent high-dose antioxidant supplementation theoretically could reduce chemotherapy efficacy. The clinical data are mixed; oncology guidance is divided. Conservative practice is to avoid high-dose antioxidants during active chemotherapy administration days, with silymarin permitted on off-days or for hepatoprotection between cycles.
• Iron interaction — silymarin chelates iron and may reduce dietary iron absorption. In iron-deficient patients (menstruating women, vegetarians, post-bariatric), separate by 2-4 hours from iron-rich meals or iron supplements.
• Pregnancy/lactation — safety data limited; conservative practice avoids new initiation.
Key Research Papers
- Valenzuela A, Aspillaga M, Vial S, Guerra R (1989). Selectivity of silymarin on the increase of the glutathione content in different tissues of the rat. Planta Med 55(5):420-2. — PubMed
- Kim SH et al. (2012). Silibinin prevents TPA-induced MMP-9 expression and VEGF secretion by inactivation of the Raf/MEK/ERK pathway. Mol Carcinog. — PubMed
- Kim BR et al. (2012). Silibinin protects against carbon tetrachloride-induced acute hepatotoxicity via Nrf2 activation. Toxicology. — PubMed
- Mereish KA, Bunner DL, Ragland DR, Creasia DA (1991). Protection against microcystin-LR-induced hepatotoxicity by silymarin: biochemistry, histopathology, and lethality. Pharm Res 8(2):273-7. — PubMed
- Surai PF (2015). Silymarin as a Natural Antioxidant: An Overview of the Current Evidence and Perspectives. Antioxidants (Basel) 4(1):204-47. — PubMed
- Huseini HF et al. (2006). The efficacy of Silybum marianum (L.) Gaertn. (silymarin) in the treatment of type II diabetes: a randomized, double-blind, placebo-controlled, clinical trial. Phytother Res 20(12):1036-9. — PubMed
- Gharagozloo M et al. (2009). The effect of an Iranian herbal drug on minor beta-thalassemia: a randomized double-blind placebo-controlled clinical trial. Phytomedicine. — PubMed
- Bektur NE et al. (2016). Protective effects of silymarin against acetaminophen-induced hepatotoxicity and nephrotoxicity in mice. Toxicol Mech Methods. — PubMed
- Kren V, Walterova D (2005). Silybin and silymarin — new effects and applications. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 149(1):29-41. — PubMed
- Comelli MC et al. (2007). Toward the definition of the mechanism of action of silymarin: activities related to cellular protection from toxic damage. Integr Cancer Ther 6(2):120-9. — PubMed
- Lieber CS et al. (2003). Silymarin retards the progression of alcohol-induced hepatic fibrosis in baboons. J Clin Gastroenterol. — PubMed
- Polyak SJ, Ferenci P, Pawlotsky JM (2013). Hepatoprotective and antiviral functions of silymarin components in hepatitis C virus infection. Hepatology. — PubMed
PubMed Topic Searches
- PubMed: Silymarin glutathione (GSH)
- PubMed: Silymarin Nrf2/ARE pathway
- PubMed: Silymarin + NAC combination
- PubMed: Silymarin + alpha-lipoic acid
- PubMed: Silymarin phase II detoxification
- PubMed: Silymarin oxidative stress / lipid peroxidation
Connections
- Milk Thistle Overview
- Milk Thistle Benefits Hub
- Liver Protection & Detox
- Hepatitis Adjunctive
- Skin Health
- N-Acetylcysteine (NAC)
- Glutathione
- Oxidative Stress
- Liver Cleansing
- Detox Protocols
- Turmeric (Curcumin)
- Dandelion
- Liver Disease
- NAFLD/NASH
- Type 2 Diabetes
- Hemochromatosis
- Mold & Mycotoxins
- Vitamin C
- Selenium
- Comprehensive Metabolic Panel
- All Herbs