Cold Hands and Feet
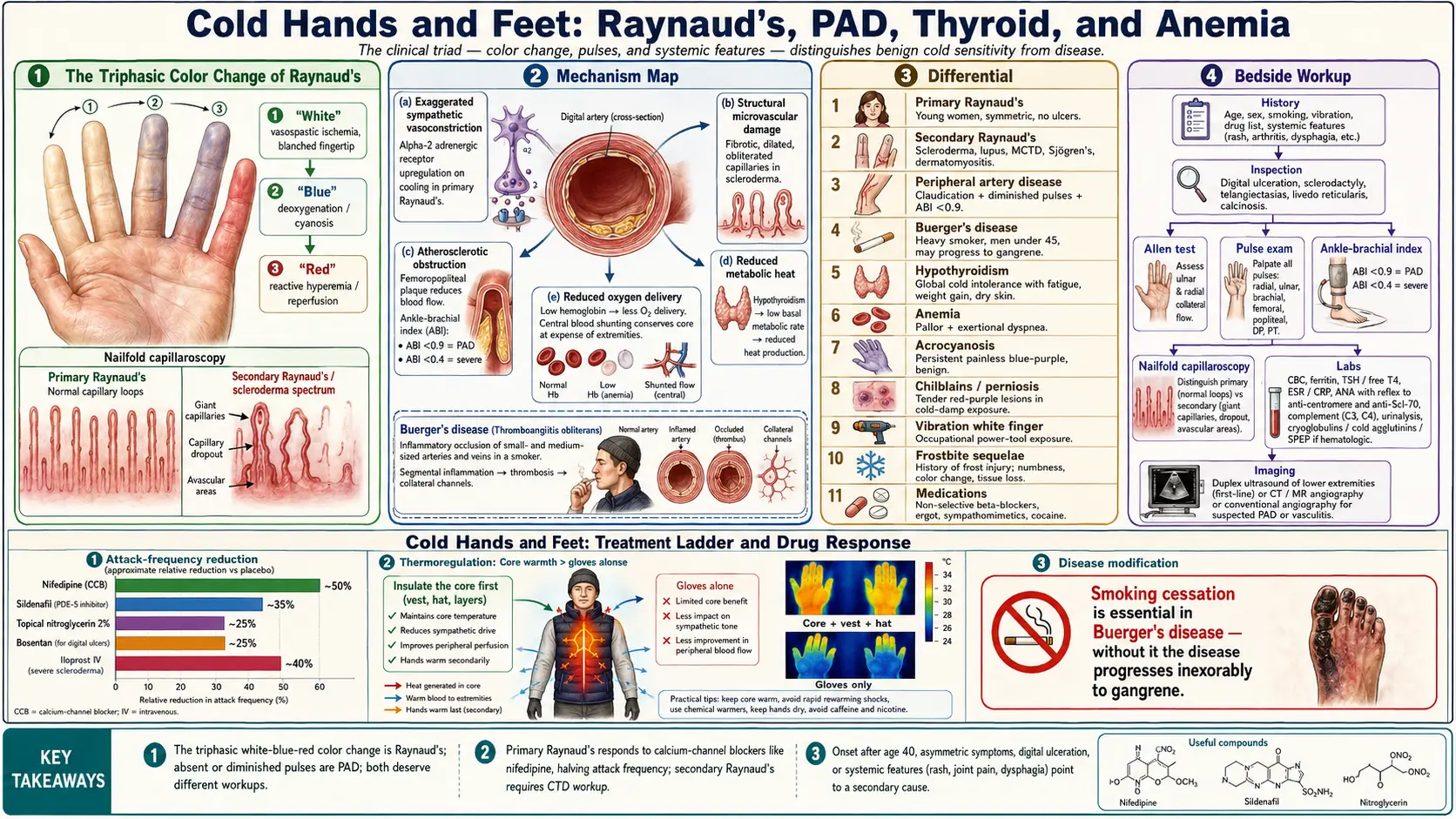


Table of Contents
- Overview
- Types
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Cold hands and feet span a spectrum from benign vasoconstriction — a chilly room, low body fat, anxiety, or simple physiological cold sensitivity — all the way to vascular disease and connective tissue disease. Most people experience cold extremities occasionally without any underlying pathology, but persistent or asymmetric cold extremities deserve evaluation. The clinical triad to assess is straightforward: color change (a white-blue-red triphasic pattern points strongly to Raynaud's phenomenon), pulses (absent or diminished pulses suggest peripheral artery disease), and associated systemic features (cold intolerance with fatigue, weight gain, and dry skin suggests hypothyroidism; cold extremities with pallor and exertional dyspnea suggest anemia). Onset after age 40, asymmetric symptoms, digital ulceration, or systemic features such as joint pain, rash, or dysphagia all raise the probability of a secondary cause that requires specific treatment.
