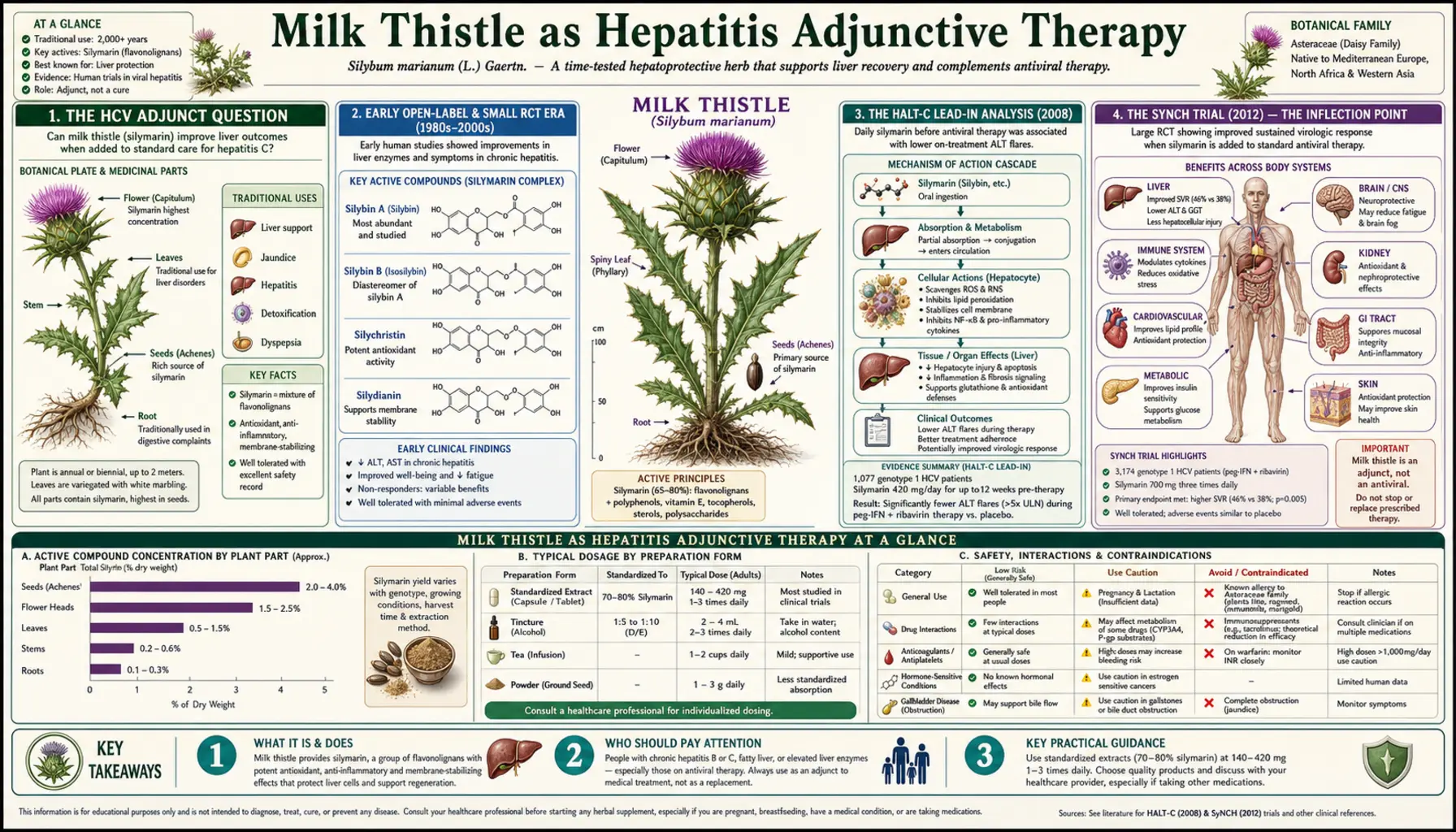
Milk Thistle as Hepatitis Adjunctive Therapy
The story of milk thistle in chronic viral hepatitis is the most instructive case study in herbal medicine of how the evidence-base evolves as trial quality improves. From the 1980s through the early 2000s, milk thistle was widely promoted (especially in the United States) as a "treatment" for chronic hepatitis C based on small open-label trials showing reduced serum aminotransferases. The 2012 SyNCH trial — a properly powered NIH-sponsored randomized placebo-controlled study of high-dose silymarin in interferon-failed HCV patients — produced unambiguously negative results: no benefit on HCV RNA, no benefit on serum ALT, no benefit on liver histology. At roughly the same time, the arrival of direct-acting antivirals (sofosbuvir, ledipasvir, glecaprevir, and successors) made HCV definitively curable in over 95% of treated patients within 8-12 weeks. Milk thistle's role in HCV has therefore been definitively recast: not a treatment of the virus, but a reasonable adjunct for symptomatic relief, fatigue, quality of life, and ongoing hepatic-cell-membrane stabilization during and after antiviral therapy. The HBV evidence is similar but smaller. This page walks through the trial history, the 2012 SyNCH inflection point, the modern HBV/HCV adjunct framework, and the Siliphos / IdB 1016 phosphatidylcholine bioavailability-enhanced formulation that is the modern preferred preparation.
