Insomnia
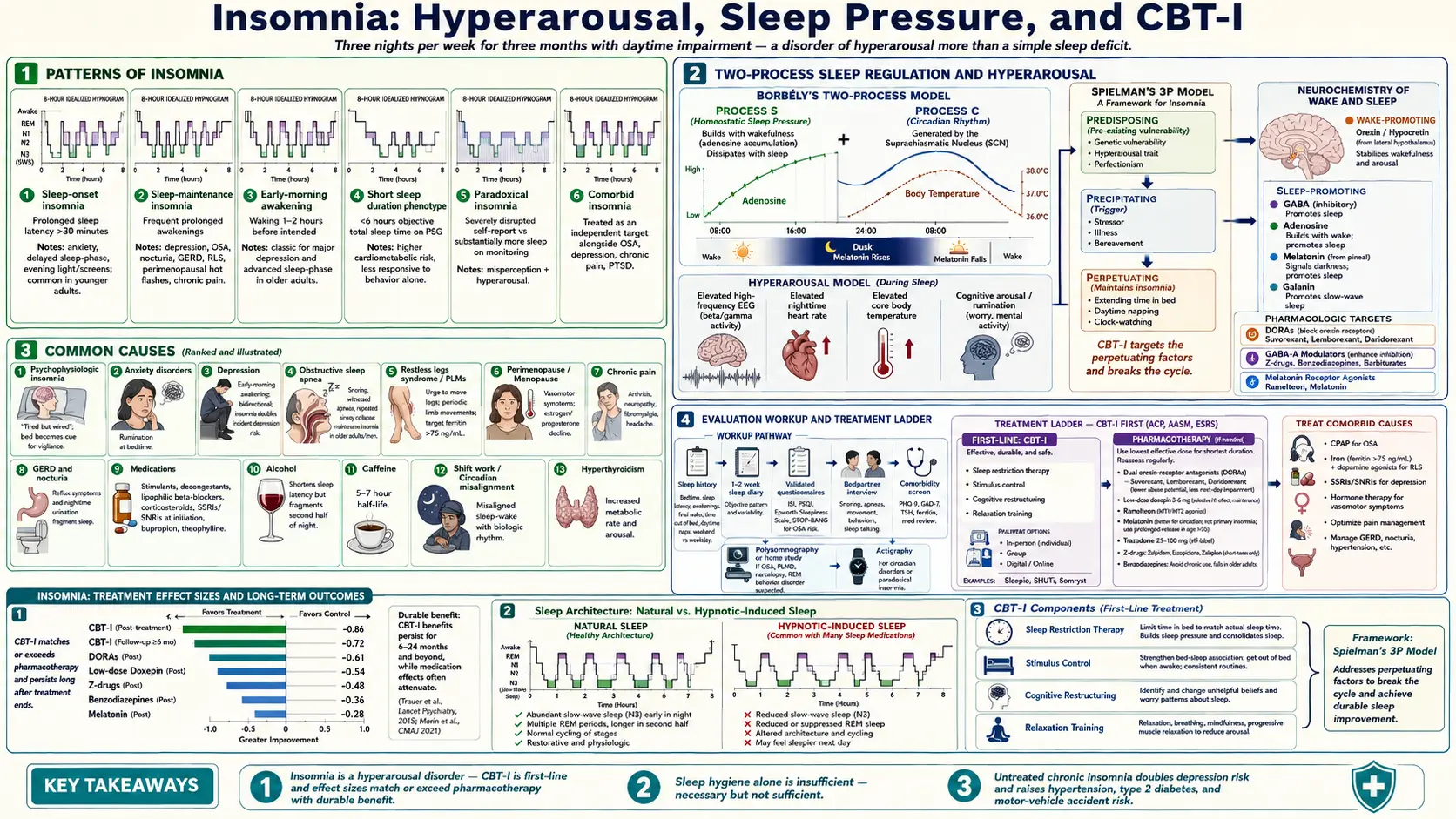


Table of Contents
- Pathophysiology: Hyperarousal Model
- Causes and Comorbidities
- Sleep Hygiene — Evidence and Limitations
- CBT-I: Gold Standard Treatment
- Pharmacotherapy
- Special Populations
- Comorbid Insomnia and Mental Health
- Sleep Study Indications and Evaluation
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Pathophysiology: Hyperarousal Model
Two-Process Model of Sleep
Normal sleep is governed by two competing biological systems. Process S (homeostatic sleep drive) builds progressively during wakefulness as adenosine accumulates in the brain, creating mounting pressure to sleep. Adenosine is released and cleared during sleep, resetting the drive for the next waking period. Caffeine works precisely by blocking adenosine receptors, pharmacologically erasing Process S pressure. Process C is the circadian alerting signal, generated by the suprachiasmatic nucleus (SCN) of the hypothalamus. The SCN receives light signals via the retinohypothalamic tract, which suppresses melatonin secretion from the pineal gland during daylight hours. The circadian signal peaks twice daily — in the early morning and again in the early evening (the “forbidden zone” for sleep) — creating windows of heightened wakefulness that oppose sleep even when Process S is elevated. Insomnia arises when one or both of these systems malfunction, or when external and psychological forces override them.