Types
- Primary Raynaud's phenomenon — idiopathic, typically begins in young women, symmetric, no underlying disease, no digital ulceration, normal nailfold capillaries.
- Secondary Raynaud's phenomenon — associated with scleroderma, lupus, mixed connective tissue disease, Sjögren's, dermatomyositis, or hematologic disease. Often asymmetric, may progress to digital ulceration or gangrene, abnormal nailfold capillaroscopy.
- Peripheral artery disease (PAD) — atherosclerotic obstruction of large or medium-sized arteries, producing cold extremities with claudication, diminished pulses, and a low ankle-brachial index.
- Microvascular cold sensitivity — small-vessel disease from diabetes, smoking, or chronic kidney disease. Pulses are typically preserved but capillary blood flow is impaired.
- Metabolic cold intolerance — reduced metabolic heat production from hypothyroidism, anemia, low body weight, or anorexia nervosa. Whole-body cold sensitivity rather than focal extremity findings.
- Acrocyanosis — persistent, painless, symmetric blue-purple discoloration of hands and feet, often with sweating. Benign, usually idiopathic, no triphasic color change.
- Chilblains (perniosis) — tender, itchy, red-purple lesions on toes or fingers triggered by exposure to cold and damp conditions. Self-limited but recurrent.
Common Causes
- Primary Raynaud's phenomenon — idiopathic vasospasm of the digital arteries, most often in women between ages 15 and 30. Episodes are triggered by cold or emotional stress.
- Secondary Raynaud's — scleroderma, lupus, mixed connective tissue disease, Sjögren's syndrome, dermatomyositis, and rheumatoid arthritis.
- Peripheral artery disease — atherosclerotic obstruction driven by smoking, diabetes, hyperlipidemia, hypertension, and age. Produces cold extremities, claudication, and diminished pulses.
- Buerger's disease (thromboangiitis obliterans) — segmental inflammatory occlusion of small and medium arteries in heavy tobacco smokers, almost always in men under 45. May progress to digital gangrene unless smoking is stopped.
- Hypothyroidism — reduced metabolic rate produces global cold intolerance, fatigue, weight gain, dry skin, constipation, and bradycardia.
- Anemia — reduced oxygen-carrying capacity and compensatory peripheral vasoconstriction produce cold extremities, pallor, and exertional dyspnea.
- Hypothalamic dysfunction — impaired thermoregulation in anorexia nervosa, severe weight loss, panhypopituitarism, or hypothalamic injury.
- Medications — non-selective beta-blockers, ergot alkaloids, sympathomimetics, certain chemotherapy agents (bleomycin, cisplatin), and stimulants can provoke or worsen vasoconstriction.
- Cocaine and other vasoconstrictors — intense sympathetic stimulation can produce digital ischemia and Raynaud's-like attacks.
- Vibration injury (vibration white finger) — chronic occupational exposure to hand-held power tools causes structural microvascular damage and cold-induced episodes.
- Frostbite history — previous cold injury permanently lowers the threshold for cold-induced vasoconstriction in the affected fingers and toes.
Mechanisms
Cold extremities reflect either reduced delivery of warm blood to the skin and digits, reduced metabolic heat production, or both. Most patients have one dominant mechanism:
- Exaggerated sympathetic vasoconstriction — in primary Raynaud's, otherwise normal digital arteries respond to cold or stress with intense, prolonged contraction. Alpha-2 adrenergic receptors are upregulated on cooling, amplifying the response.
- Structural microvascular damage — in scleroderma and other connective tissue diseases, the digital and nailfold capillaries become fibrotic, dilated, and obliterated. Capillaroscopy reveals dropout, giant capillaries, and avascular areas. The vasospastic response is layered on top of fixed obstructive disease.