Table of Contents
- The HCV Adjunct Question
- Early Open-Label and Small RCT Era (1980s-2000s)
- The HALT-C Lead-In Analysis (2008)
- The SyNCH Trial (2012) — The Inflection Point
- The Direct-Acting Antiviral (DAA) Era and the Modern Reframing
- Intravenous Silibinin in HCV Salvage Therapy
- Hepatitis B (HBV) Evidence Base
- Siliphos / IdB 1016 — The Bioavailability Solution
- Legalon and Standardization Issues
- Modern Dosing Protocols
- Symptom and Quality-of-Life Effects
- Cautions and Antiviral Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
The HCV Adjunct Question
Hepatitis C virus (HCV) infection chronically affects an estimated 50-70 million people worldwide, including approximately 2.4 million in the United States as of the most recent CDC estimates. Untreated chronic HCV leads to cirrhosis in 15-30% of patients over 20-30 years, with subsequent risk of hepatocellular carcinoma. The disease was, for decades, the principal indication for liver transplantation in developed countries.
The therapeutic landscape transformed completely between 2013 and 2018 with the introduction of direct-acting antivirals (DAAs) — combination regimens of sofosbuvir, ledipasvir, velpatasvir, glecaprevir, pibrentasvir, and others — that achieve sustained virologic response (cure) in over 95% of treated patients with 8-12 week oral courses. HCV is now considered curable for essentially anyone with access to treatment.
The question this page addresses is therefore not "does milk thistle treat HCV" — we know the answer is no — but the more nuanced question: "what role, if any, does milk thistle play as an adjunct in HCV patients?" The patient populations of interest are: (1) HCV patients before they start DAA therapy (often a wait of weeks to months for prior-authorization or insurance approval), (2) HCV patients during DAA therapy (potential symptomatic and hepatocellular support), (3) HCV patients after DAA cure who have residual hepatic damage (cirrhosis, fibrosis, persistent ALT elevation), and (4) HCV patients who cannot access or cannot tolerate DAAs.
The honest answer for all four populations is that silymarin is a reasonable adjunct based on its general hepatoprotective profile, but it does not affect the virus or change the trajectory of viral disease. The relevant outcomes are symptomatic and biochemical (ALT/AST reduction, fatigue, quality of life), not virologic.
Early Open-Label and Small RCT Era (1980s-2000s)
The early enthusiasm for milk thistle in chronic hepatitis came from a series of small, mostly open-label, mostly European studies in the 1980s and 1990s. Representative results:
- Buzzelli et al. (1993) — 20 patients with chronic active hepatitis received Siliphos (silybin-phosphatidylcholine) 240 mg twice daily for 7 days. Serum ALT and AST decreased significantly. Open-label, no control group.
- Marcelli et al. (1992) — 60 patients with chronic active hepatitis (mixed alcoholic and viral) randomized to Siliphos 120 mg three times daily versus placebo for 60 days. Significant reductions in serum aminotransferases in the silymarin arm.
