Goldenseal for Digestive & Gut Health
Goldenseal's digestive applications are one of its most clinically supported and most paradoxically practical uses. Berberine's notoriously poor systemic oral bioavailability (approximately 5%) is actually a therapeutic advantage in the gut: the unabsorbed 95% remains in the lumen, where it can directly contact intestinal pathogens at clinically meaningful concentrations. This makes goldenseal (and other berberine-rich plants) uniquely suited to in-gut antimicrobial action against bacterial diarrhea, C. difficile, H. pylori, and small intestinal bacterial overgrowth (SIBO). Layered on top of the antimicrobial action are three complementary digestive effects: bitter-principle vagal stimulation of saliva/gastric acid/bile, mucous-membrane astringency from hydrastine, and direct inhibition of bacterial enterotoxin-driven intestinal fluid secretion. This deep-dive walks through each digestive application, the supporting clinical evidence (including the landmark 2014 Johns Hopkins SIBO trial), the comparison to cheaper berberine sources, and the practical considerations for using goldenseal as part of a gut-restoration protocol.
Table of Contents
- Bitter Principles and Digestive Stimulation
- Why Poor Bioavailability Becomes a Gut-Therapy Advantage
- Bacterial Diarrhea (E. coli, V. cholerae, Shigella)
- Clostridioides difficile and Toxin Inhibition
- SIBO and the Johns Hopkins Trial
- Helicobacter pylori and Peptic Ulcer Adjunct
- Direct Inhibition of Enterotoxin-Driven Cl− Secretion
- Inflammatory Bowel Disease Adjunct Pilot Data
- Intestinal Barrier and Microbiome Effects
- Comparison to Barberry, Oregon Grape, and Pure Berberine HCl
- Practical Dosing for Gut Applications
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
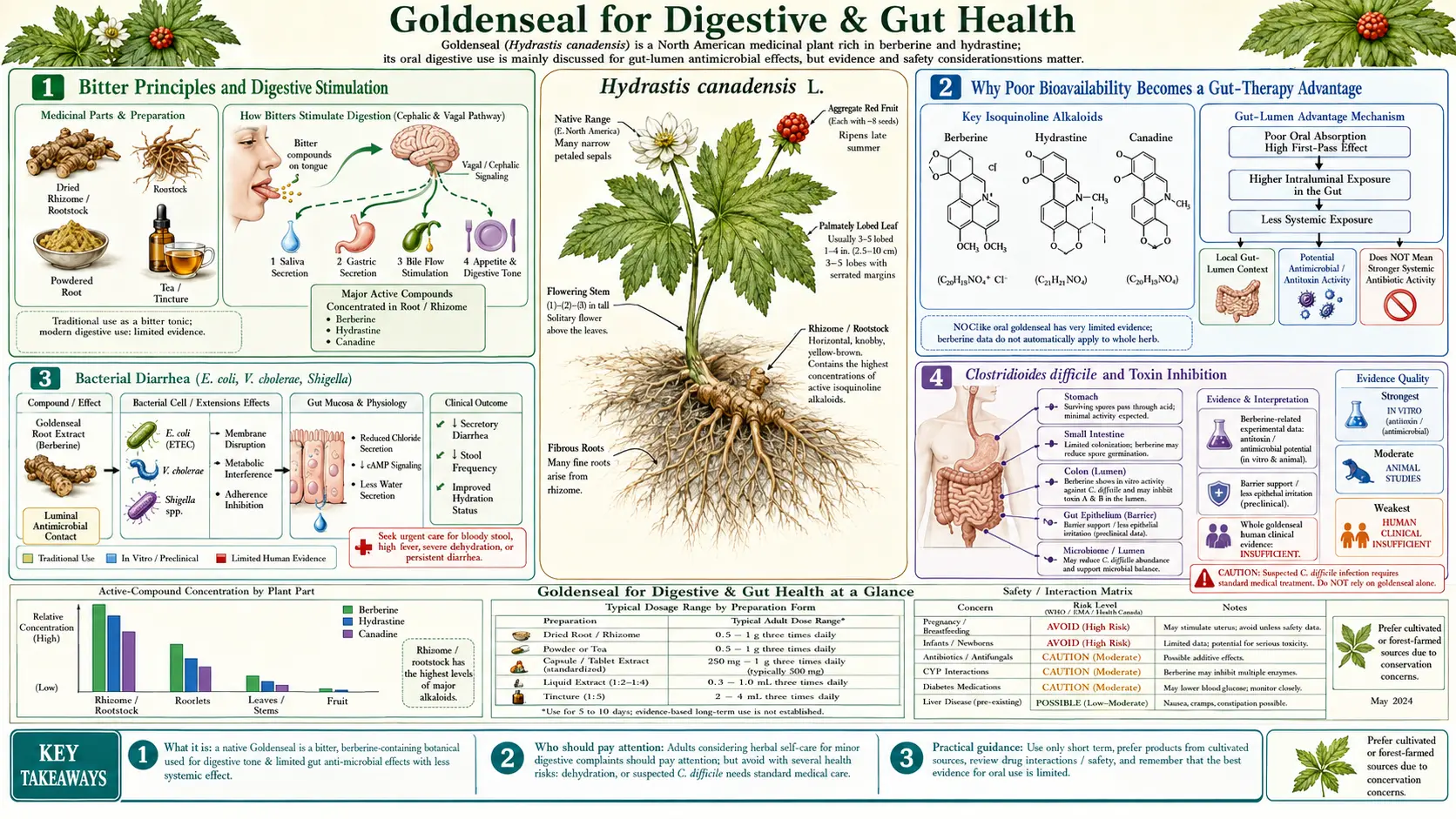
Bitter Principles and Digestive Stimulation
Goldenseal is one of the most powerful bitter herbs in the Western pharmacopeia. The bitter taste is generated almost entirely by the isoquinoline alkaloids, and the digestive-stimulating effects of bitters are mediated by a coordinated cascade beginning in the mouth and extending through the entire upper gastrointestinal tract.
When bitter compounds contact the bitter taste receptors (T2Rs) on the tongue, they trigger a vagal nerve reflex that increases:
- Salivary secretion — preparing the mouth and pharynx for swallowing, beginning starch digestion via salivary amylase
