Carpal Tunnel Syndrome
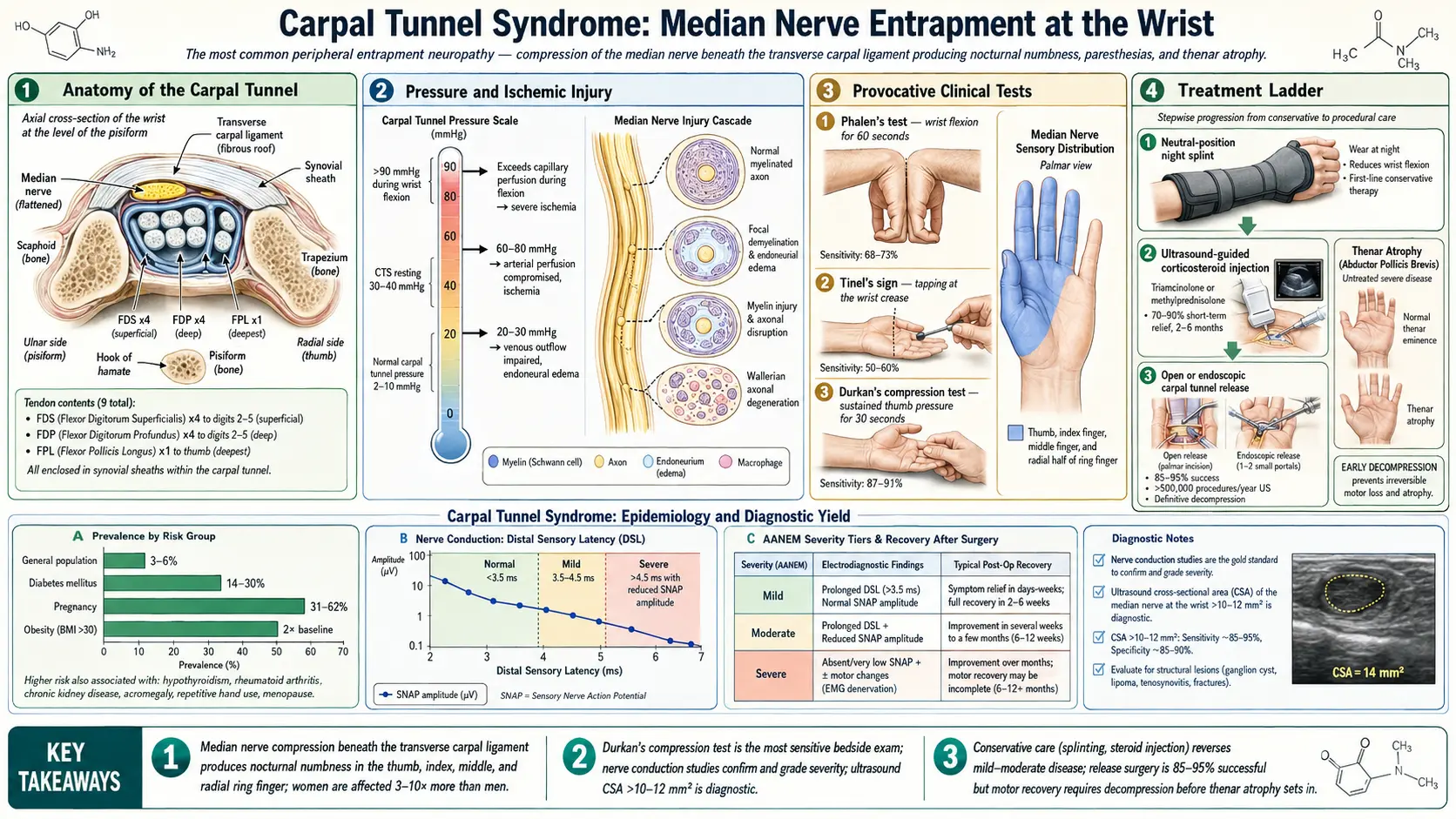
Table of Contents
- Overview
- Epidemiology
- Anatomy of the Carpal Tunnel
- Causes and Risk Factors
- Clinical Presentation
- Diagnosis and Special Tests
- Conservative Treatment
- Surgical Treatment
- Outcomes and Special Populations
- References & Research
- Research Papers
- Connections
- Featured Videos
1. Overview
Waking up in the middle of the night with a burning, tingling hand — and finding that shaking it vigorously makes it feel better — is the textbook story of carpal tunnel syndrome (CTS). It is the most common peripheral nerve entrapment neuropathy in the world, affecting an estimated 3–6% of the general adult population, and it is responsible for more lost work days than almost any other upper-extremity condition. Despite its prevalence, it is still frequently dismissed or delayed in diagnosis because the early symptoms of tingling and nocturnal numbness are easy to attribute to poor sleeping position or "overuse."
