Staphylococcus aureus — The Golden Staph
Symptoms & Infections
The full spectrum of staph infections — from pimples to life-threatening sepsis.
Skin Infections
Boils, abscesses, cellulitis, impetigo, and folliculitis — the most common staph presentations.
Invasive Disease & Sepsis
Bacteremia, endocarditis, pneumonia, osteomyelitis, and septic shock.
Diagnosis Tests
Blood cultures, wound cultures, sensitivity testing, and identifying MRSA.
Treatment & Prevention
How staph infections are treated — from topical mupirocin to IV vancomycin.
MRSA Treatment
Vancomycin, daptomycin, linezolid, and ceftaroline for resistant staph.
Decolonization & Control
Mupirocin nasal decolonization, chlorhexidine baths, and hospital infection control.
MRSA Drug Resistance
The mecA gene, beta-lactam resistance mechanisms, and the VRSA threat.
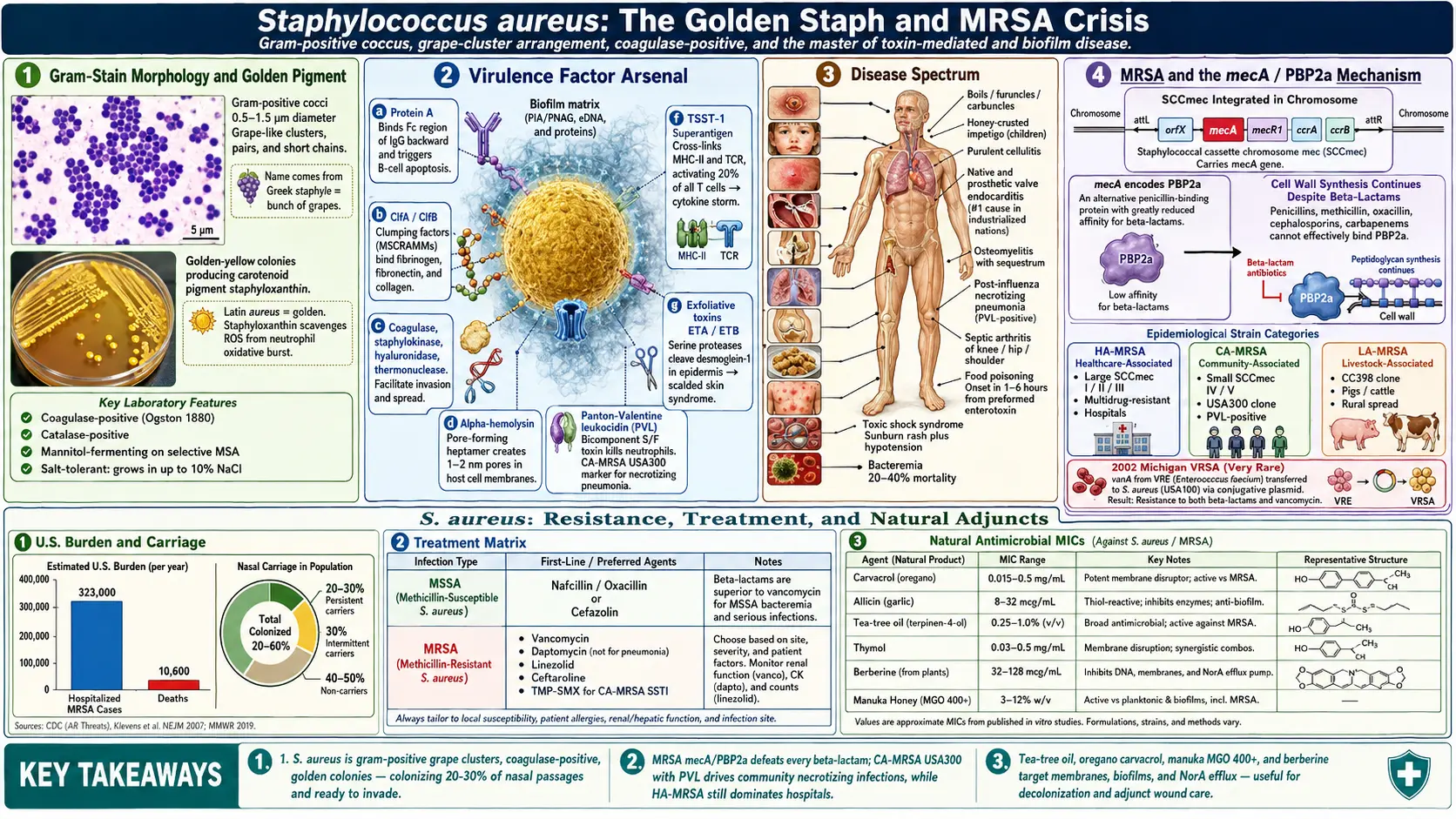
Table of Contents
- Discovery and Microbiology
- Virulence Factors and Pathogenesis
- Diseases Caused by S. aureus
- MRSA — Methicillin-Resistant Staphylococcus aureus
- Conventional Antibiotic Treatment
- Natural Antibacterial Herbs Effective Against S. aureus
- Research on Herbal Approaches to MRSA
- Biofilm Formation and Herbal Disruption
- Prevention and Hygiene
- Key Research Papers
- Featured Videos
1. Discovery and Microbiology
Staphylococcus aureus was first identified in 1880 by the Scottish surgeon Sir Alexander Ogston, who observed the bacterium in pus drained from surgical abscesses at Aberdeen Royal Infirmary. Ogston named the organism after the Greek word staphyle (bunch of grapes), reflecting the characteristic grape-like clusters he observed under the microscope. The species name aureus (Latin for "golden") was later assigned by Friedrich Julius Rosenbach in 1884, who distinguished it from the white-pigmented Staphylococcus albus (now S. epidermidis) based on colony color.