- Gastric acid (HCl) secretion — mediated by parietal cells, lowering gastric pH for optimal pepsin activity and protein digestion
- Pepsinogen secretion — the precursor that gastric acid activates into the protein-cleaving enzyme pepsin
- Bile flow (cholagogue effect) — gallbladder contraction releasing bile into the duodenum for fat emulsification
- Pancreatic enzyme secretion — amylase, lipase, and protease release into the duodenum
- Intestinal motility — promoting forward peristalsis and reducing stagnation
The classical herbalist's description of goldenseal as a "bitter tonic" maps directly onto this cascade. For individuals with hypochlorhydria (low stomach acid), poor fat digestion (sluggish bile flow, bloating after fatty meals), or generally poor appetite, taking a small amount of bitter goldenseal tincture (10-20 drops in water) 15-30 minutes before meals can produce a measurable improvement in digestive function. The effect is so consistent across bitter herbs (gentian, dandelion root, artichoke leaf, wormwood) that the bitter-principle pharmacology is now standard in integrative gastroenterology.
For routine bitter-stimulation purposes, however, much cheaper and more sustainable bitter herbs are equally effective. Goldenseal's value as a "digestive bitter" is genuine but not unique — gentian root or dandelion root tincture deliver the same vagal-reflex digestive stimulation without any conservation cost.
Why Poor Bioavailability Becomes a Gut-Therapy Advantage
Berberine's systemic oral bioavailability is approximately 5% — one of the lowest of any therapeutically active phytochemical. In pharmaceutical drug development, this would normally be considered a fatal flaw. For gut applications, it is a therapeutic advantage.
The 95% of orally administered berberine that does not enter systemic circulation remains in the gastrointestinal lumen, where it is exposed to bacterial populations at concentrations far exceeding the minimum inhibitory concentrations (MICs) required for antibacterial effect. A standard 500 mg oral berberine dose can produce luminal berberine concentrations of 200-400 micrograms per milliliter in the small intestine and proximal colon — well above the 16-128 microgram-per-milliliter MICs documented for most clinically relevant Gram-positive and Gram-negative gut pathogens.