- Mayer KE et al. (2005) — systematic review of 14 trials in chronic liver disease; concluded that milk thistle preparations produced modest reductions in serum transaminases (typically 20-30%) but had insufficient evidence for clinical endpoints (survival, complications).
These early results drove widespread off-label use of milk thistle for chronic hepatitis throughout the 1990s and 2000s, particularly in the United States where conventional HCV therapy (interferon alpha plus ribavirin) had cure rates of only 30-50% with significant toxicity. Many HCV patients turned to integrative medicine, and milk thistle was the most-recommended herbal supplement in that setting.
The pattern of evidence — small trials, soft endpoints (transaminases rather than viral load or fibrosis), open-label or inadequate blinding — was a classic setup for the larger, more rigorous trials of the late 2000s to deliver disappointing results.
The HALT-C Lead-In Analysis (2008)
The HALT-C (Hepatitis C Antiviral Long-Term Treatment Against Cirrhosis) trial was a large NIH-sponsored multicenter trial of long-term low-dose interferon for prevention of cirrhosis progression in HCV. As a substudy, the investigators (Seeff et al., Gastroenterology 2008) analyzed milk thistle use among the 1,145 enrolled HCV patients.
Findings:
- 17% of HCV patients reported milk thistle use at baseline (consistent with widespread off-label use in this population)
- Milk thistle users had lower serum ALT and AST than non-users (the predicted effect from the open-label literature)
- Milk thistle users did not have lower HCV viral load, lower liver fibrosis scores, or different rates of cirrhosis progression
- The investigators concluded that observed transaminase reduction in milk thistle users did not translate to improved clinical outcomes
This was the first hint, on a large dataset, that the transaminase-reduction effect seen in earlier trials was not delivering downstream clinical benefit. The HALT-C analysis was observational rather than randomized, but the size and quality of the dataset (1,145 patients with detailed clinical follow-up) made it influential. The investigators called for a definitive randomized trial — which became SyNCH.
The SyNCH Trial (2012) — The Inflection Point
The SyNCH trial (Silymarin in NASH and C Hepatitis) was the long-awaited NIH-funded, NCCAM-sponsored, definitive randomized placebo-controlled trial of silymarin in chronic HCV. Design: 154 patients with chronic HCV who had failed prior interferon-based therapy, randomized to one of three arms for 24 weeks:
- Placebo (50 patients)
- Silymarin 420 mg three times daily (52 patients)
- Silymarin 700 mg three times daily (52 patients) — high-dose arm
The silymarin preparation was a standardized 89.4%-silymarin Madaus / Mylan product, the same Legalon-equivalent extract used in the European cirrhosis trials. The 700 mg three-times-daily arm (2,100 mg/day) was the highest dose ever formally tested in HCV.
Primary endpoint: at least 50% reduction in serum ALT, or reduction to within normal range, at week 24.
Results, published in JAMA (Fried MW et al., 2012):
- Primary endpoint met by 2/50 (4%) placebo, 1/52 (2%) low-dose silymarin, and 2/52 (4%) high-dose silymarin — no statistically significant difference
- HCV RNA: no change in any arm
- Mean serum ALT: no significant change in either silymarin arm versus placebo
- Quality of life scores (SF-36, CLDQ): no significant difference
- Safety: silymarin was well-tolerated at both doses
The conclusion: "Higher than customary doses of silymarin did not significantly reduce serum ALT levels more than placebo in participants with chronic HCV infection unsuccessfully treated with interferon-based therapy."
This was the inflection point in the milk thistle / HCV story. SyNCH was adequately powered, properly blinded, used a high-quality standardized preparation, and tested doses up to three times the standard dose. The trial did not find an effect because there was no effect to find at any dose tested.
The published response from the integrative medicine community focused on (1) the patient selection (interferon-failed patients with advanced disease) being unfavorable for any intervention, (2) the oral bioavailability limitation of standard silymarin (Siliphos was not used), and (3) the choice of ALT reduction as the primary endpoint when fibrosis or HCV RNA might have been more relevant. These critiques have merit, but they do not rescue the underlying claim that silymarin treats HCV.