S. aureus is a Gram-positive coccus, approximately 0.5 to 1.5 micrometers in diameter. Under Gram staining, the cells appear as dark purple spheres arranged in irregular grape-like clusters, though pairs and short chains can also occur. The organism is non-motile, non-spore-forming, and facultatively anaerobic, meaning it can grow in both the presence and absence of oxygen.
A hallmark feature of S. aureus is its production of the carotenoid pigment staphyloxanthin, which gives colonies their distinctive golden-yellow color on nutrient agar. Staphyloxanthin is far more than a cosmetic trait — it functions as a virulence factor by scavenging reactive oxygen species produced by the host immune system during the oxidative burst of neutrophils. Studies have demonstrated that mutant strains lacking staphyloxanthin are significantly more susceptible to killing by human neutrophils and show reduced virulence in animal infection models.
S. aureus is distinguished from other staphylococci by its production of the enzyme coagulase, which converts fibrinogen to fibrin, causing blood plasma to clot. The coagulase test remains a key diagnostic tool in clinical microbiology laboratories. The organism is also catalase-positive (distinguishing it from streptococci), salt-tolerant (growing in up to 10% NaCl), and capable of fermenting mannitol — properties exploited in selective media such as mannitol salt agar.
Approximately 20 to 30 percent of the human population are persistent nasal carriers of S. aureus, while an additional 30 percent carry the organism intermittently. The anterior nares are the primary colonization site, though the skin, perineum, pharynx, and gastrointestinal tract also serve as reservoirs. Carriage is generally asymptomatic but significantly increases the risk of subsequent infection, particularly in surgical patients, dialysis patients, and those with indwelling medical devices.
2. Virulence Factors and Pathogenesis
S. aureus possesses an extraordinary arsenal of virulence factors that enable it to adhere to host tissues, evade the immune system, damage cells and tissues, and disseminate throughout the body. This versatility explains why S. aureus causes such a wide range of diseases, from minor skin infections to life-threatening systemic conditions.
Surface Proteins and Immune Evasion
Protein A is anchored to the cell wall and binds the Fc region of immunoglobulin G (IgG) antibodies in the wrong orientation, effectively coating the bacterium in a layer of non-functional antibodies. This prevents opsonization and phagocytosis, allowing the bacterium to evade complement-mediated killing and neutrophil engulfment. Protein A also triggers B-cell apoptosis, further undermining the adaptive immune response.
Clumping factor A and B (ClfA/ClfB) and other MSCRAMMs (microbial surface components recognizing adhesive matrix molecules) mediate binding to fibrinogen, fibronectin, collagen, and other extracellular matrix proteins. These adhesins are critical for the initial colonization of host tissues and for attachment to implanted medical devices coated with host proteins.
Enzymes
Coagulase (both free coagulase and bound clumping factor) activates prothrombin, converting fibrinogen to fibrin. The resulting fibrin clot surrounds the bacteria, shielding them from phagocytes. Staphylokinase performs the opposite function, dissolving fibrin clots to facilitate bacterial dissemination once an abscess matures. Hyaluronidase degrades hyaluronic acid in connective tissue, promoting the spread of infection through tissues. Lipases break down lipids in the skin, aiding colonization of sebaceous areas. DNase (thermonuclease) degrades neutrophil extracellular traps (NETs), a recently discovered immune defense mechanism.
Toxins
S. aureus produces a formidable array of toxins:
- Alpha-hemolysin (alpha-toxin): A pore-forming toxin that inserts into host cell membranes, creating heptameric barrel-shaped pores approximately 1-2 nm in diameter. It destroys a wide range of host cells including erythrocytes, epithelial cells, endothelial cells, monocytes, and lymphocytes. Alpha-toxin is considered one of the most important virulence factors in skin and soft tissue infections and pneumonia.
- Beta-hemolysin: A sphingomyelinase that degrades sphingomyelin in cell membranes, causing lysis of erythrocytes and other cell types. Its activity is enhanced at low temperatures (the "hot-cold" lysis phenomenon).
- Gamma-hemolysin: A bicomponent pore-forming toxin composed of S and F subunits that assemble on target cell membranes to form octameric pores. It targets neutrophils, monocytes, macrophages, and erythrocytes.
