Milk Thistle for Liver Protection and Detox
Milk thistle's reputation as the premier herbal liver protectant rests on three pillars of evidence: a 2,000-year traditional-use record stretching back to Dioscorides (1st century CE) and Pliny the Elder; modern regulatory recognition by the German Commission E (1986), the European Medicines Agency HMPC monograph (2018), and the WHO traditional-medicine monograph; and a uniquely dramatic clinical application as the standard-of-care intravenous antidote for Amanita phalloides (death cap mushroom) poisoning across Europe (Legalon SIL), where observational data show mortality dropping from ~25% to under 10% in treated patients. The active extract, silymarin, is a flavonolignan complex composed principally of silybin A and silybin B (collectively called "silibinin") together with isosilybin, silychristin, and silydianin — with silybin alone accounting for 60-70% of standardized silymarin and serving as the principal active compound. This page walks through the historical record, the regulatory monographs, the Cochrane meta-analyses of alcoholic liver disease and cirrhosis, the mushroom-poisoning antidote story, and the hepatocyte membrane-stabilization plus protein-synthesis-stimulation mechanism that drives both damage prevention and active regeneration.
Table of Contents
- 2,000 Years of Traditional Use
- The Silymarin Flavonolignan Complex
- German Commission E and EMA Monographs
- Alcoholic Liver Disease — Trials and Cochrane Meta-Analyses
- Cirrhosis Trials (Trinks, Ferenci, Pares)
- Non-Alcoholic Fatty Liver Disease (NAFLD/NASH)
- The Amanita phalloides Antidote — Legalon SIL IV
- Hepatic Regeneration Mechanism (RNA Polymerase I)
- Hepatocyte Membrane Stabilization (OATP1B3 Block)
- Dosing Protocols, Forms, and Bioavailability
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
2,000 Years of Traditional Use
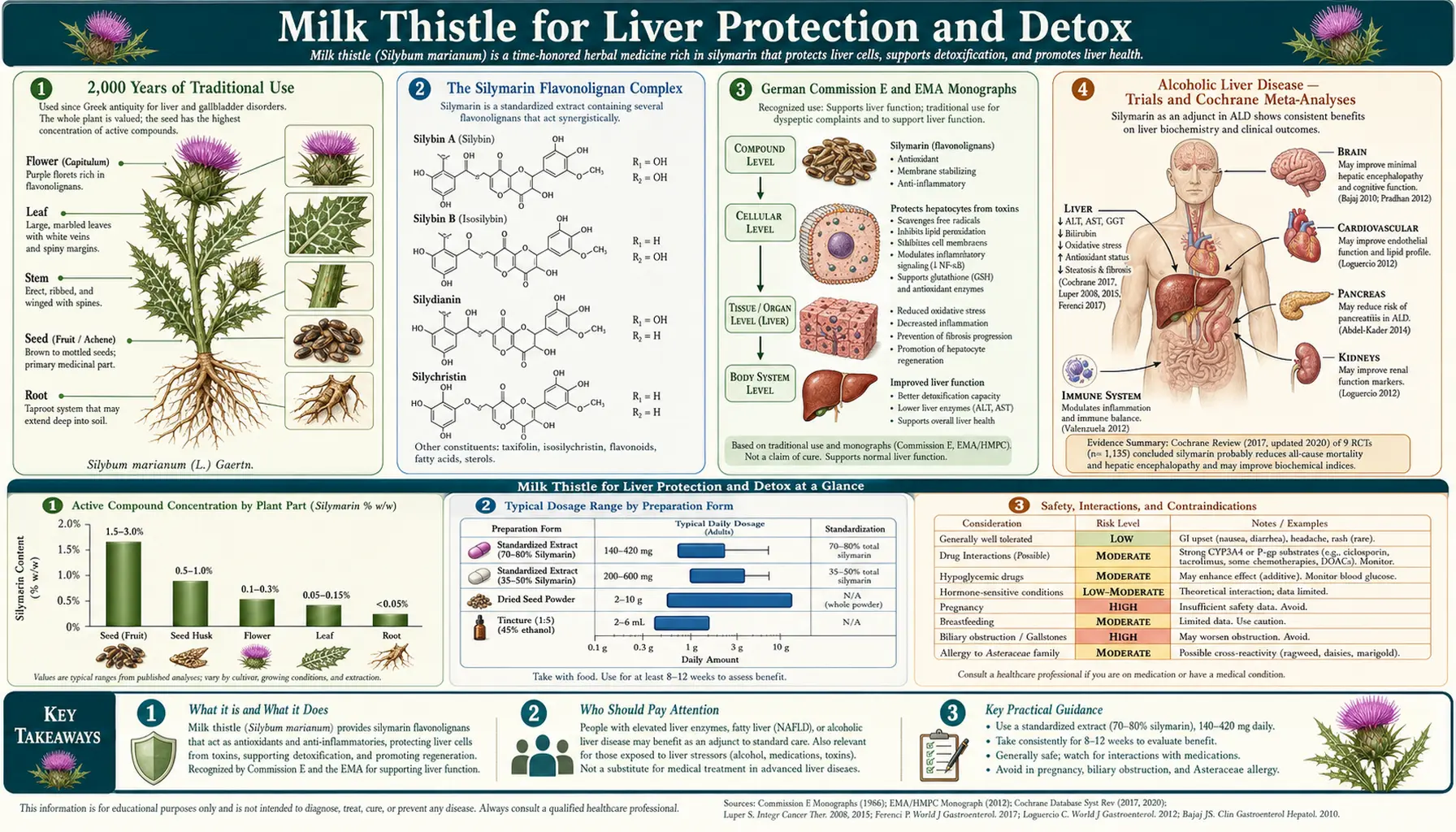
Milk thistle (Silybum marianum; Asteraceae family) is native to the Mediterranean basin and parts of Asia. The plant's common name derives from the white veining on its leaves, which medieval Christian tradition attributed to drops of the Virgin Mary's milk — the species epithet marianum shares the same etymology.
The earliest documented medicinal use comes from Dioscorides, the 1st-century-CE Greek physician whose De Materia Medica remained the dominant Western pharmacopeia for over fifteen centuries. Dioscorides recommended the plant for "carrying off bile." Pliny the Elder, writing in the same era, recorded its use specifically for liver complaints and as a "blood purifier."
