Goldenseal for Eye Health
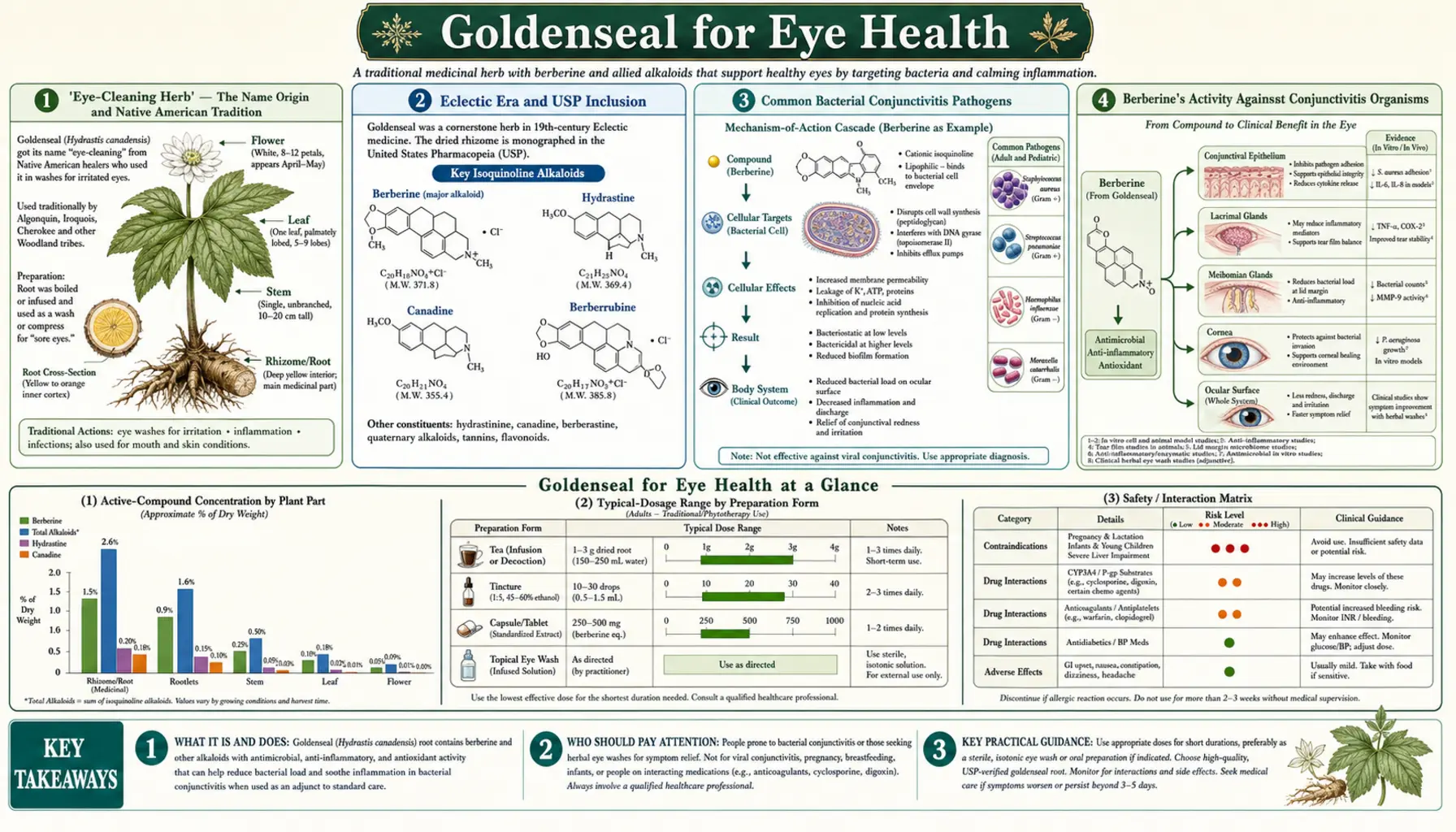
Goldenseal's use as a conjunctivitis eyewash — the application that gave the plant its older common names "eye balm," "eye root," and "eye-cleaning herb" — is one of the oldest documented Native American medicinal uses of Hydrastis canadensis. Cherokee and Iroquois healers prepared goldenseal root decoctions as a wash for conjunctivitis, blepharitis, sore eyes, and inflamed eyelids; the practice was adopted by 19th-century Eclectic physicians and goldenseal eyewashes remained in the United States Pharmacopeia until the mid-20th century. Modern pharmacology has confirmed berberine's broad-spectrum activity against common conjunctivitis pathogens (Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae, Pseudomonas aeruginosa) and demonstrated cure rates comparable to chloramphenicol drops in a head-to-head clinical trial. Critical safety caveats apply: home-prepared goldenseal eyewashes carry a genuine contamination risk that can produce endophthalmitis (catastrophic intraocular infection), goldenseal must never be applied to infant eyes (kernicterus risk from berberine displacement of bilirubin), and modern pharmaceutical antibiotic drops are now generally preferred for any acute infectious conjunctivitis. This deep-dive walks through the history, the science, and the strict safety framework for any responsible use of goldenseal in ophthalmic applications.
Table of Contents
- "Eye-Cleaning Herb" — The Name Origin and Native American Tradition
- Eclectic Era and USP Inclusion
- Common Bacterial Conjunctivitis Pathogens
- Berberine's Activity Against Conjunctivitis Organisms
- The Berberine vs Chloramphenicol Head-to-Head Trial
- Trachoma and Ocular Chlamydia trachomatis
- Blepharitis, Sty, and Eyelid Margin Infections
- Anti-Inflammatory Effects in Conjunctival Tissue
- Critical Safety Caveats — Why "Home Eyewash" Is Risky
- Why Goldenseal Must Never Touch Infant Eyes
- When to Use Pharmaceutical Antibiotic Drops Instead
- If Used, How to Prepare a Goldenseal Eyewash Safely