- Delta-hemolysin (delta-toxin): A small amphipathic peptide that disrupts membranes in a detergent-like manner. It also functions as a phenol-soluble modulin (PSM) and activates mast cells, contributing to allergic and inflammatory responses.
- Panton-Valentine leukocidin (PVL): A bicomponent pore-forming toxin encoded by phage-borne genes lukS-PV and lukF-PV. PVL specifically targets and destroys neutrophils and macrophages. It is strongly associated with community-acquired MRSA (CA-MRSA) strains and is a marker for severe necrotizing skin infections and necrotizing pneumonia, particularly in young, otherwise healthy individuals.
- Toxic shock syndrome toxin-1 (TSST-1): A superantigen that cross-links MHC class II molecules on antigen-presenting cells with T-cell receptors in a non-specific manner, activating up to 20 percent of the entire T-cell population simultaneously. This triggers a massive cytokine storm (IL-1, IL-2, TNF-alpha, IFN-gamma) resulting in fever, hypotension, multi-organ failure, and the characteristic desquamating rash of toxic shock syndrome.
- Staphylococcal enterotoxins (SEA through SEE, SEG through SEQ): Heat-stable superantigens that cause staphylococcal food poisoning when ingested. They are resistant to degradation by gastrointestinal proteases and survive boiling, meaning that food contaminated with preformed enterotoxin remains toxic even after thorough cooking.
- Exfoliative toxins (ETA and ETB): Serine proteases that specifically cleave desmoglein-1, a desmosomal adhesion molecule in the granular layer of the epidermis, causing the widespread blistering and skin separation characteristic of staphylococcal scalded skin syndrome.
Biofilm Formation
S. aureus readily forms biofilms on both biotic surfaces (damaged tissue, heart valves) and abiotic surfaces (catheters, prosthetic joints, implants). Biofilm formation proceeds through attachment, accumulation, maturation, and dispersal phases. The biofilm matrix consists of polysaccharide intercellular adhesin (PIA/PNAG), extracellular DNA (eDNA), and proteins. Bacteria within biofilms are up to 1,000-fold more resistant to antibiotics and are largely protected from host immune defenses, making biofilm-associated infections exceptionally difficult to treat.
3. Diseases Caused by S. aureus
S. aureus is one of the most versatile human pathogens, capable of infecting virtually every organ system. The spectrum of disease ranges from superficial skin infections to rapidly fatal systemic conditions.
Skin and Soft Tissue Infections
S. aureus is the leading cause of bacterial skin and soft tissue infections worldwide:
- Furuncles (boils): Deep infections of hair follicles presenting as painful, erythematous, pus-filled nodules. Multiple coalescing furuncles form a carbuncle, which involves subcutaneous tissue and may be accompanied by systemic symptoms.
- Impetigo: A highly contagious superficial skin infection characterized by honey-colored crusted lesions, most common in children. Bullous impetigo, caused by exfoliative toxin-producing strains, presents with large fluid-filled blisters.
- Cellulitis: A spreading infection of the skin and subcutaneous tissues presenting as an expanding area of erythema, warmth, swelling, and pain. Purulent cellulitis with abscess formation is strongly associated with S. aureus, particularly CA-MRSA strains.
- Wound infections: S. aureus is the most common pathogen in surgical site infections and traumatic wound infections, readily colonizing devitalized tissue and foreign material.
Invasive and Systemic Infections
- Bacteremia and sepsis: S. aureus bacteremia carries a mortality rate of 20 to 40 percent even with appropriate antibiotic therapy. The organism has a propensity for metastatic seeding, and patients with S. aureus bacteremia must be evaluated for secondary foci of infection including endocarditis, osteomyelitis, and septic arthritis.
- Infective endocarditis: S. aureus is the leading cause of infective endocarditis in industrialized nations, affecting both native and prosthetic heart valves. Acute S. aureus endocarditis is a fulminant disease with large, destructive vegetations, valvular perforation, paravalvular abscesses, and a high rate of embolic complications including stroke, splenic infarcts, and mycotic aneurysms.
- Osteomyelitis: S. aureus is the most common cause of both acute hematogenous osteomyelitis (predominantly in children) and chronic osteomyelitis. The organism invades osteoblasts, forms biofilm on bone surfaces, and creates sequestra (fragments of dead bone) that harbor bacteria and resist antibiotic penetration.
- Pneumonia: S. aureus pneumonia occurs as a primary community-acquired infection (often following influenza), hospital-acquired ventilator-associated pneumonia, or hematogenous pneumonia with septic pulmonary emboli. PVL-positive strains cause necrotizing pneumonia with rapid cavitation and high mortality.
- Septic arthritis: S. aureus is the most common cause of septic arthritis in adults, typically affecting large joints such as the knee, hip, and shoulder.
Toxin-Mediated Diseases
- Staphylococcal food poisoning: One of the most common causes of bacterial food poisoning worldwide, with onset of severe nausea, vomiting, abdominal cramps, and diarrhea within 1 to 6 hours of ingesting food contaminated with preformed enterotoxin. The illness is typically self-limited, resolving within 24 to 48 hours.