The herb appears continuously throughout the European medieval and Renaissance herbal tradition. Nicholas Culpeper, the 17th-century English herbalist, wrote that milk thistle was "as good as any in the world for dropsy, opening obstructions of the liver and spleen." German physicians made it the central liver herb in the 18th and 19th centuries, and Eclectic medicine in 19th-century America (King's American Dispensatory) listed it as a specific for hepatic congestion and "passive congestion of the abdominal viscera."
The modern phytochemistry began in 1968 when Wagner and colleagues at the University of Munich isolated and characterized the silymarin complex. The first standardized pharmaceutical preparation, Legalon (manufactured by Madaus, now Mylan), was introduced in Germany in 1969 and has remained the reference standard against which other preparations are compared. Legalon's standardization to 70-80% silymarin (with defined silybin content) is the basis on which essentially all rigorous clinical trials have been conducted.
The Silymarin Flavonolignan Complex
"Silymarin" refers not to a single molecule but to a defined mixture of flavonolignans extracted from the seed (more precisely, the achene, the dry indehiscent fruit) of Silybum marianum. Standardized silymarin contains:
- Silybin A and silybin B — the two diastereoisomers of the principal active compound, together called "silibinin." Silybin accounts for approximately 60-70% of total silymarin. Silybin A and B are present in roughly equimolar amounts and share the same flavonolignan skeleton (3-O,4-O-bond between taxifolin and coniferyl alcohol) but differ in stereochemistry at two chiral centers. Both isomers are pharmacologically active, with silybin B slightly more potent on most assays.
- Isosilybin A and B — structural isomers of silybin (regiochemistry of the flavonolignan bond differs), accounting for approximately 5-10% of silymarin. Isosilybin is the most potent inhibitor of prostate cancer cell proliferation in vitro and is being investigated as a possible cancer chemopreventive.
- Silychristin — approximately 10-20% of silymarin, with strong direct antioxidant activity and a distinct mechanism affecting thyroid hormone transport via MCT8.
- Silydianin — approximately 5% of silymarin, less studied than the others but contributes to the overall antioxidant capacity.
