Numbness and Tingling
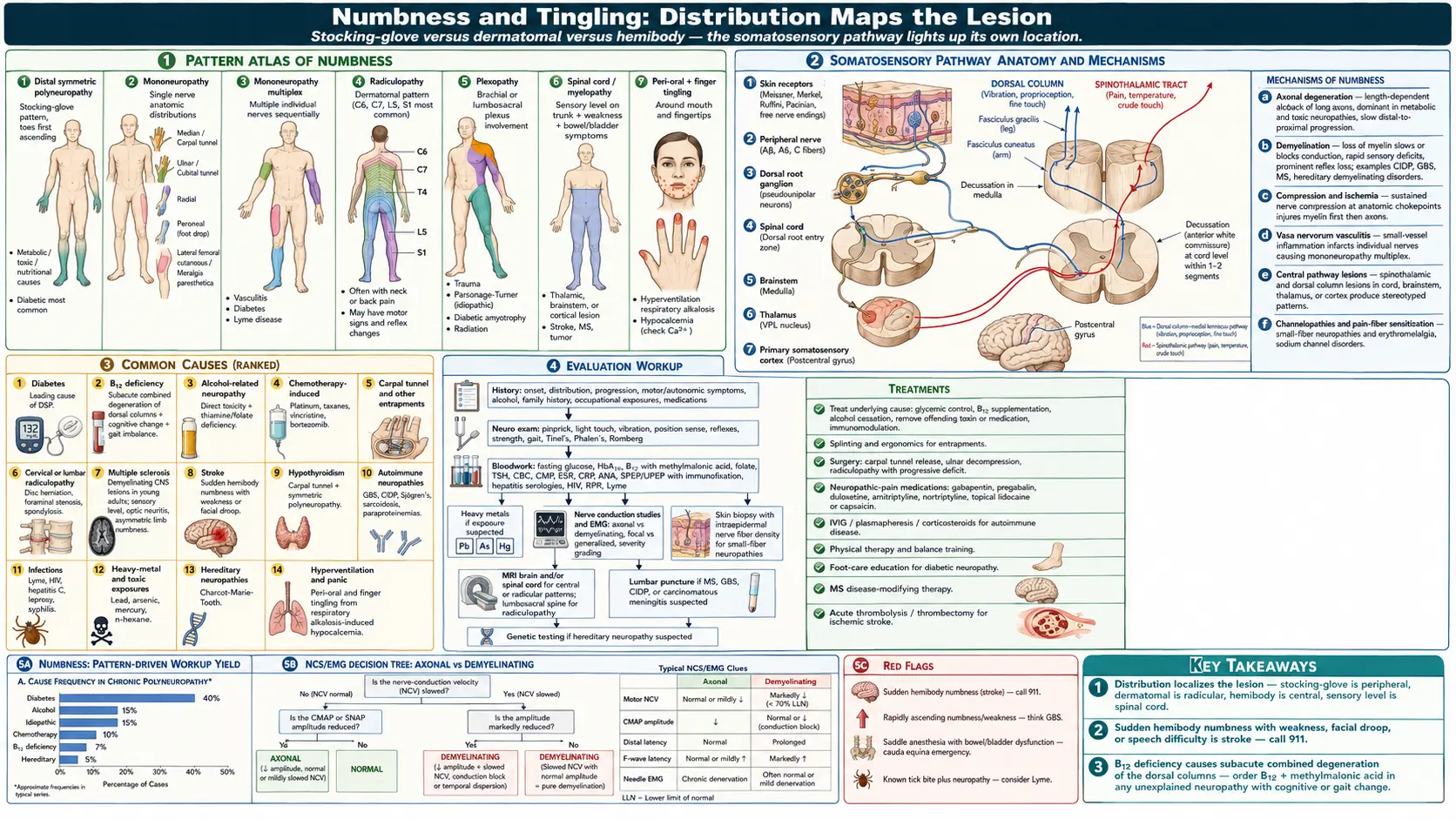
Table of Contents
- Overview
- Patterns of Numbness
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Numbness (loss of sensation) and tingling (paresthesia, "pins and needles") reflect dysfunction anywhere along the somatosensory pathway — small or large peripheral nerve fibers, dorsal roots, spinal cord tracts, brainstem nuclei, thalamus, or sensory cortex. The distribution of the symptoms is the single most useful clue: distal symmetric stocking-glove patterns suggest a length-dependent peripheral neuropathy (most often diabetic, alcohol-related, B12 deficiency, or chemotherapy); focal asymmetric patterns suggest a single nerve, plexus, or root lesion; multifocal or central patterns raise concern for multiple sclerosis, stroke, or spinal cord pathology and are often more urgent.