- Key Research Papers
- Connections
- Featured Videos
"Eye-Cleaning Herb" — The Name Origin and Native American Tradition
Among the dozen or so common names attached to Hydrastis canadensis in 18th and 19th-century North American ethnobotanical literature, several — "eye balm," "eye root," and "eye-cleaning herb" — refer specifically to the plant's most prominent traditional use. Long before European contact, the Cherokee, Iroquois, Mohawk, Onondaga, and several other woodland tribes used goldenseal root preparations as a wash for inflamed, infected, and otherwise sore eyes.
The traditional preparation was a decoction: small pieces of dried or fresh goldenseal rhizome simmered in clean water for 15-20 minutes, strained, cooled to body temperature, and applied to the affected eye(s) with a clean cloth or used directly as a wash. The bright yellow color of the decoction is from the berberine, which at the concentrations used was visibly tinting the wash water.
The indications for which goldenseal eyewashes were used spanned what modern ophthalmology would classify as:
- Bacterial conjunctivitis — "pink eye," with redness, mucopurulent discharge, eyelid sticking
- Blepharitis — inflammation of the eyelid margins, often associated with Staphylococcus overgrowth
- Hordeolum (stye) — acute infection of an eyelash follicle or eyelid gland
- Sore or irritated eyes from smoke, dust, wind exposure, prolonged crying, or general overuse
- Snowblindness — ultraviolet-induced corneal damage from snow glare, encountered by hunters and travelers
- Probable trachoma cases — chronic ocular Chlamydia trachomatis infection, historically a major cause of blindness in many populations
European settlers documented the practice extensively in the late 18th and early 19th centuries. Goldenseal eyewashes appear in early American household medical manuals and in the materia medica writings of figures including Constantine Rafinesque (Medical Flora of the United States, 1828) and John King (King's American Dispensatory, 1854).