- Toxic shock syndrome (TSS): A life-threatening condition caused by TSST-1 or enterotoxin-mediated superantigen activity. It presents with sudden onset of high fever, diffuse erythroderma (sunburn-like rash), hypotension, and involvement of three or more organ systems. Originally associated with tampon use in menstruating women, non-menstrual TSS now accounts for the majority of cases and can complicate any staphylococcal infection.
- Staphylococcal scalded skin syndrome (SSSS): Caused by exfoliative toxins in neonates and young children, SSSS presents with widespread erythema, fragile blisters, and superficial desquamation giving the appearance of a scald burn. The exfoliative toxins circulate hematogenously, and the skin separation occurs at sites distant from the primary infection focus.
4. MRSA — Methicillin-Resistant Staphylococcus aureus
The emergence of methicillin-resistant Staphylococcus aureus (MRSA) represents one of the most significant challenges in modern infectious disease medicine. MRSA was first reported in the United Kingdom in 1961, only two years after methicillin was introduced as a penicillinase-resistant penicillin specifically designed to treat penicillin-resistant S. aureus.
Mechanism of Resistance
MRSA resistance is mediated by the mecA gene (or less commonly mecC), carried on a mobile genetic element called the staphylococcal cassette chromosome mec (SCCmec). The mecA gene encodes an alternative penicillin-binding protein, PBP2a (also called PBP2'), which has greatly reduced affinity for all beta-lactam antibiotics including penicillins, cephalosporins, and carbapenems. Because cell wall synthesis can proceed through PBP2a even in the presence of beta-lactams, MRSA is resistant to virtually the entire beta-lactam class — the most widely used family of antibiotics worldwide.
Epidemiological Categories
- Hospital-associated MRSA (HA-MRSA): The traditional form of MRSA, associated with healthcare settings including hospitals, nursing homes, and dialysis centers. HA-MRSA strains typically carry larger SCCmec elements (types I, II, or III) with additional resistance determinants, conferring multidrug resistance. Risk factors include prolonged hospitalization, surgery, indwelling devices, ICU admission, and prior antibiotic exposure.
- Community-associated MRSA (CA-MRSA): Emerged in the late 1990s as a cause of infections in otherwise healthy individuals without traditional healthcare risk factors. CA-MRSA strains typically carry smaller SCCmec elements (types IV or V), are often susceptible to non-beta-lactam antibiotics, and frequently harbor PVL genes. The USA300 clone became the dominant CA-MRSA strain in North America, causing epidemic waves of skin and soft tissue infections.
- Livestock-associated MRSA (LA-MRSA): First identified in Dutch pig farmers in 2005, LA-MRSA (predominantly CC398) colonizes livestock including pigs, cattle, and poultry, and can be transmitted to humans through direct animal contact or environmental exposure. LA-MRSA has become a significant concern in agricultural communities across Europe.
Prevalence and Impact
MRSA accounts for a substantial proportion of S. aureus infections globally. In the United States, the Centers for Disease Control and Prevention (CDC) estimated over 323,000 hospitalized MRSA cases and approximately 10,600 deaths annually. While invasive MRSA infections have declined since 2005 due to improved hospital infection control, community-associated MRSA infections remain common. MRSA prevalence varies geographically, with rates exceeding 50 percent of hospital S. aureus isolates in some countries while remaining below 5 percent in Scandinavian nations with stringent search-and-destroy policies.
VRSA Emergence
The emergence of vancomycin-resistant S. aureus (VRSA) represents the most alarming resistance development. VRSA strains acquire the vanA gene cluster from vancomycin-resistant enterococci (VRE) via conjugative transfer, enabling modification of the peptidoglycan target that vancomycin binds. Since the first VRSA isolate was identified in Michigan in 2002, only a small number of confirmed VRSA cases have been reported globally, but the potential for wider dissemination remains a critical public health concern.
5. Conventional Antibiotic Treatment
The treatment of S. aureus infections depends on the susceptibility profile of the infecting strain, the site and severity of infection, and patient-specific factors.
Treatment of MSSA (Methicillin-Susceptible) Infections
For methicillin-susceptible S. aureus (MSSA), anti-staphylococcal penicillins (nafcillin, oxacillin, flucloxacillin) and first-generation cephalosporins (cefazolin) remain the treatment of choice. These agents have superior efficacy compared to vancomycin for MSSA infections, with clinical studies demonstrating better outcomes and lower mortality with beta-lactam therapy.
Treatment of MRSA Infections
- Vancomycin: A glycopeptide antibiotic that has been the cornerstone of MRSA treatment for decades. Vancomycin inhibits cell wall synthesis by binding to the D-Ala-D-Ala terminus of peptidoglycan precursors. However, its use is complicated by nephrotoxicity, the need for therapeutic drug monitoring, slow bactericidal activity, and the emergence of vancomycin-intermediate S. aureus (VISA) strains with MICs of 4-8 mcg/mL due to thickened cell walls that trap vancomycin molecules.
- Daptomycin: A lipopeptide antibiotic that inserts into the bacterial cell membrane and causes rapid depolarization. It is approved for MRSA bacteremia, right-sided endocarditis, and skin and soft tissue infections. Daptomycin is inactivated by pulmonary surfactant and therefore cannot be used for pneumonia.