- Atherosclerotic obstruction — in PAD, plaque narrows the femoral, popliteal, or tibial arteries and limits flow at rest or during exertion. Collaterals partly compensate but cannot match demand under cold or activity stress.
- Reduced metabolic heat — in hypothyroidism, basal metabolic rate falls, decreasing whole-body heat production. Low body mass and low body fat similarly reduce both heat generation and insulation.
- Reduced oxygen delivery — in anemia, hemoglobin is insufficient to carry adequate oxygen to peripheral tissues. The body responds by shunting blood centrally, leaving the extremities cold and pale.
- Inflammatory occlusion — in Buerger's disease and small-vessel vasculitis, segmental inflammation thromboses small arteries, producing focal ischemia.
Evaluation
Workup is guided by age of onset, symmetry, presence of triphasic color change, and any systemic features. A reasonable starting set includes:
- History — age of onset, sex, smoking history, occupational vibration exposure, drug list (beta-blockers, ergot, stimulants, cocaine), systemic symptoms (rash, joint pain, dry eyes/mouth, dysphagia, dyspnea, weight change).
- Physical exam — inspect for color change, digital ulceration, sclerodactyly, telangiectasias, calcinosis, livedo reticularis, rash, and synovitis. Compare hand temperatures, perform Allen test for radial/ulnar arch patency, palpate all peripheral pulses.
- Ankle-brachial index (ABI) — bedside ratio of ankle to arm systolic pressure. Values below 0.9 indicate PAD; below 0.4 indicates severe disease.
- Nailfold capillaroscopy — magnified inspection of the proximal nailfold. Normal in primary Raynaud's; shows giant capillaries, dropout, and disorganization in scleroderma-spectrum disease.
- Bloodwork — CBC (anemia), ferritin and iron studies, TSH and free T4 (thyroid), comprehensive metabolic panel, ESR and CRP (inflammation), ANA with reflex to anti-centromere and anti-Scl-70 antibodies (scleroderma spectrum), complement levels, and urinalysis.
- Specialized antibody panel — anti-dsDNA, anti-Ro/La, anti-RNP, anti-Jo-1 if connective tissue disease is suspected on initial screening.
- Cryoglobulins, cold agglutinins, serum protein electrophoresis — if hematologic or paraproteinemic cause is suspected.
- Duplex ultrasound or angiography — for confirmed or suspected PAD, to localize and quantify obstruction.
- Cold provocation testing — in selected occupational or research settings; not routinely needed in clinical practice.
Management
- Keep the core warm — maintaining trunk warmth is often more effective than gloves and socks alone, because peripheral vasoconstriction is partly driven by central thermoregulatory reflexes. Layered clothing, hats, and warm vests reduce attack frequency.
- Avoid triggers — cold air, cold water, sudden temperature changes, emotional stress, vibration, and tobacco. Use insulated gloves before entering refrigerated sections of supermarkets.
- Smoking cessation — essential in Buerger's disease (without cessation, the disease progresses inexorably) and central in PAD treatment.
- Calcium-channel blockers — nifedipine extended-release 30–60 mg daily or amlodipine 5–10 mg daily are first-line drug therapy for Raynaud's. They reduce attack frequency by roughly half in most patients.
- Phosphodiesterase-5 inhibitors — sildenafil or tadalafil for severe digital ischemia, particularly in scleroderma-associated Raynaud's with digital ulcers.
- Topical nitroglycerin — 2 percent ointment applied to affected digits can abort an attack or speed recovery; headache is the limiting side effect.
- Prostacyclin analogs — intravenous iloprost for refractory digital ulcers in scleroderma; produces sustained improvement in healing.
- Endothelin-receptor antagonists — bosentan reduces new digital ulcer formation in scleroderma.
- Treat the underlying connective tissue disease — immunosuppression, antifibrotic agents, and disease-specific therapy alter the course of secondary Raynaud's.
- Antiplatelet therapy and statins for PAD — aspirin or clopidogrel plus a high-intensity statin reduce cardiovascular events. Cilostazol improves walking distance. Revascularization (angioplasty, stenting, bypass) is reserved for limiting claudication or threatened limbs.
- Levothyroxine for hypothyroidism — restores metabolic rate; cold intolerance often resolves within weeks of normalizing TSH.