This is why the most clinically validated applications of berberine and goldenseal are in-gut antimicrobial effects:
- Bacterial diarrhea treatment (high luminal berberine kills enteric pathogens)
- SIBO (small intestinal bacterial overgrowth) eradication
- H. pylori adjunct therapy (luminal berberine reaches the gastric mucosa)
- C. difficile infection (luminal berberine reaches colonic C. difficile and inhibits toxin production)
- Traveler's diarrhea prophylaxis
The contrast with systemic antibiotic-style applications is striking. For a systemic infection (e.g. pneumonia, sepsis, MRSA bacteremia), oral berberine simply cannot reach therapeutic systemic concentrations — the in vitro MICs against MRSA are unreachable through oral dosing alone. Topical or intravenous administration would be required, neither of which is standard for berberine.
The practical implication is that goldenseal's most defensible and best-evidenced clinical indications are concentrated in the gastrointestinal tract. This is also true for the sustainable berberine alternatives — Oregon grape root, barberry, Chinese goldthread, and purified berberine HCl all share the same poor systemic bioavailability + high luminal exposure pharmacokinetic profile.
Bacterial Diarrhea (E. coli, V. cholerae, Shigella)
The most extensively studied digestive application of berberine is the treatment of acute infectious diarrhea. The landmark clinical trial is Rabbani and colleagues' 1987 study published in the Journal of Infectious Diseases, in which 165 adults with diarrhea caused by enterotoxigenic E. coli (ETEC) or Vibrio cholerae were randomized to berberine sulphate (400 mg single dose) or placebo. Results:
- For ETEC diarrhea: stool volume reduced by approximately 45% in the first 24 hours in the berberine arm
- For cholera: stool volume reduced by approximately 30%, with the additional effect of decreased stool vibrio counts (direct antibacterial effect, not just symptom modulation)
- Safety: well tolerated, no serious adverse events
Multiple subsequent trials and a meta-analysis published in Phytomedicine have confirmed berberine's significant reduction in duration and stool volume for acute infectious diarrhea caused by E. coli, V. cholerae, and Shigella species. The effect is consistent enough that some integrative travel-medicine protocols recommend prophylactic berberine for travelers to areas with high traveler's-diarrhea incidence.
The mechanism is dual: direct bactericidal/bacteriostatic effect on the enteric pathogens at the high luminal berberine concentrations achieved, plus inhibition of the bacterial-enterotoxin-driven intestinal fluid secretion that produces the diarrhea (discussed in detail below).
For acute infectious diarrhea, the practical decision usually favors purified berberine HCl over goldenseal, on cost and sustainability grounds. A typical regimen is 500 mg of berberine HCl every 6 hours for the duration of acute symptoms (typically 2-5 days), tapering as symptoms resolve.
Clostridioides difficile and Toxin Inhibition
Clostridioides difficile (formerly Clostridium difficile) infection is one of the leading causes of hospital-acquired diarrhea and a major contributor to antibiotic-associated colitis. The clinical syndrome ranges from mild diarrhea to fulminant pseudomembranous colitis with toxic megacolon. The disease-causing agents are two large clostridial toxins: toxin A (enterotoxin) and toxin B (cytotoxin), which together produce the mucosal inflammation, epithelial necrosis, and fluid secretion that characterize the colitis.
Berberine's relevance to C. difficile infection extends beyond direct antibacterial activity (MIC 16-64 micrograms per milliliter against clinical isolates). Research published in the Journal of Medical Microbiology demonstrated that berberine at sub-MIC concentrations — concentrations too low to kill C. difficile — reduces toxin A production by approximately 70% and toxin B production by approximately 60%. This toxin-inhibitory effect is mechanistically distinct from direct killing and may be at least as clinically important.
The clinical relevance is concentrated in two contexts:
- Recurrent C. difficile infection — approximately 20% of patients treated for primary C. difficile infection develop a recurrence within 8 weeks, and risk of further recurrence rises with each episode. Berberine has been studied as an adjunct to standard therapy (vancomycin, fidaxomicin) for recurrence prevention, with several small studies showing reduced recurrence rates.
- Adjunct during active C. difficile treatment — some integrative practitioners add berberine to standard vancomycin protocols to provide additional toxin reduction during the period when host inflammation and mucosal damage are at peak severity.
For these indications, the clinical evidence base is suggestive but limited. The 2017 American College of Gastroenterology guidelines for C. difficile infection do not include berberine as a recommended therapy — the indication remains within the integrative-medicine adjunct category rather than standard-of-care. Patients with C. difficile infection should be under physician care; berberine is an adjunct, not a replacement, for evidence-based treatment.