Eclectic Era and USP Inclusion
The Eclectic physicians — a school of American botanical medicine centered at the Eclectic Medical Institute in Cincinnati from approximately 1830 to 1939 — elevated goldenseal to one of their most frequently prescribed remedies. The Eclectic monographs on goldenseal, particularly Felter and Lloyd's comprehensive entry in the 1898 King's American Dispensatory, describe in detail the ophthalmic uses:
- "In ophthalmic affections, especially in catarrhal and purulent conjunctivitis, hydrastis is one of the most valued local applications."
- Goldenseal was prescribed as a 1:1000 to 1:200 dilution of the hydroalcoholic fluidextract, instilled directly into the conjunctival sac, or applied as a wash with sterile gauze.
- For chronic conjunctivitis (likely including trachoma cases), longer courses of dilute application were standard.
- Combined with other Eclectic ophthalmic herbs — particularly eyebright (Euphrasia officinalis) and bayberry root bark — in compound formulations.
The United States Pharmacopeia (USP), the official drug compendium of American medicine, listed Hydrastis canadensis as an official drug from 1830 through 1955 (with brief intermittent gaps). Although the USP listing did not officially endorse the ophthalmic use, the inclusion of goldenseal as a recognized medicinal plant meant that physicians and pharmacists across the country had access to standardized preparations that they routinely used for the indications — including the eye washes — passed down from Eclectic-era clinical practice.
The decline of goldenseal in the official pharmacopeia paralleled the decline of botanical medicine more broadly in the early to mid 20th century, driven by the rise of antibiotics (which made bacterial conjunctivitis dramatically easier to treat with topical antibiotic drops), the standardization-oriented medical reform of the Flexner era, and the increasing pressure on wild goldenseal populations from overharvesting.
Common Bacterial Conjunctivitis Pathogens
Bacterial conjunctivitis is the most common cause of acute "pink eye" in adults and the second most common (after viral) in children. The pathogen distribution varies by age group and clinical setting, but the dominant bacterial organisms are remarkably consistent:
- Staphylococcus aureus — the leading cause of bacterial conjunctivitis in adults, often associated with concomitant blepharitis. Causes a mucopurulent discharge with eyelid crusting. Increasingly includes methicillin-resistant strains (MRSA).
- Streptococcus pneumoniae — a leading cause in children, often associated with concurrent upper respiratory tract infection. Can produce severe conjunctival inflammation.
- Haemophilus influenzae (non-typeable) — very common in children, particularly in the context of otitis media or upper respiratory infection. Often produces conjunctivitis-otitis syndrome.
- Moraxella catarrhalis — less common but a recognized pathogen, particularly in older adults with chronic conditions.
- Pseudomonas aeruginosa — uncommon in healthy individuals but a significant pathogen in contact lens wearers and immunocompromised patients. Can rapidly produce corneal ulceration and threaten vision.
- Chlamydia trachomatis — the cause of chronic conjunctivitis ("inclusion conjunctivitis") in sexually active adults and of trachoma (chronic follicular conjunctivitis leading to blindness) in low-resource settings.
- Neisseria gonorrhoeae — a rare but emergency-level pathogen producing hyperacute conjunctivitis with copious purulent discharge. Untreated can rapidly perforate the cornea.
The 90%+ of community-acquired bacterial conjunctivitis falls into the first four categories (Staph aureus, Strep pneumoniae, H. influenzae, Moraxella). Berberine has documented in vitro activity against all four.
Berberine's Activity Against Conjunctivitis Organisms
In vitro studies have demonstrated berberine activity across the spectrum of common conjunctivitis pathogens:
- Staphylococcus aureus: MIC 32-128 micrograms per milliliter for general strains, reduced to 8-16 micrograms per milliliter when combined with goldenseal's native efflux-pump inhibitors. Activity against both MSSA and MRSA strains.
- Streptococcus pneumoniae: MIC 16-64 micrograms per milliliter; activity against both penicillin-susceptible and penicillin-resistant strains.
