Milk Thistle — Benefits Deep Dive
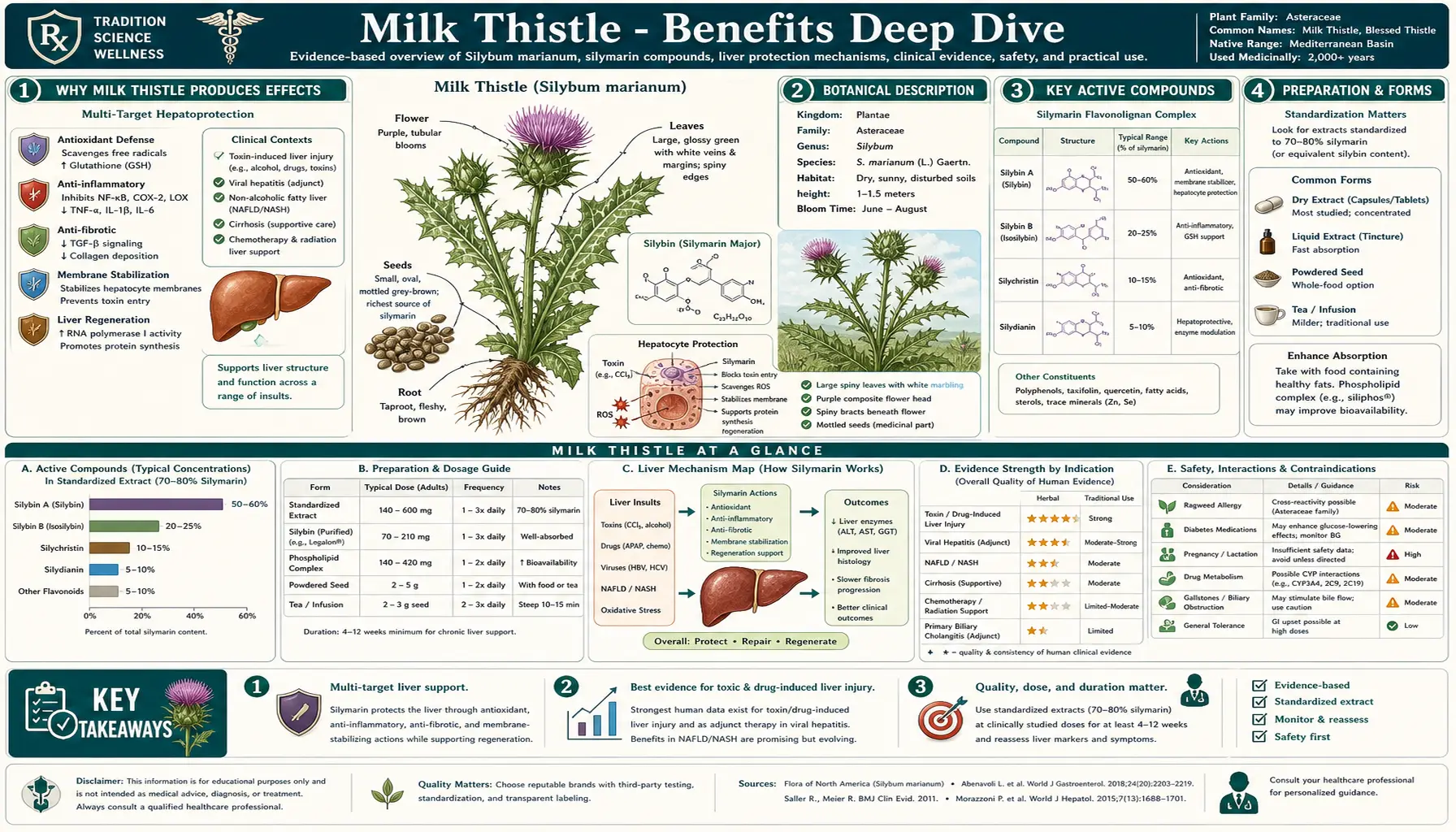
Milk Thistle (Silybum marianum) is the single most-studied herbal liver protectant in modern phytomedicine, with a documented therapeutic record stretching back more than 2,000 years to Dioscorides and Pliny the Elder. The active constituent is silymarin, a flavonolignan complex extracted from the seed (technically the achene), composed principally of silybin A and silybin B (collectively "silibinin") along with isosilybin, silychristin, and silydianin. Silybin alone accounts for 60-70% of standardized silymarin and is the principal active compound. The most dramatic clinical demonstration of milk thistle's liver-protective effect is the use of intravenous silibinin (Legalon SIL) as the standard-of-care antidote for Amanita phalloides (death cap mushroom) poisoning across Europe — a setting in which placebo-controlled trials are impossible but observational evidence shows mortality dropping from ~25% to under 10%. Four benefit pages below explore the conditions where milk thistle produces the largest clinical effect — alcoholic and toxic liver disease, oxidative stress and glutathione replenishment, chronic viral hepatitis (HBV and HCV) adjunctive therapy, and topical and oral dermatologic applications.