The Direct-Acting Antiviral (DAA) Era and the Modern Reframing
The publication of SyNCH coincided with the emergence of direct-acting antiviral (DAA) therapy for HCV. Telaprevir and boceprevir were approved in 2011 as first-generation DAAs added to interferon-based regimens; sofosbuvir (the first nucleotide polymerase inhibitor) was approved in late 2013 as the foundation of interferon-free regimens. By 2016, multiple all-oral 8-12 week DAA combinations were curing >95% of HCV patients across all genotypes.
This made the SyNCH negative result moot in a practical sense. HCV is now a curable disease for any patient with access to DAA therapy. The question "what should HCV patients take instead of DAAs" no longer needs an answer for most patients.
Milk thistle's role in HCV has therefore been reframed in three pragmatic ways:
- Pre-DAA hepatocellular support — for patients awaiting insurance approval, or with persistently elevated ALT and significant symptoms while awaiting treatment, silymarin at standard doses may provide modest symptomatic and biochemical improvement during the wait. It does not affect the virus and should not delay DAA initiation.
- Concurrent with DAA therapy — some patients add milk thistle during their 8-12 week DAA course as general hepatoprotection. There is no evidence this helps DAA cure rates (which are already >95%), but it does not interfere. Drug-interaction concerns are minimal at standard milk thistle doses (CYP3A4 inhibition is theoretical but clinically small).
- Post-DAA cure with residual cirrhosis — patients cured of HCV but left with cirrhosis remain at risk for hepatocellular carcinoma and decompensation. Silymarin as long-term hepatoprotection in this population is reasonable, though no specific trials exist. Standard 420 mg/day, indefinite duration, periodic ALT and Child-Pugh assessment.
For the population without access to DAAs (uninsured patients in some U.S. settings, low-income countries with limited DAA access), milk thistle remains a reasonable symptomatic adjunct, but the priority should be establishing DAA access through patient-assistance programs, generic availability, or international procurement.
See our Hepatitis C page and Hepatitis overview page for the broader HCV clinical picture.
Intravenous Silibinin in HCV Salvage Therapy
A footnote to the HCV / silymarin story: between 2008 and the DAA breakthrough, a small body of European literature explored intravenous silibinin (Legalon SIL) as salvage therapy for HCV patients with previous interferon failure, particularly in the post-transplant setting where HCV recurrence is universal and rapid.
Ferenci and colleagues (Vienna 2008, Gastroenterology) reported that high-dose IV silibinin (15-20 mg/kg/day for 14 days) produced dose-dependent reductions in HCV RNA, sometimes by 3-4 log₁₀ — a much larger effect than ever observed with oral silymarin. The mechanism was hypothesized to involve direct inhibition of HCV RNA-dependent RNA polymerase (NS5B) at the high tissue concentrations achievable with IV but not oral dosing.
Subsequent post-transplant studies (Beinhardt et al.) used IV silibinin successfully in patients with severe HCV recurrence who had failed interferon-based regimens. The effect was real but transient — HCV RNA rebounded after IV silibinin discontinuation.
This entire IV-silibinin-for-HCV literature was rendered obsolete by DAAs. Sofosbuvir achieved 4+ log reductions in HCV RNA at oral doses with vastly better tolerability than IV silibinin infusions. IV Legalon SIL is no longer used for HCV in current practice but remains the standard antidote for amanita poisoning. The clinical-pharmacology data, however, established that silibinin at high tissue concentrations does have direct antiviral activity — just not at concentrations achievable by oral dosing.
Hepatitis B (HBV) Evidence Base
The hepatitis B (HBV) literature on milk thistle is smaller than the HCV literature and considerably more heterogeneous. HBV is a different therapeutic challenge from HCV because (1) most HBV is suppressible but not curable with current antivirals (entecavir, tenofovir), (2) the principal goals of therapy are HBV DNA suppression and prevention of disease progression rather than cure, and (3) HBsAg (surface antigen) clearance is the elusive functional-cure endpoint that current therapies rarely achieve.