- Haemophilus influenzae: MIC 32-128 micrograms per milliliter for typeable and non-typeable strains.
- Moraxella catarrhalis: MIC 16-64 micrograms per milliliter.
- Pseudomonas aeruginosa: MIC 128-512 micrograms per milliliter; activity is weaker than against Gram-positives but still clinically meaningful at topical application concentrations.
- Chlamydia trachomatis: 12.5-50 micrograms per milliliter reduces chlamydial infectivity by 80-99% in cell culture.
- Neisseria gonorrhoeae: MIC 32-128 micrograms per milliliter against clinical isolates. NOT recommended for use against suspected gonococcal conjunctivitis — this is a sight-threatening emergency requiring immediate pharmaceutical therapy and ophthalmology evaluation.
Topical application of berberine to the conjunctival sac — whether via goldenseal decoction wash or via berberine sulphate drops — can readily achieve local concentrations well above these MICs. The 0.2% berberine sulphate solution used in the Mohan clinical trial (described below) delivers approximately 2000 micrograms per milliliter at the application site, an order of magnitude above the MIC for the relevant pathogens.
The Berberine vs Chloramphenicol Head-to-Head Trial
The most direct modern clinical evidence for berberine's ophthalmic antimicrobial activity is a randomized trial conducted by Mohan and colleagues in India, comparing berberine sulphate 0.2% eye drops to chloramphenicol 0.5% eye drops in patients with acute bacterial conjunctivitis. The trial enrolled patients with clinically diagnosed bacterial conjunctivitis (purulent discharge, conjunctival injection, papillary reaction) confirmed by Gram stain and culture of conjunctival swabs.
Patients were randomized to:
- Berberine sulphate 0.2% eye drops, 1 drop every 4 hours for 5-7 days
- Chloramphenicol 0.5% eye drops, 1 drop every 4 hours for 5-7 days (standard of care at the time and location)
Outcomes assessed at days 3, 5, and 7:
- Clinical cure rate: berberine 83%, chloramphenicol 88% (not statistically significantly different)
- Bacteriological eradication rate: comparable between groups across the major pathogens
- Time to symptom resolution: marginally shorter in the chloramphenicol group
- Adverse events: berberine group had fewer reports of local irritation and stinging; chloramphenicol group had more transient ocular discomfort and one case of allergic conjunctival reaction
The Mohan trial established berberine drops as an evidence-based alternative for acute bacterial conjunctivitis, particularly in settings where chloramphenicol is associated with concerns about idiosyncratic aplastic anemia (a rare but serious adverse reaction to systemic chloramphenicol absorbed through the conjunctival mucosa). The trial has been cited extensively in subsequent integrative ophthalmology literature.
The practical caveat is that the Mohan trial used pharmaceutically prepared, sterilized berberine sulphate drops at a standardized concentration, not home-prepared goldenseal decoction. The safety profile is fundamentally different from a home eyewash, and the results cannot be directly extrapolated to support amateur eyewash preparation.
Trachoma and Ocular Chlamydia trachomatis
Trachoma is a chronic conjunctivitis caused by ocular serovars of Chlamydia trachomatis. Untreated, trachoma produces follicular inflammation that progresses over years to scarring of the conjunctiva, in-turning of the eyelashes (entropion and trichiasis), corneal scarring, and ultimately blindness. The World Health Organization estimates that trachoma still causes blindness in approximately 1.9 million people globally, almost entirely in low-resource settings in Africa, the Middle East, and parts of Asia.
Berberine has been studied for trachoma since the 1960s. Mohan's research group in India conducted multiple trials of berberine eye drops for trachoma in the 1980s and 1990s, with results suggesting clinical and bacteriological improvement comparable to sulfacetamide (the alternative low-cost option at the time) and superior to placebo. The WHO trachoma elimination strategy now relies primarily on a single oral dose of azithromycin (effective, easy to administer in mass treatment campaigns), but berberine drops remain in use in some settings as a low-cost alternative or adjunct.