- Taxifolin (dihydroquercetin) — the flavonoid precursor of all the flavonolignans, present in small amounts and contributing flavonoid antioxidant activity.
The pharmacologic implication of this complex composition is that preparation matters enormously. Generic supermarket capsules labeled "milk thistle" with no silymarin assay may contain anywhere from 30% to 80% silymarin and may have wildly different silybin fractions. Clinical trials use standardized preparations — usually Legalon, Siliphos, or pharmacopoeial-grade silymarin meeting the European Pharmacopoeia monograph — and results from those trials should not be generalized to unstandardized commercial products.
German Commission E and EMA Monographs
Milk thistle is one of the few herbal medicines to have received explicit positive regulatory monographs from both the German Commission E (1986) and the European Medicines Agency HMPC (Committee on Herbal Medicinal Products) monograph (finalized 2018).
The German Commission E Monograph (1986) lists milk thistle fruit and standardized silymarin extract as approved for:
- Dyspeptic complaints
- Toxic liver damage
- Supportive treatment in chronic inflammatory liver disease and hepatic cirrhosis
Recommended daily dose per Commission E: 12-15 g of crushed seeds, or pharmaceutical preparations equivalent to 200-400 mg silymarin (calculated as silybin) daily. No serious adverse effects are recognized; the only contraindication listed is rare allergic reaction in patients sensitive to other Asteraceae family plants (ragweed, daisies, marigolds).
The EMA HMPC monograph (Committee on Herbal Medicinal Products, "Silybi mariani extractum siccum raffinatum et normatum," adopted 2018) recognizes the same essential indications under the EMA's "Well-Established Use" category for liver indications (supportive treatment in chronic inflammatory liver disease, hepatic cirrhosis, and toxic liver damage) and under the EMA's "Traditional Use" category for dyspeptic complaints. The HMPC dose range mirrors Commission E.
The WHO Monograph on Selected Medicinal Plants Volume 2 (1999) provides the global traditional-medicine reference, listing the same liver indications and the dosing range of 200-400 mg silymarin per day in divided doses.
These three monographs together represent the most authoritative herbal regulatory recognition for any single botanical — comparable in regulatory standing to ginkgo for cognitive complaints and St. John's wort for mild depression.
Alcoholic Liver Disease — Trials and Cochrane Meta-Analyses
The largest body of human clinical-trial evidence on milk thistle is in alcoholic liver disease (ALD). The clinical question is whether silymarin slows progression from alcoholic hepatitis or steatohepatitis to cirrhosis, and whether it improves survival in cirrhotic patients who continue to drink.
The pivotal early trials were European, conducted from the 1970s through the 1990s. The most-cited is the Ferenci trial (Vienna, 1989): 170 patients with histologically-confirmed cirrhosis (predominantly alcoholic) were randomized to 420 mg/day silymarin or placebo for an average of 41 months. The trial reported a 4-year survival of 58% in the silymarin group versus 39% in placebo. The benefit was strongest in the Child-Pugh A (compensated cirrhosis) subgroup and in the alcohol-etiology subgroup. Mean follow-up was 41 months.
The subsequent Pares trial (Barcelona, 1998) was larger (200 patients), restricted to alcoholic cirrhosis, and ran for two years. It did not replicate the Ferenci survival benefit. This discrepancy — positive results in earlier smaller trials and null results in later larger trials — runs through the entire milk thistle literature and is the principal reason the herb remains controversial in conventional hepatology despite its strong regulatory monographs.
The Cochrane Review on milk thistle for alcoholic and/or hepatitis B or C liver disease (Rambaldi, Jacobs, Gluud, 2007, updating their 2005 review) pooled 13 randomized trials with a total of 915 patients. The conclusions:
- For mortality: silymarin did not significantly reduce all-cause mortality (relative risk 0.78, 95% CI 0.53-1.15) or liver-related mortality (RR 0.91, 95% CI 0.52-1.59)
- For liver-related complications: no significant effect
- For aminotransferases (ALT/AST): silymarin produced modest reductions (statistically significant but of uncertain clinical importance)
- Quality assessment: most trials were small and had methodological limitations; the authors noted that adequately-powered, high-quality trials were needed before silymarin could be recommended or rejected
The honest summary: silymarin produces modest improvements in biochemical markers of liver damage (transaminases, bilirubin) and may produce small subgroup benefits in compensated alcoholic cirrhosis, but the highest-quality trials have not shown a survival benefit. The German and EMA regulatory authorities consider this sufficient to support the existing monograph indications; the U.S. FDA does not.