Hyperarousal Theory
The most empirically supported framework for chronic insomnia is the hyperarousal model. People with chronic insomnia show objectively elevated arousal across multiple biological domains: elevated heart rate and heart-rate variability abnormalities; elevated urinary cortisol and catecholamines at night; higher core body temperature at sleep onset; and — most distinctively — EEG showing increased beta wave (16–30 Hz) power during sleep, the same high-frequency activity that characterizes wakefulness. In addition to this physiologic hyperarousal, cognitive arousal (racing thoughts, worry about not sleeping, monitoring for sleep-related threats) and emotional arousal compound the problem. This is why sedative-hypnotics that force sleep do not eliminate the underlying disorder: the hyperarousal substrate remains.
Conditioned Arousal
A critical perpetuating mechanism is classical conditioning. After enough nights of lying awake in bed, the bed and bedroom become conditioned stimuli for wakefulness rather than sleep. The same person who falls asleep effortlessly on a couch is instantly alert when they get into bed. This conditioned arousal forms the rationale for stimulus control therapy, a core CBT-I component: the bed must be re-associated with sleep by spending time in bed only when sleepy and leaving when awake.
Spielman's 3P Model
Arthur Spielman's predisposing–precipitating–perpetuating (3P) model explains why most people recover from a sleepless night but some develop lifelong chronic insomnia. Predisposing factors include genetic hyperarousal trait, perfectionism, tendency toward internalizing stress, and female sex (women have 40–50% higher lifetime risk). A precipitating event — job loss, bereavement, illness, relationship breakdown, a shift in work schedule — launches the acute episode. Most people then recover. Those who develop chronic insomnia accumulate perpetuating behaviors: extending time in bed to “catch up,” daytime napping, canceling evening plans to rest, watching the clock at 3 AM, and developing anticipatory anxiety about whether tonight will be another bad night. CBT-I is designed to systematically dismantle these perpetuating behaviors.
By definition, ICSD-3 chronic insomnia disorder requires sleep difficulty on at least three nights per week for at least three months, with adequate opportunity for sleep, causing meaningful daytime impairment (fatigue, mood disturbance, cognitive difficulty, or occupational/social dysfunction). Prevalence in the general population is 10–30%, with a chronic disorder rate of approximately 10%. Short-term insomnia (fewer than three months) is usually stressor-related and most cases resolve spontaneously when the stressor passes.
Causes and Comorbidities
Acute Insomnia
Situational insomnia is nearly universal and requires no treatment beyond time. Job loss, divorce, grief, travel across time zones, a new infant, noise, temperature, and unfamiliar environments all reliably disrupt sleep. The distinction between situational and chronic insomnia is duration and perpetuating behavior, not the trigger itself. When the precipitant resolves and the sleeplessness persists, the diagnosis shifts to chronic insomnia disorder and treatment becomes appropriate.
Comorbid Insomnia
Most clinical insomnia occurs alongside another condition. The previous paradigm of “secondary insomnia” — wait for the primary condition to improve and sleep will follow — has been abandoned. Insomnia should now be treated as an independent target regardless of what else is present.
- Major depression — the most common psychiatric comorbidity. Depression characteristically causes early-morning awakening plus difficulty initiating sleep. Critically, insomnia frequently precedes the onset of depression by weeks and is often the first symptom patients report. Screening with the PHQ-9 is essential. Treating insomnia independently (not just waiting for the antidepressant to work) accelerates mood recovery.