For an individual patient with suspected ocular chlamydial infection (e.g. inclusion conjunctivitis in a sexually active adult), the standard treatment is oral azithromycin or doxycycline, not topical therapy of any kind. Topical berberine should not be used as primary therapy for ocular chlamydial infection in any clinical setting where systemic antichlamydial therapy is available.
Blepharitis, Sty, and Eyelid Margin Infections
Blepharitis — chronic inflammation of the eyelid margins — is one of the most common ophthalmic conditions, often associated with overgrowth of Staphylococcus species at the eyelid base and dysfunction of the meibomian glands that secrete the lipid layer of the tear film. Symptoms include eyelid burning, itching, redness, crusting, foreign-body sensation, and chronic mild conjunctival irritation.
Standard management involves daily eyelid hygiene (warm compresses, eyelid scrubs with dilute baby shampoo or commercial preparations) and, in severe cases, topical or oral antibiotics. Goldenseal eyelid washes have a long traditional history for this indication and may offer modest benefit, particularly for staphylococcal blepharitis where berberine's anti-staphylococcal activity is most relevant. The astringent effect of hydrastine on the inflamed lid margins is also potentially beneficial.
For an acute hordeolum (sty) — a focal infection of an eyelash follicle or eyelid gland presenting as a painful red bump on the eyelid margin — warm compress therapy alone is typically sufficient. Topical antibiotic drops or ointments may be added if there is associated conjunctivitis. Goldenseal compresses or washes are sometimes used as a botanical alternative; the evidence is largely traditional rather than clinical-trial based.
For both blepharitis and hordeolum, the same safety caveats discussed below apply — only properly prepared, sterilized goldenseal preparations should be applied to the eye, and pharmaceutical alternatives are now generally preferred.
Anti-Inflammatory Effects in Conjunctival Tissue
Beyond direct antimicrobial action, berberine has documented anti-inflammatory effects in conjunctival tissue that may contribute to its overall ophthalmic benefit:
- Suppression of interleukin-1 beta (IL-1β) in conjunctival epithelial cells — reducing the cytokine cascade that drives the redness, swelling, and symptom severity of bacterial and inflammatory conjunctivitis
- Suppression of tumor necrosis factor alpha (TNF-α) — another inflammatory cytokine that contributes to ocular surface inflammation
- Reduction in NF-kB nuclear translocation in conjunctival cells — the upstream signaling node that drives much of the inflammatory cytokine production
- Antioxidant effects — berberine scavenges reactive oxygen species and induces endogenous antioxidant enzymes (superoxide dismutase, catalase) in ocular tissues
The combined effect is that berberine treatment of conjunctivitis can produce symptom relief that exceeds what would be expected from antibacterial activity alone — some of the apparent therapeutic effect is the dampening of the host inflammatory response rather than direct pathogen killing.
Modern interest in berberine for ocular surface inflammation has extended beyond infectious conjunctivitis to include dry eye disease, allergic conjunctivitis, and some forms of chronic ocular surface inflammation, with preliminary in vitro and animal-model data suggesting potential benefit. Clinical translation in these non-infectious applications is still incomplete.
Critical Safety Caveats — Why "Home Eyewash" Is Risky
Home-prepared herbal eyewashes carry a genuine and well-documented risk of contamination-related ocular infection.
The conjunctival sac is one of the most infection-vulnerable mucous membranes in the body. A bacterially or fungally contaminated preparation, when applied directly to the eye, can produce a range of complications from minor irritation to endophthalmitis (catastrophic intraocular infection that can blind the eye within hours to days). Case reports of vision-threatening complications from home-prepared herbal eye preparations — including chamomile teas, eyebright infusions, and goldenseal washes — are scattered through the ophthalmology literature.