SIBO and the Johns Hopkins Trial
Small intestinal bacterial overgrowth (SIBO) is a condition in which excessive bacterial colonization of the small bowel produces bloating, abdominal pain, diarrhea or constipation, malabsorption, and a constellation of nutritional deficiencies. SIBO is increasingly recognized as a common contributor to irritable bowel syndrome, unexplained chronic GI symptoms, and post-infectious diarrhea.
The standard-of-care SIBO treatment is the non-absorbed antibiotic rifaximin (550 mg three times daily for 14 days), often combined with neomycin for methane-predominant subtypes. Rifaximin is highly effective but expensive (approximately $1500-2000 per 14-day course in the United States without insurance), often not covered by insurance for SIBO indication, and frequently requires repeated courses for SIBO that recurs.
The landmark study comparing herbal antimicrobial therapy to rifaximin for SIBO was published in 2014 by Chedid and colleagues at Johns Hopkins, in Global Advances in Health and Medicine. The retrospective study examined 165 SIBO patients (confirmed by lactulose breath testing) treated either with rifaximin (the standard) or with one of two herbal antimicrobial regimens (each containing berberine-rich botanicals as core components). Results:
- Rifaximin response rate: 34% (negative follow-up breath test)
- Herbal antimicrobial response rate: 46% (negative follow-up breath test)
- Herbal antimicrobial response in rifaximin non-responders: 57% (those who had failed rifaximin first)
- Safety: comparable adverse event rates between rifaximin and herbal groups
The herbal protocols studied contained berberine-rich botanicals (goldenseal, Oregon grape, or barberry) alongside other antimicrobials including oregano oil, garlic extract, and red thyme oil. The berberine component is widely understood to be the most therapeutically active single constituent.
The implications for clinical SIBO management are significant: a properly formulated herbal antimicrobial protocol with berberine as a core component appears to be at least as effective as rifaximin, at a fraction of the cost. The Chedid trial has been cited extensively in integrative gastroenterology literature and is now part of standard naturopathic SIBO management protocols. Herbal antimicrobial protocols for SIBO typically use berberine HCl at 500 mg three times daily as the core, often combined with oregano oil and other supporting antimicrobials, for 4-8 weeks.
For SIBO specifically, the practical case for goldenseal vs alternatives is again resolved in favor of the more sustainable berberine sources. The Chedid protocols included goldenseal alongside the alternatives; modern integrative gastroenterologists more typically use purified berberine HCl or Oregon grape extract on cost and sustainability grounds.
Helicobacter pylori and Peptic Ulcer Adjunct
Helicobacter pylori is the bacterium responsible for the majority of peptic ulcers and a recognized risk factor for gastric adenocarcinoma. Standard treatment is "triple therapy" (proton pump inhibitor + amoxicillin + clarithromycin) for 14 days, with quadruple therapies (adding bismuth or metronidazole) used in regions with high clarithromycin resistance. Eradication rates with standard triple therapy have declined to approximately 70-75% in many regions due to growing antibiotic resistance.
Berberine has been studied as an adjunct to standard H. pylori eradication regimens. Research published in the World Journal of Gastroenterology demonstrated several relevant activities:
- Direct antibacterial activity against H. pylori at MIC 25-100 micrograms per milliliter
- Inhibition of H. pylori urease, the enzyme that H. pylori uses to neutralize gastric acid in its immediate microenvironment by generating ammonia from urea. Without urease, H. pylori cannot survive in the gastric lumen.
- Inhibition of H. pylori motility at sub-inhibitory concentrations, reducing the bacterium's ability to colonize new mucosal sites
- Synergistic activity with clarithromycin and amoxicillin against clinical isolates of H. pylori, including some clarithromycin-resistant strains
The clinical translation has been studied in several small randomized trials, generally showing modest improvements in eradication rate when berberine is added to standard triple therapy (typical improvements of 5-15 percentage points), and improvements in symptom resolution speed. The evidence is suggestive rather than definitive, and berberine has not entered standard H. pylori eradication guidelines, but it remains a reasonable adjunct in patients with prior eradication failure or in regions with high antibiotic resistance.