Deep-Dive Articles
Liver Protection & Detox
The silymarin flavonolignan complex (silybin A/B, isosilybin, silychristin, silydianin), the German Commission E and EMA HMPC monographs, Cochrane meta-analyses of alcoholic liver disease and cirrhosis trials, the Amanita phalloides mushroom poisoning antidote story (intravenous Legalon SIL silibinin), the hepatocyte membrane-stabilization and hepatic-regeneration mechanism (RNA polymerase I stimulation), and the canonical 420 mg/day standardized silymarin dosing protocol.
Antioxidant & Glutathione
Silymarin's replenishment of hepatic and intestinal glutathione (GSH) by 35-50%, Nrf2/ARE pathway activation upregulating phase II detoxification enzymes (NQO1, HO-1, GST, glutamate-cysteine ligase), direct free-radical scavenging chemistry, side-by-side comparison with N-acetylcysteine (NAC) as a GSH-precursor alternative, and the documented synergy with alpha-lipoic acid (ALA) and selenium in liver-support protocols.
Hepatitis Adjunctive
The mixed-evidence picture for chronic hepatitis C (HCV) — positive serum-aminotransferase signals in older trials, the disappointing HALT-C and Fried/SyNCH IV silibinin trials, and the modern reframing of milk thistle as an HCV symptom-and-quality-of-life adjunct now that direct-acting antivirals cure most HCV. Hepatitis B (HBV) trials showing modest aminotransferase reduction and HBV DNA effects. The Siliphos / IdB 1016 phosphatidylcholine complex that solves milk thistle's notoriously poor oral bioavailability.
Skin Health
Topical silymarin as a UVB-photoprotective agent (preventing sunburn cell formation, pyrimidine dimer reduction, and apoptosis in keratinocytes), randomized trials in melasma and chloasma showing pigmentation reduction comparable to hydroquinone with a vastly better safety profile, post-inflammatory hyperpigmentation use, rosacea anti-inflammatory effects, and the dual antioxidant + NF-kappa-B-inhibition + matrix metalloproteinase suppression mechanism behind topical formulations.
Table of Contents
- Deep-Dive Articles
- Why Milk Thistle Produces Effects
- Key Research Papers
- External Authoritative Resources
- Connections
- Featured Videos
Why Milk Thistle Produces Effects
Most herbal products have either a single dominant mechanism or such poorly characterized chemistry that the mechanism remains speculative. Milk thistle is unusual in having both well-characterized active constituents (the silymarin flavonolignan complex, with silybin A and B identified and synthesized) and multiple complementary mechanisms that converge on the same target organ — the hepatocyte. Five mechanisms together explain the breadth of clinical effect:
- Hepatocyte membrane stabilization — silybin physically intercalates into the phospholipid bilayer of the hepatocyte plasma membrane, altering membrane fluidity in a way that blocks toxin entry. This is the demonstrated mechanism behind the Amanita phalloides antidote use: alpha-amanitin and phalloidin (the two principal death-cap toxins) enter hepatocytes via the OATP1B3 sodium-independent organic-anion transporter, and silybin competes for that same transporter, preventing toxin uptake. This same membrane-protective effect underlies milk thistle's protection against carbon tetrachloride, acetaminophen, halothane, and ethanol in animal models.
- Hepatic protein synthesis and regeneration (RNA polymerase I stimulation) — silybin stimulates nucleolar RNA polymerase I, increasing ribosomal RNA transcription, ribosome assembly, and protein synthesis in hepatocytes. The cells most damaged by toxin or alcohol exposure are also the cells most actively regenerating, and silymarin accelerates that regenerative protein synthesis. This is the rare mechanism that drives active healing, not just damage prevention.