For patients with active alcoholic liver disease, milk thistle is best understood as an adjunct that may reduce inflammation while patients pursue the only definitively effective intervention — alcohol abstinence. See our Liver Disease page and Cirrhosis page for the broader clinical context.
Cirrhosis Trials (Trinks, Ferenci, Pares)
The cirrhosis trial set deserves separate attention because cirrhosis is the highest-stakes liver disease for which milk thistle has been tested, and because the discordance between trials is so instructive.
The Trinks trial (Munich, 1981) was an early double-blind placebo-controlled study of 36 patients with alcoholic cirrhosis randomized to silymarin or placebo. It reported normalization of serum bilirubin and aminotransferases in the silymarin group and was widely cited as supporting use.
The Ferenci trial (1989), as described above, was the landmark survival trial — 170 patients, 41 months mean follow-up, significant survival benefit in compensated cirrhosis and alcohol-etiology subgroups.
The Pares trial (1998) attempted to replicate Ferenci with 200 alcoholic cirrhosis patients. Two-year follow-up. No significant survival benefit. Critics noted that the Pares cohort had more advanced disease at baseline (more Child-Pugh B and C), shorter follow-up than Ferenci, and continued drinking by a substantial fraction of both arms — possibly diluting any benefit.
The Lucena trial (2002) in chronic alcoholic liver disease showed silymarin reduced lipid peroxidation markers (MDA) and improved glutathione status but did not move clinical endpoints.
Most modern hepatology guidelines do not recommend silymarin as a standard-of-care intervention in cirrhosis but acknowledge that the European regulatory monographs reflect a defensible interpretation of the totality of evidence. The herb is widely used in Germany, Austria, and Italy as an adjunct in chronic liver disease management.
Non-Alcoholic Fatty Liver Disease (NAFLD/NASH)
NAFLD and its progressive form NASH (non-alcoholic steatohepatitis) are now the leading cause of chronic liver disease in the United States and most developed countries, affecting an estimated 25-30% of adults. The pharmaceutical pipeline has been disappointing — no FDA-approved drug exists for NASH as of this writing (resmetirom was approved in 2024 for NASH with fibrosis but uptake remains limited). This has driven interest in milk thistle as a possible NAFLD adjunct.
The trial base is encouraging but small. The Solhi trial (2014) randomized 50 NAFLD patients to silymarin (140 mg three times daily) or placebo for 8 weeks. The silymarin group showed significant reductions in ALT and AST. The Hashemi trial (2009) reported similar transaminase improvements in 50 NASH patients.
The 2017 Kheong trial (Malaysia) was the largest properly-designed silymarin NAFLD trial: 99 patients with biopsy-proven NASH, randomized to high-dose silymarin (700 mg three times daily, IdB 1016 formulation) versus placebo for 48 weeks. Results were modest: a numerical but not statistically significant reduction in fibrosis stage in the treated arm. Most secondary endpoints favored silymarin.
For NAFLD patients (the bulk of whom are not on any pharmaceutical regimen), milk thistle 420-700 mg/day for 6-12 months is a reasonable adjunct alongside weight loss, dietary intervention (Mediterranean diet), and management of metabolic syndrome components. See our NAFLD page for the full clinical approach.
The Amanita phalloides Antidote — Legalon SIL IV
The most dramatic clinical application of milk thistle in modern medicine is the use of intravenous silibinin (Legalon SIL, manufactured by Madaus) as the standard-of-care antidote for Amanita phalloides (death cap) mushroom poisoning across Europe. This indication is unique in herbal medicine — nowhere else does a botanical extract serve as a registered emergency-medicine intravenous antidote.
Amanita phalloides ingestion is uncommon (estimated 50-100 cases annually in Europe, 5-10 in the United States) but devastating: untreated mortality is approximately 20-25%, driven by hepatic necrosis from the cyclopeptide toxins alpha-amanitin and phalloidin. Death typically occurs 6-16 days post-ingestion from fulminant hepatic failure, often requiring emergency liver transplantation.