Representative HBV trials:
- Kalantari et al. (2011) — 60 chronic HBV patients randomized to silymarin or placebo for 6 months. Silymarin produced modest ALT reduction; no effect on HBV DNA or HBsAg.
- Wei et al. (2008) — meta-analysis of 9 Chinese-language HBV silymarin trials totaling approximately 1,000 patients. Reported modest improvements in liver function tests but methodological quality of included trials was generally poor.
- Rambaldi Cochrane Review (2007) — the same Cochrane review covering alcoholic liver disease also covered HBV. Conclusion: insufficient evidence for clinical benefit in HBV.
The honest summary: HBV evidence for milk thistle is weaker than the HCV evidence base and similarly does not support use as a primary or curative treatment. Adjunctive use during nucleoside analog therapy (entecavir, tenofovir) is reasonable but does not change disease trajectory.
Siliphos / IdB 1016 — The Bioavailability Solution
The persistent question raised by negative oral silymarin trials is whether higher tissue concentrations of silybin would have produced different results. Free silybin has 20-50% oral bioavailability with extensive first-pass conjugation in the liver to glucuronide and sulfate forms (which retain some but not all of the parent compound's activity). The serum half-life is approximately 6 hours.
Siliphos (formerly IdB 1016, developed by Indena S.p.A. of Italy) is a silybin-phosphatidylcholine 1:2 molar complex. The phosphatidylcholine component dramatically improves the lipid-membrane partitioning of silybin during intestinal absorption, with the result that Siliphos delivers approximately 4.6-fold higher silybin plasma concentrations than equimolar standard silymarin. The complex also extends serum half-life modestly.
Siliphos pharmacokinetics:
- 120 mg Siliphos (containing approximately 80 mg silybin) produces peak silybin plasma concentrations equivalent to approximately 540 mg of standard silymarin
- The improvement is most pronounced for free (non-conjugated) silybin in serum
- Hepatic tissue concentrations follow plasma levels, providing 3-5× higher liver silybin exposure
Clinical evidence for Siliphos benefit beyond standard silymarin is mixed. The 2017 Kheong NASH trial (described on the Liver Protection page) used high-dose IdB 1016 (700 mg three times daily) and produced numerical but not statistically significant fibrosis improvement. Several small open-label HCV pilots have suggested better transaminase responses with Siliphos than with equivalent oral silymarin.
The pragmatic position: for patients who can afford it (Siliphos is roughly 3-5× the cost of standard silymarin), it is the rational choice based on pharmacokinetics. For most patients, standard high-quality silymarin (Legalon-equivalent, 80%-standardized) at higher doses (e.g., 700 mg twice daily instead of 140 mg three times daily) achieves similar tissue exposure at lower cost.
Legalon and Standardization Issues
Legalon is the brand name of the original Madaus (now Mylan / Viatris) milk thistle standardized extract, the preparation against which essentially all rigorous clinical trials have been conducted. Standardization specifications:
- Extracted from Silybum marianum seed (achene)
- Standardized to 70-80% silymarin content, with silymarin defined chromatographically as the sum of silybin A, silybin B, isosilybin A, isosilybin B, silychristin, and silydianin
- Silybin content is the specific marker compound, with defined minimums for both silybin A and silybin B
- Manufactured to European Pharmacopoeia specifications
The clinical importance of standardization: generic supermarket milk thistle products may contain anywhere from 30% to 80% silymarin, may not specify silybin content separately, may have wide batch-to-batch variation, and frequently do not meet the European Pharmacopoeia monograph. A 175 mg "milk thistle" capsule from a generic brand may contain anywhere from 50 mg to 140 mg of actual silymarin — a nearly threefold range, with proportionally large variation in silybin content.
For clinical applications where milk thistle is being used as a defined therapeutic intervention (chronic hepatitis adjunct, NAFLD, post-acute liver injury recovery), a standardized 80%-silymarin preparation that meets European Pharmacopoeia specifications — Legalon, Siliphos, or equivalent pharmaceutical-grade products — is the appropriate choice. For general "liver support" without specific therapeutic claims, lower-cost standardized products are acceptable, but unstandardized capsules should be avoided.