- Linezolid: An oxazolidinone that inhibits protein synthesis by binding to the 23S ribosomal RNA of the 50S ribosomal subunit. It has excellent oral bioavailability and tissue penetration, making it valuable for MRSA pneumonia and infections where intravenous access is limited. Long-term use is limited by myelosuppression, peripheral neuropathy, and serotonin syndrome risk.
- Trimethoprim-sulfamethoxazole (TMP-SMX): Widely used for uncomplicated CA-MRSA skin and soft tissue infections due to oral availability, low cost, and generally preserved susceptibility among community MRSA strains.
- Other agents: Ceftaroline (the only cephalosporin active against MRSA via binding to PBP2a), tedizolid, dalbavancin, oritavancin, and telavancin provide additional options for specific clinical scenarios.
Resistance Trends
Antibiotic resistance in S. aureus continues to evolve. Resistance to mupirocin (used for nasal decolonization), clindamycin (inducible resistance via the erm genes), fluoroquinolones, and fusidic acid is increasingly reported. The spread of multidrug-resistant HA-MRSA clones and the emergence of daptomycin non-susceptibility and linezolid resistance further narrow therapeutic options, underscoring the urgent need for new antibacterial strategies.
6. Natural Antibacterial Herbs Effective Against S. aureus
A growing body of peer-reviewed research has demonstrated that numerous plant-derived compounds possess significant antibacterial activity against S. aureus, including antibiotic-resistant strains. The following herbs have the strongest evidence base for anti-staphylococcal activity.
Oregano (Origanum vulgare)
Oregano essential oil and its primary phenolic compound carvacrol demonstrate potent antibacterial activity against S. aureus. Carvacrol disrupts the bacterial cell membrane by integrating into the phospholipid bilayer, increasing membrane permeability, and causing leakage of intracellular contents including ions, ATP, and nucleic acids. Published minimum inhibitory concentration (MIC) values for carvacrol against S. aureus range from 0.015 to 0.5 mg/mL depending on the strain and methodology. Oregano oil has also demonstrated activity against MRSA strains, with MIC values typically in the range of 0.06 to 0.5% (v/v). The related compound thymol, also found in oregano, acts synergistically with carvacrol.
Garlic (Allium sativum)
Garlic contains the organosulfur compound allicin (diallyl thiosulfinate), produced when the enzyme alliinase converts alliin upon crushing or chopping of fresh garlic cloves. Allicin exhibits broad-spectrum antibacterial activity by reacting with thiol groups in essential enzymes, particularly those involved in RNA synthesis, lipid biosynthesis, and acetyl-CoA formation. MIC values for allicin against S. aureus have been reported as 8 to 32 mcg/mL. Ajoene, another garlic-derived compound, inhibits quorum sensing in S. aureus and has shown synergy with conventional antibiotics including tobramycin. Fresh garlic extract has demonstrated activity against both MSSA and MRSA in multiple in vitro studies.
Tea Tree (Melaleuca alternifolia)
Tea tree oil is one of the most extensively studied essential oils for anti-staphylococcal activity. Its primary active component, terpinen-4-ol, disrupts bacterial membrane integrity and inhibits respiration. Tea tree oil has demonstrated consistent activity against S. aureus with MIC values typically between 0.25 and 1.0% (v/v), and importantly, it retains activity against MRSA strains at similar concentrations. Clinical studies have evaluated tea tree oil for nasal decolonization of MRSA carriers, topical treatment of MRSA wound infections, and as a component of hospital-based decolonization protocols. Tea tree oil also demonstrates activity against S. aureus biofilms at concentrations at or near the planktonic MIC.
Goldenseal (Hydrastis canadensis)
Goldenseal root contains the isoquinoline alkaloid berberine, which exhibits antibacterial activity through multiple mechanisms including inhibition of the bacterial enzyme FtsZ (essential for cell division), disruption of cell membrane function, and inhibition of DNA and protein synthesis. MIC values for berberine against S. aureus range from 32 to 128 mcg/mL for susceptible strains. While these MIC values are relatively high compared to conventional antibiotics, berberine has attracted significant research interest for its ability to inhibit bacterial efflux pumps, particularly the NorA multidrug efflux pump in S. aureus. By blocking NorA, berberine can restore the susceptibility of resistant strains to multiple antibiotics, functioning as a resistance-modifying agent.
Thyme (Thymus vulgaris)
Thyme essential oil contains thymol as its principal antibacterial compound. Thymol shares a structural similarity with carvacrol (they are positional isomers) and acts by a similar membrane-disrupting mechanism. Thymol integrates into the lipid bilayer at the polar headgroup region, causing increased membrane fluidity, leakage of potassium ions and ATP, and ultimately cell death. MIC values for thymol against S. aureus are typically 0.03 to 0.5 mg/mL. Thyme oil has demonstrated synergistic activity when combined with antibiotics such as penicillin and tetracycline against S. aureus, reducing the required antibiotic concentration by 4 to 16-fold in checkerboard assays.