The toxin uptake mechanism is the key. Alpha-amanitin enters hepatocytes via the OATP1B3 sodium-independent organic-anion transporter on the sinusoidal (basolateral) membrane of hepatocytes. Once inside, it irreversibly inhibits RNA polymerase II, halting messenger RNA transcription and killing the cell. Silybin competitively blocks OATP1B3, preventing alpha-amanitin uptake.
The IV protocol: Legalon SIL is given as a 5 mg/kg loading dose over 1 hour, followed by 20 mg/kg/day as continuous infusion for 48-96 hours. Treatment must be started as soon as possible after ingestion — ideally within 48 hours, before significant hepatocellular necrosis has occurred. Patients identified earlier (still in the asymptomatic latency phase 6-24 hours post-ingestion) have the best outcomes.
The largest case series, by Mengs and colleagues (2012, Current Pharmaceutical Biotechnology), reported 1,491 patients treated with Legalon SIL: mortality 8.8% overall, dropping to under 5% when treatment was started within 48 hours of ingestion. Historical controls (no specific antidote, supportive care only) show mortality of 20-25%. Although a randomized controlled trial of mushroom-poisoning antidote is ethically impossible, the magnitude and consistency of benefit across European poison centers is regarded as definitive.
Legalon SIL is not FDA-approved in the United States, but the FDA grants emergency-use access through Investigational New Drug applications — U.S. poison centers can obtain it within 24 hours through the FDA expanded-access program. North American poison control protocols increasingly call for it as first-line antidote in confirmed or strongly suspected Amanita ingestion.
Hepatic Regeneration Mechanism (RNA Polymerase I)
The mechanism that distinguishes milk thistle from most other hepatoprotectants is that it does not merely prevent liver damage — it actively stimulates regeneration of damaged hepatocytes. The mechanism is silybin's stimulation of nucleolar RNA polymerase I.
RNA polymerase I is the enzyme responsible for transcribing ribosomal RNA (rRNA) genes. Because ribosomal RNA assembles into ribosomes that in turn manufacture all cellular proteins, RNA polymerase I activity is the rate-limiting step in protein synthesis. In rapidly-regenerating tissue (the regenerating liver after partial hepatectomy or toxic injury), RNA polymerase I activity surges, supporting the protein synthesis needed for cell growth and division.
Silybin binds to a specific site on the nucleolar polymerase complex and increases its transcriptional activity. The result is enhanced rRNA production, increased ribosome assembly, and accelerated protein synthesis — precisely what damaged liver cells need to recover. In experimental models of liver injury (partial hepatectomy, CCl4 toxicity, ischemia-reperfusion), silybin pretreatment accelerates the restoration of liver mass and the recovery of hepatic synthetic function.
This regenerative mechanism is distinct from (and complementary to) the membrane-stabilization and OATP1B3-blocking effects described in the next section. Together they explain why milk thistle works as both a prophylactic (taken before known toxin exposure, e.g., chemotherapy) and a rescue agent (started after acute hepatic injury). The Amanita protocol exploits both: silybin blocks further toxin uptake while simultaneously stimulating regeneration of cells that have already been damaged but not yet died.
Hepatocyte Membrane Stabilization (OATP1B3 Block)
The second mechanism on which essentially all milk thistle clinical effects depend is hepatocyte membrane stabilization. Silybin physically intercalates into the phospholipid bilayer of the hepatocyte plasma membrane, altering membrane fluidity and structurally protecting the membrane against toxin-induced permeabilization.
The membrane effect has two components. The first is the OATP1B3 transporter block already discussed for amanita. OATP1B3 (organic anion-transporting polypeptide 1B3) is one of the principal hepatocyte uptake transporters for amphipathic anionic compounds, including bilirubin, bile acids, several drugs (atorvastatin, fexofenadine), and toxic anions such as phalloidin and amanitin. Silybin's competitive inhibition of OATP1B3 reduces hepatocellular uptake of toxic substrates — a generalizable mechanism that protects against multiple chemical insults, not just amanita.