Typical adjunct dosing: berberine HCl 500 mg three times daily, combined with standard triple therapy for 14 days. As always, purified berberine HCl is preferred over goldenseal for this indication on sustainability grounds.
Direct Inhibition of Enterotoxin-Driven Cl− Secretion
One of berberine's most elegant mechanisms in infectious diarrhea is a direct effect on the intestinal epithelium independent of its antibacterial activity. Many of the most clinically significant diarrhea-causing organisms — Vibrio cholerae, enterotoxigenic E. coli, certain Shigella species — produce enterotoxins that activate cAMP-dependent signaling in intestinal epithelial cells, opening apical chloride channels (CFTR) and producing massive secretion of Cl− (and water following osmotically) into the gut lumen. This is the molecular mechanism of cholera and ETEC diarrhea: the secretory volume can reach 1 liter per hour in severe cholera.
Berberine has been shown to directly block the cAMP-activated chloride secretion pathway in intestinal epithelial cells. Studies using Ussing chamber preparations of small intestine epithelium demonstrate that berberine inhibits cholera-toxin-induced and ETEC-heat-labile-toxin-induced Cl− secretion in a dose-dependent manner. This effect is independent of berberine's antibacterial activity — it would reduce diarrheal fluid loss even in a treated infection where the bacteria have been killed but the secreted toxins continue to drive epithelial fluid loss.
The clinical implications:
- Berberine's effect on cholera and ETEC diarrhea is more rapid than would be expected from antibacterial action alone — symptom improvement begins within hours rather than the days required for antibacterial bacterial reduction
- The dual mechanism (direct antibacterial + Cl− channel inhibition) explains why berberine reduces stool volume even more than it reduces stool bacterial counts in cholera
- The Cl− channel inhibition is potentially clinically valuable as an adjunct to oral rehydration therapy in low-resource settings where access to antibiotics is limited
The same Cl− channel inhibition is responsible for some of the constipation that can occur as a side effect of long-term berberine use in adults without diarrhea — the channel inhibition reduces normal baseline fluid secretion into the gut.
Inflammatory Bowel Disease Adjunct Pilot Data
The application of berberine and goldenseal to Crohn's disease and ulcerative colitis is an area of active research with a small but growing pilot evidence base. The theoretical case is compelling: berberine has documented anti-inflammatory effects (NF-kB pathway inhibition, reduction of TNF-alpha and IL-6), intestinal barrier-restorative effects (upregulation of tight junction proteins claudin and occludin), and potential immune-modulating effects (Th17/Treg balance modulation).
Several small clinical trials have explored berberine in IBD:
- Ulcerative colitis in remission — a 2020 Chinese trial randomized 109 patients in ulcerative colitis remission to berberine 300 mg three times daily or placebo for 12 months. The berberine group showed a relapse rate of 36% vs 59% in the placebo group (significant), with reduced markers of mucosal inflammation.
- Crohn's disease — smaller pilot data with similar trends, particularly for postoperative recurrence prevention. The mechanistic plausibility is high but definitive randomized data are still limited.
- Microscopic colitis — case series suggest benefit, with the proposed mechanism being a combination of direct anti-inflammatory effect and barrier restoration
For IBD specifically, the practical recommendation is that berberine should be considered an adjunct to (not a replacement for) standard immunosuppressive or biologic therapy. The cytochrome P450 drug interactions are particularly relevant in IBD where patients may be on biologics, immunosuppressants, or anti-inflammatory drugs metabolized through the affected enzymes. Always discuss with a treating gastroenterologist before adding berberine to an IBD regimen.
Intestinal Barrier and Microbiome Effects
Beyond direct antimicrobial and anti-inflammatory effects, berberine has documented effects on the intestinal barrier and on overall gut microbiota composition that may be relevant for conditions involving "leaky gut" / increased intestinal permeability.
Tight junction protein expression: Berberine increases the expression of intestinal tight junction proteins including claudin-1, claudin-5, occludin, and zonula occludens-1 (ZO-1). These proteins form the molecular seal between adjacent intestinal epithelial cells and are the primary determinant of intestinal barrier permeability. Berberine's tight-junction-restorative effect has been documented in animal models of inflammatory bowel disease, diet-induced obesity, and chronic alcohol exposure.