CTS occurs when the median nerve is compressed as it travels through the carpal tunnel — a narrow, rigid passageway at the wrist formed by the carpal bones on three sides and the transverse carpal ligament (flexor retinaculum) on the fourth. Because there is no give in that bony and ligamentous channel, any increase in tissue volume within the tunnel — from tendon sheath swelling, fluid retention, arthritic spurs, or any of a dozen other causes — compresses the median nerve and produces the characteristic constellation of symptoms in the thumb, index, middle, and radial half of the ring finger.
The good news is that effective treatments exist at every stage of severity: splinting and injections for mild to moderate cases, and a brief surgical procedure (carpal tunnel release) that is one of the most consistently successful operations in all of medicine for moderate-to-severe or treatment-refractory disease.
2. Epidemiology
CTS is a disease of working-age adults, with peak incidence in the fourth through sixth decades of life. Women are affected two to three times more often than men, a gap that reflects the smaller baseline carpal tunnel dimensions in women, hormonal influences on connective tissue and fluid balance, and the greater prevalence of predisposing conditions such as hypothyroidism and rheumatoid arthritis. Annual incidence in the US is estimated at approximately 3.4 per 1,000 person-years, with prevalence of 50–100 per 1,000 in working populations.
Occupational associations are well documented. Jobs involving sustained or repetitive wrist flexion and extension, sustained grip or pinch, or hand-arm vibration — assembly-line work, meat packing, keyboard-intensive work, dentistry, carpentry — are associated with elevated CTS rates. However, the relationship between office keyboard use and CTS is actually weaker than popular belief suggests; typing at neutral wrist postures does not substantially increase pressure in the carpal tunnel at typical workloads.
3. Anatomy of the Carpal Tunnel
The carpal tunnel is a rigid fibro-osseous canal at the base of the palm. Its floor and walls are formed by the carpal bones arranged in a concave arch: the scaphoid and trapezium radially, the hamate and pisiform ulnarly. The roof is the transverse carpal ligament (TCL), a thick fibrous band stretching between the medial and lateral bony prominences. This channel cannot expand in response to increased internal pressure — unlike fascial compartments elsewhere in the body, there is essentially no compliance.
The tunnel contains the median nerve and nine flexor tendons (the four flexor digitorum superficialis, four flexor digitorum profundus, and flexor pollicis longus tendons, each enclosed in their synovial sheaths). Normal carpal tunnel pressure is approximately 2–10 mmHg at rest. With wrist flexion or extension, pressure can spike to 30–90 mmHg; in patients with CTS, these pressures are substantially higher, impairing epineural blood flow and axonal transport within the nerve.
The median nerve provides sensory innervation to the palmar surface of the thumb, index, middle, and radial half of the ring finger, and motor innervation to the thenar muscles (abductor pollicis brevis, opponens pollicis, and the superficial head of flexor pollicis brevis). The abductor pollicis brevis is particularly important because thenar wasting — visible hollowing at the base of the thumb — indicates chronic, severe nerve compression that may not fully reverse even after surgical decompression.