Patterns of Numbness
- Distal symmetric polyneuropathy (stocking-glove) — the most common pattern; toes first, slowly ascending; usually metabolic, toxic, or nutritional.
- Mononeuropathy — single nerve in its anatomic distribution: median (carpal tunnel), ulnar (cubital tunnel), radial, peroneal, lateral femoral cutaneous (meralgia paresthetica).
- Mononeuropathy multiplex — multiple individual nerves involved sequentially; classic in vasculitis, diabetes, and Lyme disease.
- Radiculopathy — nerve-root distribution; cervical (C6, C7) or lumbar (L5, S1) most common; often with neck or back pain and motor signs.
- Plexopathy — brachial or lumbosacral plexus; trauma, idiopathic (Parsonage-Turner), diabetic, or radiation-related.
- Spinal cord (myelopathy) — sensory level on the trunk, often with weakness and bowel/bladder involvement; emergencies include cord compression and transverse myelitis.
- Hemibody — thalamic, brainstem, or cortical lesion; consider stroke, MS, tumor.
- Peri-oral and finger tingling — often hyperventilation or hypocalcemia.
Common Causes
- Diabetes — the leading cause of distal symmetric polyneuropathy in developed countries.
- B12 deficiency — can produce subacute combined degeneration of the dorsal columns, with paresthesias, gait imbalance, and cognitive change.
- Alcohol-related neuropathy — from direct toxicity and associated thiamine and folate deficiencies.
- Chemotherapy-induced peripheral neuropathy — platinum agents, taxanes, vincristine, bortezomib.
- Carpal tunnel syndrome and other entrapments — median nerve at the wrist, ulnar at the elbow, peroneal at the fibular head.
- Cervical or lumbar radiculopathy — disc herniation, foraminal stenosis, spondylosis.
- Multiple sclerosis — demyelinating CNS lesions; often present in young adults with a sensory level, optic neuritis, or asymmetric limb numbness.
- Stroke — sudden hemibody numbness, often with weakness or facial droop.
- Hypothyroidism — can cause carpal tunnel syndrome and symmetric polyneuropathy.
- Autoimmune neuropathies — Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy (CIDP), Sjögren's, sarcoidosis, paraproteinemias.
- Infections — Lyme disease, HIV, hepatitis C, leprosy, syphilis.
- Heavy-metal and toxic exposures — lead, arsenic, mercury, n-hexane.
- Hereditary neuropathies — Charcot-Marie-Tooth disease.
- Hyperventilation and panic — produces peri-oral and finger tingling from respiratory alkalosis-induced hypocalcemia.
Mechanisms
- Axonal degeneration — length-dependent dieback of long axons; the dominant mechanism in metabolic and toxic neuropathies, with slow distal-to-proximal progression.
- Demyelination — loss of myelin slows or blocks conduction; rapid sensory deficits, often with prominent reflex loss out of proportion to atrophy. Seen in CIDP, Guillain-Barré, MS, hereditary demyelinating neuropathies.
- Compression and ischemia — sustained nerve compression at anatomic chokepoints injures myelin first, then axons.
- Vasa nervorum vasculitis — small-vessel inflammation infarcts individual nerves, producing mononeuropathy multiplex.
- Central pathways — spinothalamic and dorsal column pathway lesions in cord, brainstem, thalamus, or cortex produce stereotyped patterns.
- Channelopathies and pain-fiber sensitization — small-fiber neuropathies and erythromelalgia involve sodium channels.
Evaluation
- History — onset, distribution, progression, motor or autonomic symptoms, alcohol, family history, occupational exposures, medications.
- Neurologic exam — pinprick, light touch, vibration, position sense, reflexes, strength, gait, Tinel's and Phalen's signs, Romberg.
- Bloodwork — fasting glucose, HbA1c, B12 with methylmalonic acid, folate, TSH, CBC, comprehensive metabolic panel, ESR, CRP, ANA, SPEP/UPEP with immunofixation, hepatitis serologies, HIV, RPR, Lyme.
- Heavy metals — if exposure or unexplained neuropathy.
- Nerve conduction studies and electromyography (NCS/EMG) — classify axonal vs demyelinating, focal vs generalized, and grade severity.
- Skin biopsy with intraepidermal nerve fiber density — for small-fiber neuropathies.
- MRI — brain and/or spinal cord for central or radicular patterns; lumbosacral spine for radiculopathy.