Microbiota modulation: Berberine produces relatively consistent and well-characterized shifts in gut microbiota composition. In multiple animal and human studies, berberine increases the relative abundance of Akkermansia muciniphila (associated with metabolic health and intestinal barrier integrity), Bacteroides species (generally beneficial), and reduces the abundance of Clostridium species and some Firmicutes. The net effect on overall microbial diversity is variable across studies, but the general direction is toward what is sometimes called a "leaner" microbiota profile.
Implications for "leaky gut" syndromes: Conditions that are increasingly characterized by increased intestinal permeability — including IBS, autoimmune diseases, food sensitivities, and chronic fatigue syndrome — may benefit from berberine's combined barrier-restorative and microbiota-modulating effects. The clinical evidence in these conditions is preliminary but mechanistically plausible.
The practical caveat is that berberine's broad antimicrobial action will also kill commensal bacteria, not just pathogens. Extended berberine use (more than 3-4 weeks continuously) without microbiota-restorative support (a high-fiber diet, fermented foods, and possibly a brief course of probiotics) may produce dysbiosis. Standard cycling protocols (2-4 weeks on, 1-2 weeks off) help mitigate this risk.
Comparison to Barberry, Oregon Grape, and Pure Berberine HCl
For gut applications specifically, the case for using goldenseal over its more sustainable alternatives is exceptionally weak. Here is the side-by-side comparison:
- Goldenseal (Hydrastis canadensis): Berberine 2.5-6% + hydrastine + canadine. Conservation status: CITES Appendix II, United Plant Savers "At-Risk." Cost: $40-80 per ounce of root powder.
- Oregon grape root (Mahonia aquifolium): Berberine 2-3% + berbamine + oxyacanthine + other supporting alkaloids. Conservation status: abundant, not threatened. Cost: $10-20 per ounce of root powder.
- Barberry (Berberis vulgaris): Berberine 1.5-3% + berbamine + palmatine + jatrorrhizine. Conservation status: abundant; the European barberry is also widespread as an invasive species in parts of North America. Cost: $10-20 per ounce.
- Chinese goldthread (Coptis chinensis): Berberine 5-8% (the highest natural concentration) + palmatine + coptisine. Conservation status: cultivated extensively in China; the wild Chinese populations are themselves under pressure but commercial supply is from cultivation. Cost: variable.
- Purified berberine HCl (capsules): Berberine 99%+ purity, typically 500 mg per capsule. Conservation status: synthesized or extracted from cultivated Chinese goldthread / barberry. Cost: $0.10-0.30 per 500 mg dose, $10-30 per bottle of 60-120 capsules. The most economical and most precisely dosed option.
For nearly all gut applications — SIBO eradication, bacterial diarrhea, H. pylori adjunct, traveler's diarrhea prophylaxis, blood sugar management, IBD adjunct — purified berberine HCl is the practical first choice. It is the most reliably dosed, the cheapest per effective dose, and free of the sustainability concerns that attach to goldenseal.
The narrow case for using goldenseal whole-root over berberine HCl in gut applications would be a clinical context where the hydrastine-mediated mucous-membrane astringency adds meaningful value (severe mucousy diarrhea with significant epithelial inflammation, perhaps). For most clinical scenarios, this is a marginal advantage that does not justify the conservation cost.
Practical Dosing for Gut Applications
For purified berberine HCl (the preferred first choice for most gut indications):
- SIBO: 500 mg three times daily with meals, for 4-8 weeks. Often combined with oregano oil (200 mg three times daily) and other supporting antimicrobials in herbal SIBO protocols.
- Acute bacterial diarrhea: 500 mg every 6 hours for the duration of acute symptoms (2-5 days), tapering as resolution occurs.
- Traveler's diarrhea prophylaxis: 500 mg twice daily, starting 1-2 days before travel through 1-2 days after return.
- H. pylori adjunct: 500 mg three times daily, combined with standard triple therapy for 14 days.
- C. difficile adjunct: 500 mg three times daily, alongside standard vancomycin or fidaxomicin therapy. Continue 2-4 weeks after standard therapy to reduce recurrence risk.
- IBD adjunct: 300-500 mg three times daily, ongoing, alongside standard immunomodulating therapy (with the cautions about drug interactions noted below).
- Blood sugar / metabolic indications: 500 mg two to three times daily with meals.