4. Causes and Risk Factors
CTS is caused by anything that increases pressure within the carpal tunnel or decreases the nerve's tolerance for compression. The most important predisposing conditions include:
- Hypothyroidism — glycosaminoglycan deposits in the tendons and connective tissue enlarge the tunnel contents. CTS is present in 7–30% of hypothyroid patients and may be the presenting complaint before a thyroid diagnosis is established. Treating the hypothyroidism often improves CTS symptoms without other intervention.
- Diabetes mellitus — peripheral neuropathy increases median nerve vulnerability to compression; the two conditions co-exist in a phenomenon called the "double crush hypothesis." Diabetic patients have higher failure rates with conservative management.
- Pregnancy — fluid retention raises tunnel pressure; CTS affects up to 62% of pregnant women, typically developing in the second and third trimesters. It resolves spontaneously after delivery in the majority of cases, so conservative management is preferred during pregnancy.
- Rheumatoid arthritis — tenosynovial inflammation directly within the tunnel physically crowds the median nerve.
- Obesity — BMI is a significant independent risk factor; increased adiposity and higher fluid retention contribute to elevated tunnel pressure.
- Repetitive wrist use — sustained wrist postures in flexion or extension, particularly combined with forceful gripping, increase intracanal pressure and tendon sheath swelling.
- Acromegaly, amyloidosis, wrist fractures (especially distal radius fractures with carpal displacement), and space-occupying lesions (ganglia, lipomas) are less common but important causes in specific clinical contexts.
5. Clinical Presentation
The symptom pattern of CTS is distinctive enough that an experienced clinician can suspect the diagnosis strongly from the history alone, before any physical examination test or imaging is performed.
Sensory symptoms
The cardinal presenting symptoms are nocturnal paresthesias — tingling, numbness, or burning in the median nerve distribution (thumb, index, middle, radial ring finger) that wake the patient from sleep. This nocturnal predominance is thought to result from sustained wrist flexion during sleep, which maximizes carpal tunnel pressure, combined with the reduction in protective postural adjustments that occur during wakefulness. Patients characteristically describe shaking or "flicking" the wrist and hand to relieve symptoms — this is so specific to CTS that it was given a formal name, the flick sign, and has high diagnostic specificity.
As the condition progresses, daytime symptoms develop: tingling with sustained gripping (driving, holding a phone or book), difficulty with fine motor tasks (buttoning, handling coins), and dropping objects unexpectedly. Some patients describe the entire hand feeling numb, but careful questioning usually reveals the symptoms spare the little finger and ulnar half of the ring finger (ulnar nerve territory) — an important distinguishing feature.
Motor symptoms and thenar wasting
Weakness of thumb opposition and abduction develops in moderate to severe CTS. Thenar wasting — visible flattening or hollowing of the thenar eminence at the base of the thumb — indicates prolonged severe compression with axonal loss. At this stage, permanent motor deficit can occur even after successful decompression, making early intervention important for patients showing any motor involvement.
6. Diagnosis and Special Tests
Clinical examination tests
- Phalen's test. The patient holds both wrists in sustained maximum flexion (elbows extended, backs of hands touching) for 60 seconds. Onset of median nerve paresthesias within 60 seconds is positive. Sensitivity approximately 68–75%, specificity 47–80%.
- Tinel's sign. The examiner taps or percusses lightly over the median nerve at the wrist crease. A positive result is tingling or paresthesias radiating distally into the median nerve distribution. Sensitivity approximately 50–62%, specificity 55–77%.
- Durkan's (carpal compression) test. Direct thumb pressure over the carpal tunnel for 30 seconds reproducing symptoms; sensitivity approximately 87%, specificity 90% — somewhat better than either Phalen's or Tinel's in isolation.
- Thenar atrophy assessment. Wasting of the abductor pollicis brevis is a late finding indicating significant axonal loss and often prompts urgent surgical consideration.