Manuka Honey (Leptospermum scoparium)
Manuka honey possesses unique non-peroxide antibacterial activity attributed primarily to methylglyoxal (MGO), a reactive carbonyl compound derived from the conversion of dihydroxyacetone present in the nectar of the manuka bush. Medical-grade manuka honey with high Unique Manuka Factor (UMF) ratings (UMF 12.5+ or MGO 400+) has demonstrated consistent bactericidal activity against S. aureus including MRSA, with MIC values of 3 to 12% (w/v) depending on the MGO concentration and test strain. Beyond direct bactericidal activity, manuka honey disrupts S. aureus biofilms, prevents bacterial adhesion to wound surfaces, maintains a moist wound environment conducive to healing, and modulates the local immune response. Medical-grade manuka honey dressings (Medihoney, Manukamed) have received FDA clearance for wound management.
7. Research on Herbal Approaches to MRSA
The increasing prevalence of MRSA and the dwindling pipeline of new antibiotics have intensified research into plant-derived antimicrobials as potential alternative or adjunctive therapies. Several lines of investigation have yielded promising results.
Oregano Oil Against MRSA
Multiple in vitro studies have demonstrated that oregano essential oil and purified carvacrol retain full activity against MRSA strains, with MIC values comparable to those against susceptible S. aureus. This is because carvacrol's mechanism of action — direct membrane disruption — bypasses the PBP2a-mediated resistance mechanism. A study published in the Journal of Applied Microbiology showed that carvacrol at sub-MIC concentrations enhanced the activity of oxacillin against MRSA, reducing the oxacillin MIC by 4 to 8-fold, suggesting potential for combination therapy. Carvacrol has also been shown to reduce S. aureus virulence gene expression, including genes encoding alpha-toxin, enterotoxins, and TSST-1, at concentrations below those required for growth inhibition.
Tea Tree Oil Decolonization Studies
Several clinical trials have evaluated tea tree oil for MRSA decolonization in hospital and community settings. A randomized controlled trial published in the Journal of Hospital Infection compared a tea tree oil-based decolonization regimen (nasal ointment plus body wash) with standard mupirocin and chlorhexidine in MRSA-colonized hospital patients. While overall decolonization rates were similar between groups, tea tree oil was significantly more effective at clearing nasal colonization than chlorhexidine alone. Other studies have demonstrated that 5% tea tree oil nasal ointment achieves MRSA nasal clearance rates of 33 to 47%, comparable to mupirocin in some populations, with the advantage of less resistance development.
Berberine and Efflux Pump Inhibition
Perhaps the most pharmacologically significant finding in herbal anti-MRSA research is berberine's ability to inhibit bacterial efflux pumps. The NorA efflux pump in S. aureus actively exports a range of structurally diverse antimicrobial compounds from the cell, conferring resistance to fluoroquinolones, biocides, and plant alkaloids including berberine itself. Research has shown that berberine, when combined with efflux pump inhibitors such as 5'-methoxyhydnocarpin (5'-MHC, a flavonolignan found naturally alongside berberine in plants such as Berberis species), demonstrates dramatically enhanced antibacterial activity. This combination — which occurs naturally in goldenseal and barberry — reduces the MIC of berberine against S. aureus by 8 to 16-fold. This discovery revealed an elegant co-evolutionary strategy: the plant produces both the antibiotic (berberine) and the efflux pump inhibitor (5'-MHC) that ensures the antibiotic reaches effective intracellular concentrations in the bacterial target.
Further research has demonstrated that berberine and related efflux pump inhibitors can restore the sensitivity of MRSA strains to conventional antibiotics, including fluoroquinolones and tetracyclines, that had been rendered ineffective by efflux-mediated resistance. This positions berberine and related compounds not as antibiotic replacements, but as antibiotic adjuvants that could extend the useful life of existing antimicrobial drugs.
Manuka Honey in MRSA Wound Care
Clinical evidence supporting manuka honey for MRSA-infected wounds has accumulated from case series, observational studies, and randomized trials. A systematic review published in the International Journal of General Medicine analyzed clinical outcomes of medical-grade honey in chronic wound management and found evidence of improved healing rates, reduced wound size, effective bacterial clearance, and decreased pain in wounds colonized or infected with MRSA. In vitro studies have shown that S. aureus (including MRSA) does not develop resistance to manuka honey even after prolonged sub-inhibitory exposure, in contrast to the rapid resistance development observed with conventional antibiotics. The multiple mechanisms of action — osmotic stress, low pH, methylglyoxal activity, hydrogen peroxide generation, and bee defensin-1 — create a multi-target assault that makes resistance development unlikely.