The second component is the membrane fluidity effect. By intercalating into the lipid bilayer, silybin modestly stiffens the membrane and reduces its permeability to small toxic molecules that would otherwise diffuse passively into the cell. In animal models, this effect protects against carbon tetrachloride (CCl4), thioacetamide, galactosamine, acetaminophen overdose, halothane hepatotoxicity, and chronic ethanol-induced injury.
The clinical translation extends beyond exotic poisonings. In oncology, silymarin is being studied as a chemoprotectant against the hepatotoxicity of methotrexate, cisplatin, doxorubicin, and tamoxifen. The trial base remains preliminary — most data are from animal models and small clinical pilot studies — but the mechanistic rationale is strong and consistent with the broader hepatocyte-protection picture.
Dosing Protocols, Forms, and Bioavailability
Standardized silymarin (Legalon equivalent): 420 mg/day in three divided doses (140 mg three times daily) is the canonical European hepatology dose, derived from Commission E and used in the Ferenci cirrhosis trial. Lower-end maintenance dosing for general liver support is 200-280 mg/day. Higher-dose protocols (700 mg three times daily, 2,100 mg/day) have been used in NASH and HCV trials.
Siliphos / IdB 1016 (silybin-phosphatidylcholine complex): The bioavailability problem with oral milk thistle is real — free silybin has 20-50% oral bioavailability with extensive first-pass conjugation. Siliphos (the Indena IdB 1016 preparation, also marketed as Siliphos by Thorne) complexes silybin with phosphatidylcholine to improve lipid-membrane partitioning. The result is approximately 4.6-fold higher silybin plasma concentrations from an equivalent silybin dose. Typical Siliphos dose: 120-360 mg/day, equivalent to roughly 540-1,620 mg of standard silymarin.
Whole-seed and tincture forms: The crushed seed (12-15 g/day per Commission E) and alcoholic tincture have a long traditional-use record but are not standardized and are not used in modern clinical trials. They are suitable for general digestive and gentle liver support; not for serious hepatic disease management.
Intravenous Legalon SIL: 5 mg/kg loading then 20 mg/kg/day continuous infusion for amanita poisoning (hospital-only).
Bioavailability optimization: Take with a meal containing some fat to enhance absorption. Avoid taking with high-fiber meals (fiber binds silymarin in the gut). Bedtime dosing may be preferred for one of the three daily doses to provide overnight liver exposure.
Duration: Liver-disease trials typically run 6-12 months. For prophylactic use during known hepatotoxic exposure (e.g., a course of acetaminophen, tuberculosis therapy with isoniazid, methotrexate), pretreatment for 1-2 weeks before and continuation throughout exposure is reasonable. Indefinite long-term use is generally regarded as safe.
Cautions and Drug Interactions
- Asteraceae allergy — patients with documented allergy to ragweed, daisies, chrysanthemums, marigolds, or other Asteraceae plants should use milk thistle cautiously or not at all. Cross-reactivity is uncommon but documented.
- Mild GI side effects — bloating, mild diarrhea, and abdominal discomfort are reported in approximately 2-10% of users at standard doses and tend to resolve with dose reduction or splitting doses with food.
- Estrogenic activity — silymarin has weak estrogen-receptor binding in vitro. The clinical relevance is uncertain but caution is advised in patients with estrogen-sensitive conditions (hormone-receptor-positive breast cancer, endometriosis). Conservative practice avoids high-dose milk thistle in these populations.
- CYP450 drug interactions — silymarin weakly inhibits CYP3A4, CYP2C9, and CYP2D6 in vitro. Clinically significant interactions are uncommon at standard doses but theoretically possible with narrow-therapeutic-index drugs (warfarin, certain anticonvulsants, immunosuppressants). Patients on critical pharmacotherapy should consult their prescriber before adding milk thistle.
- Pregnancy and lactation — not specifically contraindicated, with a long traditional-use record in pregnant women. However, modern controlled safety data are limited, and conservative practice avoids new initiation in pregnancy. The intravenous Legalon SIL formulation is given in life-threatening mushroom poisoning regardless of pregnancy status.