Modern Dosing Protocols
Pre-DAA hepatocellular support (HCV awaiting treatment):
Standard silymarin 420 mg/day in three divided doses, or Siliphos 240-360 mg/day. Duration: until DAA therapy starts. Goal: modest symptom and ALT improvement, no expectation of viral effect.
Concurrent with DAA therapy:
Optional addition of standard silymarin 280-420 mg/day. No documented benefit on cure rates, no documented harm. Discontinue if any unexpected liver test changes during DAA course.
Post-DAA cure with residual cirrhosis or persistent ALT elevation:
Standard silymarin 420 mg/day or Siliphos 240-360 mg/day, indefinite duration. Periodic monitoring of ALT, AST, and synthetic function (albumin, INR, bilirubin). Combine with lifestyle modification (alcohol abstinence, NAFLD management if metabolic syndrome present).
Chronic HBV (during nucleoside analog therapy):
Standard silymarin 420 mg/day as adjunct. Does not replace entecavir or tenofovir.
For maximum effect (NASH or severe chronic disease):
Siliphos 240 mg three times daily (720 mg/day total), or equivalent high-dose standard silymarin 700 mg twice daily. May be combined with NAC 600 mg twice daily, alpha-lipoic acid 300-600 mg/day, selenium 200 µg/day, and vitamin E 400-800 IU/day for a full integrated hepatoprotective protocol.
Administration tips:
• Take with a meal containing some fat to improve absorption
• Avoid taking with high-fiber meals
• Space doses through the day (every 6-8 hours) given the ~6-hour serum half-life
• Bedtime dose may be preferred for one of the three daily doses
Symptom and Quality-of-Life Effects
The endpoints where milk thistle does show consistent (if modest) benefit in chronic hepatitis are not the virologic or histologic endpoints but the symptomatic ones. Chronic HCV and HBV patients commonly experience fatigue, right-upper-quadrant discomfort, low-grade nausea, brain fog, and depressive symptoms — collectively sometimes called "HCV-associated extrahepatic syndrome." Several observational studies and pilot trials report improvement in these symptoms with milk thistle.
The Hepatitis Quality of Life Questionnaire (HQLQ), CLDQ (Chronic Liver Disease Questionnaire), and SF-36 have all been used to assess this dimension. Results are mixed but tend to favor silymarin for fatigue and general well-being scores at modest magnitudes (typically 3-8 points on 0-100 scales). The 2012 SyNCH trial did not find significant quality-of-life differences, but the trial population was interferon-failed (already a population with longstanding symptomatic disease) and the 24-week duration may have been too short for subtle quality-of-life changes.
For HCV patients who report fatigue and general hepatic discomfort, a 3-month trial of standard silymarin 420 mg/day is reasonable. If patient-reported outcomes improve, continue; if not, discontinue without prejudice.
Cautions and Antiviral Drug Interactions
- DAA drug interactions — the modern HCV antivirals (sofosbuvir, ledipasvir, velpatasvir, glecaprevir, pibrentasvir) are partly metabolized by CYP3A4 and partly substrates of P-glycoprotein. Silymarin is a weak CYP3A4 inhibitor and modest P-gp inhibitor in vitro. Clinically significant interactions at standard milk thistle doses have not been reported, but caution is reasonable. Patients on DAAs should inform their hepatologist if adding milk thistle, particularly high-dose Siliphos.
- HBV nucleoside analogs — entecavir and tenofovir are not significantly metabolized by CYP450 and do not have clinically relevant interactions with silymarin.
- Interferon (no longer commonly used) — no documented interaction with silymarin.
- Concomitant chronic medications — many HCV patients are on stable doses of other CYP3A4 substrates (statins, calcium channel blockers, immunosuppressants in transplant recipients). Conservative practice consults the prescriber before adding milk thistle in transplant recipients on cyclosporine or tacrolimus.
- HCC surveillance — milk thistle does not substitute for hepatocellular carcinoma (HCC) surveillance in cirrhotic patients. Six-monthly ultrasound + AFP screening remains standard regardless of supplement use.
- Asteraceae allergy — same as for any milk thistle indication.