- Iron repletion for anemia — oral or intravenous iron based on severity and tolerance, plus treatment of any underlying cause of iron loss.
- Biofeedback and autogenic training — behavioral therapies that train conscious peripheral vasodilation; effective in primary Raynaud's with sustained practice.
- Sympathectomy — surgical or chemical interruption of the sympathetic nerves to the affected limb; reserved for refractory severe cases with threatened tissue loss.
When to Seek Medical Care
- Digital ulceration, blackened fingertips, or frank gangrene.
- Sudden, severe cold and pulseless extremity with pain — acute limb ischemia is an emergency requiring immediate evaluation.
- Asymmetric symptoms (one hand or foot affected far more than the other) suggest fixed arterial disease rather than primary Raynaud's.
- Onset after age 40, or onset in a man — both raise the probability of a secondary cause.
- Raynaud's accompanied by systemic features such as rash, joint pain, dry eyes or mouth, dysphagia, shortness of breath, or skin tightening.
- Cold intolerance with progressive fatigue, weight gain, hair loss, or constipation (consider hypothyroidism).
- Cold extremities with pallor, exertional dyspnea, or palpitations (consider anemia).
- Calf pain with walking that resolves with rest (intermittent claudication) plus cold extremities suggests PAD.
Connections
- Anemia
- Peripheral Artery Disease
- Lupus
- Raynaud's Disease
- Thyroid Disorders
- Sjögren's Syndrome
- Fatigue
- Diabetes
- Lightheadedness
- Numbness & Tingling
- Hashimoto's Thyroiditis
- Iron
- Joint Pain
- Hypertension
- Inflammatory Markers
References & Research
Historical Background
The phenomenon now bearing his name was first described by French medical student Maurice Raynaud in his 1862 doctoral thesis De l'asphyxie locale et de la gangrène symétrique des extrémités, in which he documented twenty-five cases of episodic digital ischemia and proposed an autonomic-nervous-system origin. Edgar Allen described his bedside test of radial and ulnar arch patency in 1929, providing the first reproducible method to assess hand circulation at the bedside. Pharmacologic management began in earnest in the 1980s when nifedipine was shown to reduce attack frequency in primary Raynaud's; in subsequent decades, bosentan and intravenous iloprost transformed the management of digital ulcers in systemic sclerosis. The 2013 ACR/EULAR classification criteria for systemic sclerosis allowed earlier and more reproducible identification of secondary Raynaud's, while nailfold capillaroscopy moved from research tool to routine office procedure.
Key Research Papers
- Wigley FM. Clinical practice. Raynaud's phenomenon. New England Journal of Medicine. 2002;347(13):1001-1008.
- van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Annals of the Rheumatic Diseases. 2013;72(11):1747-1755.
- Kowal-Bielecka O, Fransen J, Avouac J, et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Annals of the Rheumatic Diseases. 2017;76(8):1327-1339.
- Korn JH, Mayes M, Matucci Cerinic M, et al. Digital ulcers in systemic sclerosis: prevention by treatment with bosentan, an oral endothelin receptor antagonist. Arthritis & Rheumatism. 2004;50(12):3985-3993.
- Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease. Circulation. 2017;135(12):e726-e779.
- Aboyans V, Ricco JB, Bartelink MEL, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases. European Heart Journal. 2018;39(9):763-816.
- Belch JJ, Ho M. Pharmacotherapy of Raynaud's phenomenon. Drugs. 1996;52(5):682-695.
- Thompson AE, Pope JE. Calcium channel blockers for primary Raynaud's phenomenon: a meta-analysis. Rheumatology. 2005;44(2):145-150.
- Herrick AL. The pathogenesis, diagnosis and treatment of Raynaud phenomenon. Nature Reviews Rheumatology. 2012;8(8):469-479.
- Olin JW, Sealove BA. Peripheral artery disease: current insight into the disease and its diagnosis and management. Mayo Clinic Proceedings. 2010;85(7):678-692.
PubMed Topic Searches
- Raynaud phenomenon pathogenesis
- Systemic sclerosis and digital ulcers
- Peripheral artery disease diagnosis and management
- Nailfold capillaroscopy in scleroderma
- Hypothyroidism and cold intolerance
- Thromboangiitis obliterans (Buerger's disease)