Electrodiagnostic studies (NCS/EMG)
Nerve conduction studies (NCS) and electromyography (EMG) are the gold standard for objective confirmation of CTS diagnosis and severity grading. Key findings:
- Sensory NCS is the most sensitive. Prolonged sensory latencies or reduced sensory nerve action potential (SNAP) amplitudes across the wrist are the earliest electrodiagnostic abnormality in CTS, detectable before motor changes.
- Distal motor latency >4.5 ms to the abductor pollicis brevis indicates significant median motor conduction slowing.
- EMG denervation changes (fibrillations, positive sharp waves) in thenar muscles indicate axonal loss and predict less complete recovery after decompression.
Electrodiagnostic severity grading (mild: sensory only; moderate: sensory + motor slowing without axonal loss; severe: axonal loss/denervation) guides prognosis and surgical urgency. Importantly, a mildly abnormal NCS in an asymptomatic individual does not warrant treatment; conversely, a patient with classic clinical CTS but normal NCS may still have the condition — test sensitivity is approximately 85% for confirmed clinical CTS.
7. Conservative Treatment
Wrist splinting
Neutral-position wrist splinting is the first-line treatment for mild-to-moderate CTS. Splinting the wrist in a neutral position (0–15 degrees of extension) prevents the extreme flexion and extension postures that maximally elevate intracanal pressure. Nocturnal splinting is most important because it addresses the most common and disabling symptom. Full-time splinting adds daytime benefit but reduces compliance in working patients. A systematic review found splinting superior to no treatment and comparable to corticosteroid injection in short-term symptom relief for mild-to-moderate disease.
Corticosteroid injection
Injection of a corticosteroid (typically triamcinolone 40 mg or methylprednisolone 40 mg, combined with local anesthetic) into the carpal tunnel reduces tenosynovial swelling and provides meaningful symptom relief in 70–90% of patients. Duration of effect is limited: most patients experience benefit for 1–3 months, with approximately 50% maintaining relief at 6 months and declining benefit beyond 1 year. Injection is most useful to confirm the diagnosis, provide temporary relief during pregnancy (when surgery is deferred), or bridge patients to surgery.
Activity modification
Avoiding sustained wrist flexion, reducing forceful grip, modifying keyboard workstation ergonomics, and taking regular breaks reduce symptom burden in occupation-related CTS. These measures are adjuncts, not substitutes for primary treatment in moderate-to-severe disease.
8. Surgical Treatment
Carpal tunnel release (CTR) — surgical division of the transverse carpal ligament — is one of the most performed and most consistently successful operations in orthopedic and hand surgery, with patient satisfaction rates exceeding 90% in appropriately selected patients. Surgery is indicated for moderate-to-severe CTS that has failed 6–12 weeks of conservative management, for severe CTS with thenar wasting or EMG denervation (urgent indication to prevent permanent motor loss), for CTS with constant numbness, and by patient preference after failed conservative measures.
Open versus endoscopic release
Two surgical techniques are used:
- Open CTR — a 3–5 cm incision in the palm allows direct visualization of the TCL throughout its length before division. The traditional approach, highly reliable, and preferred for revision cases or complex anatomy. Main limitation: palmar scar tenderness ("pillar pain") lasting 2–4 months post-operatively.
- Endoscopic CTR — one or two small wrist/palm incisions with a camera allow TCL division under visualization without opening the full palm. Earlier return to function and work (approximately 2 weeks earlier than open), less palmar scar tenderness. Equivalent long-term outcomes to open CTR in meta-analyses, with a marginally higher risk of incomplete release in learning-curve surgeons.
Recovery
Most patients notice immediate improvement in nocturnal paresthesias after surgery, even before the wound heals. Full recovery of sensation and grip strength typically takes 3–6 months. Thenar wasting reverses partially but may not fully resolve in longstanding severe cases. Return to light activities in 1–2 weeks; heavy manual labor in 4–6 weeks. Recurrence after CTR is uncommon (<1% per year after initial success).