8. Biofilm Formation and Herbal Disruption
How S. aureus Forms Biofilms
S. aureus biofilm development is a complex, multi-stage process. In the attachment phase, planktonic (free-floating) bacteria adhere to a surface via surface proteins (MSCRAMMs) and non-specific hydrophobic interactions. During the accumulation phase, attached bacteria multiply and produce extracellular polymeric substances (EPS) — primarily polysaccharide intercellular adhesin (PIA, encoded by the icaADBC operon), extracellular DNA released through controlled autolysis, and various surface proteins. In the maturation phase, the biofilm develops a three-dimensional architecture with fluid-filled channels that allow nutrient delivery to deeper layers. Bacteria within the mature biofilm adopt a distinct phenotype characterized by reduced metabolic activity, altered gene expression, and enhanced stress tolerance. Finally, during the dispersal phase, enzymatic degradation of the matrix (via proteases, nucleases, and phenol-soluble modulins) releases planktonic cells that can colonize new sites.
Why Biofilms Resist Antibiotics
Biofilm-associated S. aureus infections are notoriously difficult to treat for multiple reasons. The EPS matrix acts as a physical barrier that limits antibiotic penetration, with some antibiotics (e.g., vancomycin) binding to matrix components and failing to reach effective concentrations in deeper biofilm layers. Bacteria in the biofilm interior exist in a dormant or slow-growing state (persister cells), making them insensitive to antibiotics that target active cellular processes. The biofilm microenvironment features pH gradients, oxygen depletion, and waste product accumulation that can inactivate certain antibiotics. Additionally, the high cell density within biofilms facilitates horizontal gene transfer, potentially accelerating the spread of resistance genes. The net result is that biofilm-associated infections frequently require 100 to 1,000 times the antibiotic concentration needed to kill planktonic cells, concentrations that are often unachievable in vivo without unacceptable toxicity.
Herbs That Disrupt S. aureus Biofilms
Several plant-derived compounds have demonstrated the ability to prevent biofilm formation, penetrate established biofilms, and kill biofilm-embedded bacteria:
- Oregano (carvacrol): Carvacrol inhibits S. aureus biofilm formation at sub-MIC concentrations by downregulating the expression of icaA (encoding PIA synthesis) and genes involved in quorum sensing. At higher concentrations, carvacrol penetrates and disrupts mature biofilm architecture, killing embedded bacteria. Studies have reported 60 to 90% biofilm biomass reduction with carvacrol treatment at 2 to 4 times the planktonic MIC.
- Garlic (allicin, ajoene): Ajoene interferes with quorum sensing in S. aureus biofilms by inhibiting the agr (accessory gene regulator) system, which controls the switch between adhesion and dispersal phenotypes. Allicin has demonstrated ability to reduce biofilm formation by 50 to 70% at sub-inhibitory concentrations. Garlic extracts have also shown synergy with antibiotics against biofilm-embedded S. aureus, with combinations of garlic extract and rifampicin reducing biofilm viable counts by 3 to 4 log units more than either agent alone.
- Cinnamon (cinnamaldehyde): Trans-cinnamaldehyde, the major component of cinnamon bark oil, inhibits S. aureus biofilm formation in a dose-dependent manner at concentrations as low as one-quarter of the MIC. Cinnamaldehyde interferes with the bacterial quorum sensing system and reduces the production of extracellular polysaccharides. It has also demonstrated the ability to eradicate preformed biofilms, with studies showing significant reduction in viable bacteria within 24-hour-old S. aureus biofilms at concentrations of 0.1 to 0.5% (v/v).
- Andrographis (andrographolide): Andrographolide, the primary diterpene lactone from Andrographis paniculata, has shown anti-biofilm activity against S. aureus through inhibition of sortase A, a transpeptidase enzyme essential for anchoring surface proteins to the peptidoglycan layer. Because many MSCRAMMs that mediate biofilm attachment are sortase A substrates, andrographolide disrupts the initial attachment phase of biofilm formation. Studies have demonstrated 40 to 70% inhibition of S. aureus biofilm formation with andrographolide at sub-MIC concentrations, without affecting planktonic growth, suggesting anti-virulence rather than bactericidal activity.
9. Prevention and Hygiene
Preventing S. aureus infections, particularly MRSA, requires a multi-faceted approach encompassing personal hygiene, wound care, environmental measures, and in some cases, active decolonization.
Hand Hygiene
Hand washing remains the single most effective measure for preventing the transmission of S. aureus, including MRSA. Hands should be washed thoroughly with soap and water for at least 20 seconds, particularly after touching wounds, handling bandages, using the bathroom, and before preparing food. Alcohol-based hand sanitizers (containing at least 60% alcohol) are effective against S. aureus when soap and water are not available, though they are less effective if hands are visibly soiled.
Wound Care
Proper wound management is critical for preventing S. aureus infection. All cuts, scrapes, and abrasions should be cleaned promptly with soap and water, treated with an appropriate antiseptic, and covered with a clean, dry bandage until healed. Wound dressings should be changed regularly, and any signs of infection (increasing redness, warmth, swelling, pain, or purulent drainage) should prompt medical evaluation. Drainage from infected wounds contains high concentrations of S. aureus and is a major source of environmental contamination and person-to-person transmission.