- Lumbar puncture — if MS, GBS/CIDP, or carcinomatous meningitis suspected.
- Genetic testing — if hereditary neuropathy suspected.
Management
- Treat the underlying cause — glycemic control, B12 supplementation, alcohol cessation, removal of offending toxin or medication, immunomodulation in autoimmune neuropathies.
- Splinting and ergonomic changes — carpal tunnel and other entrapments often respond to splinting, posture changes, and physical therapy before surgery.
- Surgery — carpal tunnel release, ulnar nerve decompression, radiculopathy with progressive deficit.
- Neuropathic-pain medications — gabapentin, pregabalin, duloxetine, amitriptyline, nortriptyline; topical lidocaine or capsaicin.
- IVIG, plasmapheresis, corticosteroids — for autoimmune and inflammatory neuropathies.
- Physical therapy and balance training — reduces falls in distal sensory loss.
- Foot care education — daily inspection and good footwear in diabetic neuropathy to prevent ulcers.
- Disease-modifying therapy — in MS, B-cell-depleting agents and other DMTs.
- Acute thrombolysis or thrombectomy — for ischemic stroke causing sudden numbness.
When to Seek Medical Care
- Sudden onset of one-sided numbness, especially with weakness, facial droop, or speech difficulty — call 911 (possible stroke).
- Rapidly ascending numbness and weakness from feet upward — possible Guillain-Barré syndrome.
- Saddle-area numbness, new bowel or bladder incontinence, or progressive leg weakness — possible cauda equina syndrome.
- Numbness with severe back pain after trauma or in someone with cancer or immunosuppression.
- Numbness with vision change or loss in one eye (consider optic neuritis or MS).
- Rapidly progressive numbness in an immunocompromised patient.
- Numbness following a known tick bite.
Connections
- All Symptoms
- Diabetes
- Multiple Sclerosis
- Vitamin B12
- Peripheral Neuropathy
- ALS
- Joint Pain
- Chronic Pain
- Brain Fog
- Thyroid Disorders
- Vitamin B9 (Folate)
- Stroke
- Carpal Tunnel Syndrome
- Lyme Disease
- Heavy Metals
- Comprehensive Metabolic Panel
- Dizziness
- Cold Hands Feet
- Herniated Disc
- Peripheral Neuropathy
- Muscle Cramps
References & Research
Historical Background
The systematic classification of peripheral neuropathies began with electrodiagnostic studies in the 1960s and 1970s. Diabetic neuropathy was epidemiologically characterized in the Pittsburgh and Rochester studies; the discovery that intensive glycemic control reduces incidence (DCCT, 1993) reshaped management. Idebenone, alpha-lipoic acid, and acetyl-L-carnitine have been studied as neuroprotective agents with mixed results, while neuropathic-pain therapeutics have advanced from older tricyclics to gabapentinoids and SNRIs.
Key Research Papers
- Pop-Busui R, Boulton AJM, Feldman EL, et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 2017;40(1):136-154.
- DCCT Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. New England Journal of Medicine. 1993;329(14):977-986.
- Hanewinckel R, van Oijen M, Ikram MA, van Doorn PA. The epidemiology and risk factors of chronic polyneuropathy. European Journal of Epidemiology. 2016;31(1):5-20.
- England JD, Asbury AK. Peripheral neuropathy. The Lancet. 2004;363(9427):2151-2161.
- Reich DS, Lucchinetti CF, Calabresi PA. Multiple sclerosis. New England Journal of Medicine. 2018;378(2):169-180.
- Stalberg E, Falck B. Clinical motor nerve conduction studies. Methods in Clinical Neurophysiology. 1996.
- Callaghan BC, Price RS, Chen KS, Feldman EL. The importance of rare subtypes in diagnosis and treatment of peripheral neuropathy: a review. JAMA Neurology. 2015;72(12):1510-1518.
- Lauria G, Hsieh ST, Johansson O, et al. European Federation of Neurological Societies / Peripheral Nerve Society guideline on the use of skin biopsy in the diagnosis of small fiber neuropathy. European Journal of Neurology. 2010;17(7):903-912.
- Hughes RAC, Cornblath DR. Guillain-Barré syndrome. The Lancet. 2005;366(9497):1653-1666.
- Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurology. 2015;14(2):162-173.
PubMed Topic Searches
- Peripheral neuropathy evaluation
- Diabetic neuropathy treatment
- B12 deficiency and subacute combined degeneration
- Multiple sclerosis sensory symptoms
- Carpal tunnel syndrome diagnosis
- Small-fiber neuropathy and skin biopsy