9. Outcomes and Special Populations
Pregnancy-associated CTS
CTS during pregnancy is managed conservatively with neutral wrist splinting as first-line treatment. Corticosteroid injection is used cautiously for severe or disabling symptoms. The majority of cases resolve spontaneously within 1–3 months of delivery as fluid retention and hormonal changes normalize. Surgery during pregnancy is reserved for patients with progressive motor weakness or permanent sensory loss.
Diabetic CTS
CTS in diabetic patients has higher rates of bilateral involvement, higher pre-operative NCS severity, and slower post-operative recovery. Glucose control does not reliably reverse established CTS but is an important modifier of peripheral nerve health. Surgical outcomes are generally good, though complete sensory recovery may be less complete than in non-diabetic patients.
Recurrence
True anatomic recurrence after complete CTR (reformation of the TCL) is rare. More common is persistent or recurrent symptoms from incomplete initial release, tenosynovial proliferation around an intact ulnar portion of the ligament, or development of perineural fibrosis. Revision surgery has lower success rates than primary release and is performed by hand surgery specialists.
10. References & Research
Key Research Papers
- Search PubMed — RCT of corticosteroid injection vs. splinting for CTS; injection superior short-term, outcomes converge at 1 year.
- Search PubMed — Cochrane review: endoscopic vs. open CTR; equivalent long-term outcomes, faster early functional recovery endoscopic.
- Search PubMed — Cochrane review: surgical vs. non-surgical for CTS; surgery produces better long-term relief.
- Search PubMed — Long-term outcomes: corticosteroid injection vs. surgical decompression; surgery superior at 1 year in moderate-to-severe disease.
- Search PubMed — Prevalence of CTS in the general population; estimated 3.8% after electrodiagnostic confirmation.
- Search PubMed — Comprehensive review of CTS pathophysiology, diagnosis, and management; widely cited overview article.
- Search PubMed — Prevalence of CTS during pregnancy: systematic review; up to 62% incidence in third trimester.
- Search PubMed — Predictors of CTR outcome; pre-operative factors affecting long-term functional results.
- CTS and hypothyroidism — PubMed search — Association between thyroid dysfunction and carpal tunnel syndrome.
- CTS and diabetes double-crush — PubMed search — Interaction between peripheral neuropathy and entrapment in diabetic patients.
- NCS/EMG diagnosis of CTS — PubMed search — Sensitivity and specificity of electrodiagnostic criteria.
- Wrist splinting for nocturnal CTS — PubMed search — Efficacy of neutral-position splinting for symptom control.
Research Papers
The links below run live searches on PubMed, the U.S. National Library of Medicine's database of biomedical literature.
- CTS treatment outcomes
- Carpal tunnel release surgery
- Median nerve NCS/EMG diagnosis
- CTS wrist splinting conservative
- Carpal tunnel corticosteroid injection
- CTS in pregnancy
- CTS and diabetes neuropathy
- CTS and hypothyroidism
- Endoscopic vs open carpal tunnel release
- CTS recurrence and revision surgery
- Phalen Tinel test sensitivity specificity
- CTS occupational risk factors
Connections
- Tendinitis — repetitive-use tendon inflammation that co-occurs with CTS in many occupational settings.
- Rotator Cuff Tear — another upper-extremity condition; double-crush neuropathy can involve cervical and peripheral components.
- Hypothyroidism — primary predisposing condition for CTS via glycosaminoglycan deposits in the tunnel; treatment often relieves CTS.
- Diabetes — peripheral neuropathy increases median nerve vulnerability; diabetic CTS has higher treatment failure rates.
- Rheumatoid Arthritis — tenosynovial inflammation within the carpal tunnel directly compresses the median nerve.
- Peripheral Neuropathy — overlapping symptoms; electrodiagnostic studies distinguish CTS from diffuse neuropathy.
- Orthopedics — full list of musculoskeletal and nerve conditions on this site.
- All Conditions — complete disease index.