- Glutathione (GSH) replenishment — silymarin raises hepatic and intestinal glutathione concentrations by 35-50% in deficient animals and patients, restoring the body's principal water-soluble intracellular antioxidant. Because GSH is required for phase II conjugation of both endogenous oxidized molecules and exogenous toxins, this single mechanism produces broad downstream protection. See the Antioxidant & Glutathione page for the full mechanism.
- Nrf2 / antioxidant response element (ARE) pathway activation — silymarin disrupts the Keap1-Nrf2 complex, freeing Nrf2 to translocate to the nucleus and bind ARE elements in the promoter regions of phase II detoxification genes. The downstream effects include induction of NAD(P)H quinone oxidoreductase 1 (NQO1), heme oxygenase-1 (HO-1), glutathione S-transferase (GST), glutamate-cysteine ligase (the rate-limiting enzyme in GSH synthesis), and several other cytoprotective enzymes. This is now recognized as one of the master regulatory mechanisms of cellular antioxidant defense.
- Antifibrotic (hepatic stellate cell inhibition) — silymarin suppresses transforming growth factor-beta (TGF-β) signaling in hepatic stellate cells, the cell type responsible for laying down collagen during cirrhosis. By blocking stellate cell activation from quiescent vitamin-A-storing cells to activated myofibroblast-like cells, silymarin reduces collagen deposition and slows the progression of fibrosis. This is the proposed mechanism behind the modest cirrhosis-survival benefit seen in some (but not all) older European trials.
The therapeutic complication that limits all of these mechanisms is poor oral bioavailability. Free silybin has an oral bioavailability of approximately 20-50%, with extensive first-pass conjugation to glucuronide and sulfate forms in the liver, and relatively short serum half-life (~6 hours). Two pharmaceutical solutions address this: (1) Siliphos / IdB 1016, a silybin-phosphatidylcholine complex that increases bioavailability roughly 4.6-fold via improved lipid-membrane partitioning, and (2) Legalon, the standardized 80%-silymarin extract used in the European hepatology literature and the intravenous formulation (Legalon SIL) used in the mushroom-poisoning antidote protocol. Generic supermarket milk thistle capsules vary wildly in silymarin content and are not pharmaceutically equivalent to the studied preparations.
Key Research Papers
- Saller R, Meier R, Brignoli R (2001). The use of silymarin in the treatment of liver diseases. Drugs 61(14):2035-63. — PubMed
- Rambaldi A, Jacobs BP, Gluud C (2007). Milk thistle for alcoholic and/or hepatitis B or C virus liver diseases. Cochrane Database Syst Rev. — PubMed
- Mengs U, Pohl RT, Mitchell T (2012). Legalon SIL: the antidote of choice in patients with acute hepatotoxicity from amatoxin poisoning. Curr Pharm Biotechnol 13(10):1964-70. — PubMed
- Fried MW et al. (2012). Effect of silymarin (milk thistle) on liver disease in patients with chronic hepatitis C unsuccessfully treated with interferon (SyNCH trial). JAMA 308(3):274-82. — PubMed
- Loguercio C, Festi D (2011). Silybin and the liver: from basic research to clinical practice. World J Gastroenterol 17(18):2288-301. — PubMed
External Authoritative Resources
- NCCIH (NIH National Center for Complementary and Integrative Health) — Milk Thistle — U.S. government summary of evidence base, safety, drug interactions
- EMA (European Medicines Agency) HMPC monograph — Silybi mariani extractum siccum raffinatum et normatum — the formal European pharmacopoeial monograph for standardized milk thistle extract
- WHO Monographs on Selected Medicinal Plants Volume 2 — Fructus Silybi Mariae — the WHO traditional-medicine reference monograph
- MedlinePlus — Milk Thistle — NLM consumer drug-information sheet
- Memorial Sloan Kettering — Milk Thistle About Herbs — oncology-focused review of drug-herb interactions
- PubMed — All silymarin / silybin / silibinin / milk thistle research (~5,000+ papers)
Connections
- Milk Thistle (Main Page)
- Liver Protection & Detox
- Antioxidant & Glutathione
- Hepatitis Adjunctive
- Skin Health
- All Herbs
- Turmeric (Curcumin)
- Dandelion
- Chanca Piedra
- Andrographis
- N-Acetylcysteine (NAC)
- Glutathione
- Liver Disease
- Cirrhosis
- Non-Alcoholic Fatty Liver Disease
- Hepatitis
- Hepatitis C
- Liver Cleansing
- Detox Protocols
- Oxidative Stress
- Comprehensive Metabolic Panel
- GGT (Liver Enzyme)