- Hemochromatosis and iron overload — one paradoxical concern: silymarin chelates iron in vitro and may reduce iron absorption from a meal. In iron-deficient patients this could matter; in iron-overloaded patients (hereditary hemochromatosis) it is actually beneficial.
- Hypoglycemic potentiation — silymarin modestly improves insulin sensitivity in diabetics. Patients on insulin or sulfonylureas should monitor blood glucose more closely after starting milk thistle as a precaution.
- Not a substitute for definitive treatment — for active alcoholic liver disease, alcohol abstinence remains the only definitively effective intervention. For chronic HBV and HCV, direct-acting antivirals are first-line. Milk thistle is adjunctive, not curative.
Key Research Papers
- Ferenci P et al. (1989). Randomized controlled trial of silymarin treatment in patients with cirrhosis of the liver. J Hepatol 9(1):105-13. — PubMed
- Pares A et al. (1998). Effects of silymarin in alcoholic patients with cirrhosis of the liver: results of a controlled, double-blind, randomized and multicenter trial. J Hepatol 28(4):615-21. — PubMed
- Rambaldi A, Jacobs BP, Gluud C (2007). Milk thistle for alcoholic and/or hepatitis B or C virus liver diseases. Cochrane Database Syst Rev 2007(4):CD003620. — PubMed
- Mengs U, Pohl RT, Mitchell T (2012). Legalon SIL: the antidote of choice in patients with acute hepatotoxicity from amatoxin poisoning. Curr Pharm Biotechnol 13(10):1964-70. — PubMed
- Saller R, Meier R, Brignoli R (2001). The use of silymarin in the treatment of liver diseases. Drugs 61(14):2035-63. — PubMed
- Loguercio C, Festi D (2011). Silybin and the liver: from basic research to clinical practice. World J Gastroenterol 17(18):2288-301. — PubMed
- Kheong CW et al. (2017). A randomized trial of silymarin for the treatment of nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol 15(12):1940-1949. — PubMed
- Trinks J et al. (1981). Behandlung der chronisch-aggressiven Hepatitis und der alkoholischen Leberzirrhose mit Silymarin. Med Welt. — PubMed
- Letteron P et al. (1990). Mechanism for the protective effects of silymarin against carbon tetrachloride-induced lipid peroxidation and hepatotoxicity in mice. Biochem Pharmacol 39(12):2027-34. — PubMed
- Sonnenbichler J, Goldberg M, Hane L, Madubunyi I, Vogl S, Zetl I (1986). Stimulatory effect of silibinin on the DNA synthesis in partially hepatectomized rat livers. Biochem Pharmacol 35(3):538-41. — PubMed
- Floersheim GL, Eberhard M, Tschumi P, Duckert F (1982). Effects of penicillin and silymarin on liver enzymes and blood clotting factors in dogs given a boiled preparation of Amanita phalloides. Toxicol Appl Pharmacol 64(2):262-75. — PubMed
- Magdalan J et al. (2010). Influence of commonly used clinical antidotes on antioxidant systems in human hepatocyte culture intoxicated with alpha-amanitin. Hum Exp Toxicol 30(1):38-43. — PubMed
PubMed Topic Searches
- PubMed: Silymarin alcoholic liver disease
- PubMed: Silibinin amanita phalloides antidote
- PubMed: Silymarin cirrhosis meta-analysis
- PubMed: Silymarin NAFLD/NASH
- PubMed: Silybin hepatic regeneration
- PubMed: Silybin OATP1B3 transporter
Connections
- Milk Thistle Overview
- Milk Thistle Benefits Hub
- Antioxidant & Glutathione
- Hepatitis Adjunctive
- Skin Health
- Liver Disease
- Cirrhosis
- Non-Alcoholic Fatty Liver Disease
- Hepatitis
- Hepatitis C
- Hemochromatosis (Iron Overload)
- Liver Cleansing
- Detox Protocols
- Turmeric
- Dandelion
- Chanca Piedra
- Chanca Piedra: Liver Protection and Hepatitis B — HBV-specific antiviral mechanism, niranthin vs nucleoside analogs, trial evidence on HBsAg/HBV-DNA, and adjunctive use with entecavir/tenofovir.
- N-Acetylcysteine (NAC)
- Glutathione
- Comprehensive Metabolic Panel
- GGT
- All Herbs