- Don't use as substitute for vaccination — for HBV-naive patients, HBV vaccination (a two- or three-dose series of recombinant HBsAg vaccine) is the appropriate prevention. Milk thistle has no preventive role.
- Don't replace DAA therapy — patients eligible for DAA cure should be treated, not deferred for trials of herbal therapy. The 8-12 week DAA course delivers definitive cure at low cost (generic sofosbuvir/ledipasvir is now available globally) and minimal toxicity.
Key Research Papers
- Fried MW et al. (2012). Effect of silymarin (milk thistle) on liver disease in patients with chronic hepatitis C unsuccessfully treated with interferon (SyNCH trial). JAMA 308(3):274-82. — PubMed
- Seeff LB et al. (2008). Herbal product use by persons enrolled in the hepatitis C Antiviral Long-Term Treatment Against Cirrhosis (HALT-C) Trial. Hepatology 47(2):605-12. — PubMed
- Ferenci P et al. (2008). Silibinin is a potent antiviral agent in patients with chronic hepatitis C not responding to pegylated interferon/ribavirin therapy. Gastroenterology 135(5):1561-7. — PubMed
- Polyak SJ, Ferenci P, Pawlotsky JM (2013). Hepatoprotective and antiviral functions of silymarin components in hepatitis C virus infection. Hepatology 57(3):1262-71. — PubMed
- Rambaldi A, Jacobs BP, Gluud C (2007). Milk thistle for alcoholic and/or hepatitis B or C virus liver diseases. Cochrane Database Syst Rev 2007(4):CD003620. — PubMed
- Buzzelli G et al. (1993). A pilot study on the liver protective effect of silybin-phosphatidylcholine complex (IdB1016) in chronic active hepatitis. Int J Clin Pharmacol Ther Toxicol 31(9):456-60. — PubMed
- Beinhardt S et al. (2014). Silibinin monotherapy prevents graft infection after orthotopic liver transplantation in patients with chronic hepatitis C. J Hepatol 54(3):591-9. — PubMed
- Wei F, Liu SK, Liu XY, Li ZJ, Li B, Zhou YL (2008). Meta-analysis: silymarin and its combination therapy for the treatment of chronic hepatitis B. Eur J Clin Microbiol Infect Dis. — PubMed
- Kalantari H et al. (2011). The effect of milk thistle (Silybum marianum) on the chronic hepatitis B virus infection. Med J Islam Repub Iran. — PubMed
- Loguercio C et al. (2007). The effect of a silybin-vitamin E-phospholipid complex on nonalcoholic fatty liver disease: a pilot study. Dig Dis Sci. — PubMed
- Marcelli R, Bizzoni P, Conte D, Lisena MO, Lampertico M (1992). Randomized controlled study of the efficacy and tolerability of a short course of IdB 1016 in the treatment of chronic persistent hepatitis. Eur Bull Drug Res. — PubMed
- Wagoner J et al. (2010). Multiple effects of silymarin on the hepatitis C virus lifecycle. Hepatology. — PubMed
PubMed Topic Searches
- PubMed: Silymarin chronic HCV
- PubMed: Silymarin chronic HBV
- PubMed: IV silibinin HCV
- PubMed: Siliphos IdB 1016 bioavailability
- PubMed: Silymarin DAA interactions
- PubMed: Silymarin post-liver-transplant
Connections
- Milk Thistle Overview
- Milk Thistle Benefits Hub
- Liver Protection & Detox
- Antioxidant & Glutathione
- Skin Health
- Hepatitis (Overview)
- Hepatitis C
- Liver Disease
- Cirrhosis
- NAFLD/NASH
- Hepatocellular Carcinoma
- Andrographis
- Chanca Piedra: Liver Protection and Hepatitis B — HBV-specific antiviral mechanism, niranthin vs nucleoside analogs, trial evidence on HBsAg/HBV-DNA, and adjunctive use with entecavir/tenofovir.
- Turmeric
- Dandelion
- N-Acetylcysteine (NAC)
- Glutathione
- Liver Cleansing
- Detox Protocols
- Comprehensive Metabolic Panel
- GGT (Liver Enzyme)
- All Herbs