- Anxiety disorders — racing thoughts, anticipatory worry, and cognitive hyperarousal are primary drivers of sleep-onset insomnia. Generalized anxiety disorder and panic disorder are particularly common comorbidities.
- PTSD — nightmares and hypervigilance create both maintenance insomnia and sleep-onset insomnia. Insomnia in PTSD is a distinct treatment target with specific evidence-based options.
- Chronic pain — musculoskeletal pain, fibromyalgia, and neuropathic pain lower the arousal threshold and disrupt sleep architecture throughout the night. Pain and poor sleep are mutually amplifying.
- Heart failure — orthopnea, paroxysmal nocturnal dyspnea, nocturia, and Cheyne-Stokes respirations fragment sleep. OSA is highly prevalent in heart failure, further compounding the problem.
- COPD — nocturnal hypoxemia, dyspnea, and the activating effects of beta-agonists and corticosteroids all disrupt sleep.
- GERD — supine posture worsens acid reflux; nocturnal acid events cause microarousals that patients may not recall consciously.
- Hyperthyroidism — elevated thyroid hormone increases resting heart rate, core temperature, and cognitive arousal — all hyperarousal amplifiers.
- Dementia — sundowning (late-afternoon and evening agitation) and circadian fragmentation are early features of Alzheimer's and other dementias.
- Menopause — vasomotor symptoms (hot flashes) fragment sleep most severely in the year following final menstrual period; they may persist for 7–10 years.
- Advanced CKD — restless legs syndrome is especially prevalent (prevalence 20–30% in ESRD), and uremia itself is directly arousing.
Substances and Medications
- Caffeine — half-life 5–7 hours; a 3 PM coffee still has meaningful caffeine activity at 9–10 PM. The “6 PM cutoff” is too late for many sensitive individuals. Some people metabolize caffeine slowly (CYP1A2 variants) and need to stop by noon.
- Alcohol — counterintuitively, alcohol is both a sleep aid and a sleep destroyer. It shortens sleep latency (which patients interpret as helpfulness) but suppresses REM sleep, fragments the second half of the night, and causes rebound arousal as it is metabolized.
- Beta-blockers — suppress melatonin secretion via beta-1 and beta-2 receptors on the pineal gland; lipophilic agents (propranolol, metoprolol) cross the blood-brain barrier and cause nightmares more than hydrophilic agents (atenolol).
- Corticosteroids — a single evening dose of prednisone can cause profound insomnia; morning or lunchtime dosing is the clinical workaround.
- Decongestants — pseudoephedrine has significant sympathomimetic arousal effects; commonly overlooked as an insomnia cause.
- SSRI/SNRI antidepressants — activating effects (especially at initiation) can worsen insomnia transiently; vivid dreams and REM behavior disorder are known side effects; typically improve after 1–2 weeks.
- Bupropion — dopaminergic and noradrenergic activation; avoid evening dosing; one of the most reliably activating antidepressants.
- Theophylline — adenosine antagonist (similar mechanism to caffeine); tachycardia and arousal at therapeutic serum levels.
Sleep Hygiene — Evidence and Limitations
Standard Sleep Hygiene Recommendations
- Consistent sleep/wake time — the most powerful single behavioral habit. The rise time is the circadian anchor; irregular timing fragments the Process C signal and undermines sleep quality even when total sleep time is preserved. This means weekends too.
- Dark, cool, quiet sleep environment — the optimal core body temperature for sleep onset is approximately 65–68°F (18–20°C) for most adults. Even small amounts of light — a phone charging LED, streetlight through thin curtains — suppress melatonin. Blackout curtains make a measurable difference.
- Limit screens 60 minutes before bed — blue light in the 460–480 nm wavelength range is most potent at suppressing melatonin via intrinsically photosensitive retinal ganglion cells. But the cognitive activation from content (news, social media, emotionally engaging video) is at least as disruptive as the light itself. Blue-light filtering glasses reduce the photonic component but do nothing for the content component.
- Avoid caffeine after 2 PM — or earlier for slow metabolizers. The afternoon coffee that “doesn’t affect me” may still be raising arousal at midnight through adenosine receptor blockade without the conscious subjective effect.