Personal Items and Environmental Measures
Sharing personal items that contact the skin — including towels, razors, bar soap, athletic equipment, and clothing — should be avoided, as these items can serve as fomites for S. aureus transmission. In households or communities with recurrent MRSA infections, environmental cleaning with household disinfectants or dilute bleach solutions (1 tablespoon of bleach per quart of water) should focus on high-touch surfaces including doorknobs, light switches, countertops, and bathroom fixtures. Clothing, towels, and bed linens should be laundered in hot water with regular detergent and dried in a hot dryer.
Decolonization Protocols
For individuals with recurrent S. aureus infections or persistent MRSA carriage, decolonization protocols aim to eliminate the organism from its colonization sites, thereby reducing the risk of subsequent infection and transmission. Standard decolonization regimens include:
- Intranasal mupirocin ointment (2%) applied twice daily for 5 days to eradicate nasal carriage
- Chlorhexidine gluconate (2% or 4%) body washes for 5 to 14 days to reduce skin colonization
- Dilute bleach baths (one-quarter to one-half cup of regular household bleach in a full bathtub of water) twice weekly for up to 3 months
- Treatment of all colonized household contacts simultaneously to prevent recolonization
Decolonization success rates vary from 25 to 80% at 3 months, and recolonization is common, particularly when household contacts are not treated concurrently. Tea tree oil-based nasal preparations and body washes have been evaluated as alternatives to mupirocin and chlorhexidine, with the potential advantage of reduced resistance development.
Key Research Papers
Foundational and contemporary peer-reviewed studies on Staphylococcus aureus — from foundational MRSA epidemiology and IDSA treatment guidelines to community-associated MRSA, toxin biology, biofilm-mediated device infection, and endocarditis. Each citation links to the full text via DOI.
- Lowy FD. Staphylococcus aureus Infections. New England Journal of Medicine. 1998;339(8):520–532.
- Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG Jr. Staphylococcus aureus Infections: Epidemiology, Pathophysiology, Clinical Manifestations, and Management. Clinical Microbiology Reviews. 2015;28(3):603–661.
- Liu C, Bayer A, Cosgrove SE, et al. Clinical Practice Guidelines by the IDSA for the Treatment of Methicillin-Resistant Staphylococcus aureus Infections in Adults and Children. Clinical Infectious Diseases. 2011;52(3):e18–e55.
- DeLeo FR, Otto M, Kreiswirth BN, Chambers HF. Community-Associated Meticillin-Resistant Staphylococcus aureus. Lancet. 2010;375(9725):1557–1568.
- Otto M. Staphylococcus aureus Toxins. Current Opinion in Microbiology. 2014;17:32–37.
- Fowler VG Jr, Miro JM, Hoen B, et al. Staphylococcus aureus Endocarditis: A Consequence of Medical Progress. JAMA. 2005;293(24):3012–3021.
- Chambers HF, DeLeo FR. Waves of Resistance: Staphylococcus aureus in the Antibiotic Era. Nature Reviews Microbiology. 2009;7(9):629–641.
- Costerton JW, Stewart PS, Greenberg EP. Bacterial Biofilms: A Common Cause of Persistent Infections. Science. 1999;284(5418):1318–1322.
- Lu J, Turnbull L, Burke CM, et al. Manuka-Type Honeys Can Eradicate Biofilms Produced by Staphylococcus aureus Strains with Different Biofilm-Forming Abilities. PLOS ONE. 2014;9(3):e91921.
- Carson CF, Hammer KA, Riley TV. Melaleuca alternifolia (Tea Tree) Oil: A Review of Antimicrobial and Other Medicinal Properties. Clinical Microbiology Reviews. 2006;19(1):50–62.
- Stermitz FR, Lorenz P, Tawara JN, Zenewicz LA, Lewis K. Synergy in a Medicinal Plant: Antimicrobial Action of Berberine Potentiated by 5′-Methoxyhydnocarpin, a Multidrug Pump Inhibitor. Proceedings of the National Academy of Sciences. 2000;97(4):1433–1437.
- Dryden MS, Dailly S, Crouch M. A Randomized, Controlled Trial of Tea Tree Topical Preparations versus a Standard Topical Regimen for the Clearance of MRSA Colonization. Journal of Hospital Infection. 2004;56(4):283–286.
- Murray CJL, Ikuta KS, Sharara F, et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet. 2022;399(10325):629–655.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Staphylococcus aureus review
- MRSA methicillin resistant Staphylococcus aureus
- Staphylococcus aureus bacteremia endocarditis
- Staphylococcus aureus toxic shock syndrome
- Staphylococcus aureus biofilm device infection
- Vancomycin Staphylococcus aureus MIC
- Panton Valentine leukocidin Staphylococcus
- Staphylococcus aureus nasal carriage decolonization
- Community acquired MRSA skin infection
- Daptomycin MRSA bacteremia
- Manuka honey Staphylococcus aureus
Connections
- Garlic
- Oregano
- Manuka Honey
- Tea Tree
- Thyme
- Andrographis
- Goldenseal
- Cinnamon
- Sepsis
- Cellulitis
- Escherichia Coli
- Silver Nanoparticles
- Pseudomonas Aeruginosa
- Pneumonia
- Endocarditis
- Berberine
- Immune Boosting
- Antibacterial Herbs