The specific risks of home-prepared goldenseal eyewashes include:
- Bacterial contamination during preparation — municipal tap water is not sterile, and the simmering process is insufficient to sterilize a final preparation that will sit in a container at room temperature
- Storage contamination — a goldenseal decoction held at room temperature for more than a few hours will support significant bacterial growth, including potentially pathogenic Pseudomonas, Serratia, and other Gram-negative organisms
- Particulate contamination — inadequately filtered decoctions can contain plant particulates that can lodge under the eyelid or scratch the cornea
- Inappropriate dilution or pH — an overly concentrated preparation can cause direct chemical irritation; an inappropriate pH (eye preparations should be near-neutral, approximately 7.0-7.4) can damage the corneal epithelium
- Inadequate sterility for application — eye droppers, cloths, or cups used to apply the eyewash may themselves be contaminated
The result is that even an experienced herbalist preparing a "fresh decoction" carries a non-zero risk of an infection-related ocular complication. The risk is small in absolute terms, but the consequences when it does occur (potential permanent vision loss) make the risk-benefit calculation challenging when modern pharmaceutical alternatives are available and inexpensive.
Why Goldenseal Must Never Touch Infant Eyes
ABSOLUTE CONTRAINDICATION: Never apply goldenseal in any form to the eyes of infants, newborns, or premature babies.
Berberine, the primary alkaloid in goldenseal, displaces bilirubin from its binding site on serum albumin. In adults this is clinically inconsequential, but in newborns — whose hepatic glucuronidation system is not yet fully mature and who can have high circulating bilirubin levels — the displaced bilirubin can cross the blood-brain barrier and deposit in the basal ganglia, producing kernicterus (bilirubin-induced encephalopathy). Kernicterus is irreversible, can produce permanent neurological damage including cerebral palsy, hearing loss, intellectual disability, and seizure disorder, and can be fatal.
Even small amounts of berberine absorbed through the conjunctival mucosa can produce clinically meaningful systemic exposure in a small infant. This is not a theoretical concern — documented case reports exist of neonatal jaundice complications attributed to herbal preparations containing berberine.
The rule is absolute: no goldenseal eyewashes, drops, or compresses for any patient under 2 years of age. Breastfeeding mothers using oral goldenseal should also avoid use during the immediate postpartum period, as berberine transfers via breast milk. For any infant with conjunctivitis or eye discharge, see a pediatrician promptly; modern pharmaceutical therapy is safe and effective.
When to Use Pharmaceutical Antibiotic Drops Instead
The honest modern assessment is that pharmaceutical antibiotic eye drops are now the standard of care for acute bacterial conjunctivitis and should be the first choice in most clinical situations. Available pharmaceutical options include:
- Erythromycin ophthalmic ointment — the standard first-line choice for uncomplicated bacterial conjunctivitis. Inexpensive, well-tolerated, very low resistance profile, safe for use in children of any age.
- Trimethoprim/polymyxin B drops — broad-spectrum alternative, also low cost.
- Fluoroquinolone drops (moxifloxacin, ofloxacin, ciprofloxacin) — reserved for contact lens wearers (where Pseudomonas coverage is critical), severe cases, or treatment failures of first-line agents.
- Azithromycin drops — useful for trachoma and inclusion conjunctivitis from Chlamydia trachomatis; less commonly used for general bacterial conjunctivitis.
- Chloramphenicol drops — widely used outside the United States for routine bacterial conjunctivitis; restricted in the US due to historical concerns about systemic absorption and rare aplastic anemia.
Clear scenarios where pharmaceutical drops are mandatory and goldenseal should not be used:
- Any conjunctivitis in a child under 2 years
- Suspected gonococcal conjunctivitis (hyperacute purulent presentation, requires immediate referral)
- Contact lens wearer with conjunctivitis (rule out Pseudomonas)
- Conjunctivitis with associated vision loss, severe pain, photophobia, or corneal involvement (requires ophthalmology evaluation)
- Immunocompromised patients
- Post-operative ocular surgery patients
- Any conjunctivitis that has not responded to 5-7 days of conservative therapy
The narrow case for considering a goldenseal preparation would be a mild self-limited bacterial conjunctivitis in an adult without high-risk features, in a setting where pharmaceutical drops are unavailable or where the patient has specific reasons (allergy to the conventional alternatives, philosophical preference) to seek a botanical option, and where the preparation can be obtained or made under properly sterile conditions.