For goldenseal (when chosen for a specific clinical reason that warrants the alkaloid profile):
- Tincture (1:5, 60% ethanol): 2-4 mL three times daily before meals. For digestive bitter effect, 10-20 drops in water 15-30 minutes before meals.
- Standardized extract (5% berberine): 250-500 mg three times daily with meals.
- Root powder: 500-1000 mg three times daily.
- Duration: 7-21 days for acute use, with practitioner supervision for anything longer.
- Cycling: 2-3 weeks on, 1-2 weeks off, for any extended use, to preserve microbiota diversity and prevent mucous membrane over-drying.
Take all berberine-containing supplements with food to slow absorption and maximize gut exposure. Avoid combining with food items that significantly raise gastric pH (which can reduce berberine ionization and altering both luminal and systemic kinetics).
Cautions and Drug Interactions
- Pregnancy and breastfeeding — strictly contraindicated. Berberine stimulates uterine contractions, crosses the placenta, and displaces bilirubin from albumin (kernicterus risk in the neonate).
- CYP450 drug interactions — berberine is a potent inhibitor of CYP3A4, CYP2D6, and CYP2C9. Major interactions with: warfarin, statins, calcium channel blockers, cyclosporine, tacrolimus, SSRIs/SNRIs, several antiretrovirals, and many other drugs. Consult a knowledgeable prescriber before adding berberine to any prescription regimen.
- P-glycoprotein inhibition — berberine inhibits the P-gp drug efflux transporter, increasing absorption of P-gp substrates including digoxin, several chemotherapeutic agents, and some immunosuppressants.
- Hypoglycemia — berberine significantly lowers blood glucose. Patients on insulin, sulfonylureas, or other hypoglycemic medications may experience additive hypoglycemia. Monitor blood glucose closely when adding berberine to a diabetic regimen.
- Gut microbiota disruption with long-term use — berberine kills commensals as well as pathogens. Use cycling protocols (2-4 weeks on, 1-2 weeks off) and consider concurrent probiotic and prebiotic support to mitigate dysbiosis risk.
- Constipation — the same Cl− channel inhibition that benefits diarrheal disease can produce constipation in patients with baseline normal or slow transit. Reduce dose or discontinue if constipation develops.
- Neonates and young infants — never administer.
- Sustainability ethics — see the Sustainability deep dive. For gut applications, purified berberine HCl or Oregon grape are strongly preferred over goldenseal.
Key Research Papers
- Rabbani GH et al. (1987). Randomised controlled trial of berberine sulphate therapy for diarrhoea due to enterotoxigenic E. coli and V. cholerae. J Infect Dis. — PubMed
- Chedid V et al. (2014). Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global Advances in Health and Medicine. — PubMed
- Berberine inhibition of C. difficile toxin A and toxin B production — PubMed
- Berberine and H. pylori urease inhibition (World J Gastroenterol) — PubMed
- Berberine inhibition of cholera toxin-induced Cl− secretion — PubMed
- Berberine inhibition of heat-labile enterotoxin (LT) signaling — PubMed
- Berberine in ulcerative colitis remission maintenance trial — PubMed
- Berberine and intestinal tight junction protein expression — PubMed
- Berberine and Akkermansia muciniphila abundance — PubMed
- Habtemariam S. The therapeutic potential of berberine in treatment of gastrointestinal infections. Current Medicinal Chemistry. — PubMed
- Bitter principles, T2R bitter receptors, and gastric/biliary secretion — PubMed
- Berberine vs metformin for type 2 diabetes (meta-analysis) — PubMed
PubMed Topic Searches
- PubMed: Berberine + SIBO
- PubMed: Berberine + infectious diarrhea
- PubMed: Berberine + H. pylori
- PubMed: Berberine + IBD
- PubMed: Berberine + gut microbiota
Connections
- Goldenseal Overview
- Goldenseal Benefits Hub
- Goldenseal Antimicrobial Action
- Goldenseal for Eye Health
- Sustainability & Cautions
- Berberine (Pure Supplement)
- Barberry (Sustainable Alternative)
- Berberine Remedy
- SIBO
- Herbal Antimicrobials for SIBO
- Irritable Bowel Syndrome
- Crohn's Disease
- Clostridium Difficile
- Escherichia Coli
- Helicobacter Pylori
- Gut Healing
- Oregano
- Garlic
- Immune Boosting
- All Herbs