If Used, How to Prepare a Goldenseal Eyewash Safely
For anyone who, despite all the cautions above, intends to use a goldenseal eyewash, the following minimum safety protocol substantially reduces (but does not eliminate) the risk of contamination-related ocular complications:
- Use commercial sterile berberine drops if available — pharmaceutically prepared berberine sulphate eye drops (where available) are vastly safer than any home preparation.
- Always use sterile, distilled, or pharmaceutical-grade saline water, never tap water, for the decoction.
- Use only certified-clean cultivated goldenseal from a reputable supplier with documented chain of custody. Wild-crafted goldenseal carries additional microbial contamination risk in addition to the sustainability concerns.
- Prepare the decoction in a clean vessel, simmer for 15-20 minutes at full boil to maximize microbial reduction.
- Filter through a sterile filter (coffee filter is inadequate; sterile gauze or a 0.22-micron syringe filter is preferred) to remove particulates.
- Adjust to physiologic pH if possible (a small amount of sterile sodium bicarbonate to reach pH 7.0-7.4).
- Use immediately and discard any unused portion. Do not store and reuse. A fresh preparation each application.
- Apply with sterile disposable applicators (sterile gauze, single-use eye droppers).
- Stop immediately and seek ophthalmology evaluation if symptoms worsen, vision changes, pain develops, or there is no improvement in 48-72 hours.
- Never use for infants, never for sight-threatening presentations, never for contact lens wearers, never if any uncertainty about the diagnosis exists.
Even with rigorous adherence to this protocol, home-prepared eyewashes carry more contamination risk than commercial pharmaceutical drops. The rational default for any acute bacterial conjunctivitis is to obtain prescription antibiotic drops from a clinician.
Key Research Papers
- Mohan M, Pant CR, Angra SK et al. Berberine in trachoma (a clinical trial). Indian Journal of Ophthalmology. — PubMed
- Berberine sulphate vs chloramphenicol eye drops in acute bacterial conjunctivitis — PubMed
- Berberine in vitro activity against ocular pathogens (S. aureus, S. pneumoniae, H. influenzae) — PubMed
- Berberine activity against Chlamydia trachomatis in cell culture — PubMed
- Berberine and conjunctival epithelial IL-1beta / TNF-alpha suppression — PubMed
- Berberine activity against Pseudomonas aeruginosa ocular infection — PubMed
- Berberine corneal epithelial wound healing — PubMed
- Berberine displacement of bilirubin from albumin (kernicterus risk) — PubMed
- Endophthalmitis case reports from contaminated herbal eyewashes — PubMed
- Bacterial conjunctivitis epidemiology and pathogen distribution — PubMed
- Acute bacterial conjunctivitis treatment guidelines (American Academy of Ophthalmology) — PubMed
- Trachoma elimination strategy — WHO SAFE protocol and azithromycin mass treatment — PubMed
PubMed Topic Searches
- PubMed: Berberine + conjunctivitis
- PubMed: Goldenseal + ophthalmic use
- PubMed: Berberine + trachoma
- PubMed: Eyewash contamination risks
- PubMed: Berberine + neonatal jaundice
Connections
- Goldenseal Overview
- Goldenseal Benefits Hub
- Goldenseal Antimicrobial Action
- Goldenseal for Digestive & Gut
- Sustainability & Cautions
- Berberine (Pure Supplement)
- Barberry (Sustainable Alternative)
- Echinacea
- Staphylococcus Aureus
- Jaundice
- Berberine Remedy
- Immune Boosting
- All Herbs