- Avoid alcohol near bedtime — two drinks before bed may shorten sleep latency by 10 minutes while wrecking slow-wave and REM architecture and causing early-morning awakening. Patients who rely on alcohol to sleep are treating conditioned arousal with a substance that worsens long-term sleep quality.
- Exercise — regular aerobic exercise improves sleep quality by strengthening both Process S (greater metabolic adenosine load) and Process C (morning light exposure during outdoor exercise). High-intensity exercise within 2–3 hours of sleep may delay sleep onset in some individuals due to post-exercise elevation in core temperature and catecholamines.
- Bed only for sleep and sex — the stimulus control principle: watching TV, working, eating, or scrolling in bed teaches the brain that bed is a place for wakefulness.
- Only get into bed when sleepy — going to bed “at 10 PM” regardless of subjective sleepiness, then lying awake frustrated, is a powerful conditioning trial for arousal. Wait for genuine sleepiness (heavy eyelids, nodding, yawning).
- Remove clocks from view — clock-watching at 2:30 AM triggers mental arithmetic about how many hours of sleep remain, which reliably increases cortisol and defeats sleep.
- Limit naps to 20 minutes before 3 PM — napping depletes Process S homeostatic pressure, making nighttime sleep harder to initiate.
Evidence Reality Check
Sleep hygiene alone is insufficient for established chronic insomnia. Multiple randomized trials confirm that sleep hygiene education as a monotherapy produces only modest, non-durable improvement. This is a critical clinical point: telling a patient with three-year insomnia to put their phone down at 9 PM is analogous to telling a hypertensive patient to reduce sodium without offering medication — correct but inadequate. Sleep hygiene is a necessary component of good sleep medicine, but chronic insomnia is a neurobiological disorder of hyperarousal that requires more than behavioral tidying. CBT-I is the real first-line treatment; sleep hygiene is one of its five components.
CBT-I: Gold Standard Treatment
Cognitive Behavioral Therapy for Insomnia (CBT-I) is unanimously endorsed as the first-line treatment for chronic insomnia by the American Academy of Sleep Medicine (AASM), the American College of Physicians (ACP, 2016 guideline), and the European Sleep Research Society. Its superiority over pharmacotherapy lies not only in comparable acute efficacy but in durable benefit: gains persist after treatment ends, whereas pharmacotherapy requires indefinite use to maintain effect. CBT-I is typically delivered in 4–8 sessions with a trained therapist, in group format, or via digital therapeutics.
Components of CBT-I
- 1. Stimulus Control Therapy — the most powerful single component. Go to bed only when genuinely sleepy. If you are in bed and awake for more than approximately 20 minutes, get out of bed, go to another room, and engage in a quiet non-stimulating activity (reading under dim light, light stretching, slow music) until sleepiness returns, then return to bed. Repeat as needed. This systematically breaks the conditioned bed–arousal association and re-establishes the bed as a cue for sleep. This instruction is initially very difficult for patients because it goes against the instinct to stay in bed and try harder.
- 2. Sleep Restriction Therapy — prescribed total time in bed is initially restricted to the patient’s estimated actual sleep time, as recorded in a sleep diary. If a patient spends 9 hours in bed but sleeps only 5.5 hours (sleep efficiency 61%), their initial prescribed time in bed is 5.5 hours (e.g., midnight to 5:30 AM). This rapidly builds homeostatic sleep pressure (Process S), consolidates sleep, and increases sleep efficiency. As efficiency reaches 85–90%, the sleep window is extended by 15–30 minutes. Patients experience short-term worsening of sleepiness before improvement — they must be warned explicitly. Sleep restriction is counterintuitive but among the most robustly effective components of CBT-I.
- 3. Relaxation Training — progressive muscle relaxation (systematic tension and release of major muscle groups), diaphragmatic breathing, biofeedback, and guided imagery reduce somatic arousal and physiologic tension. Targets the autonomic hyperarousal component of the disorder.
- 4. Cognitive Therapy — identification and restructuring of dysfunctional beliefs about sleep. Common examples: “I must get exactly 8 hours or I’ll be useless tomorrow” (catastrophizing); “I haven’t had a good night’s sleep in 10 years” (overgeneralization); “I have no control over my sleep” (helplessness). These beliefs amplify arousal and perpetuate the disorder. Mindfulness-based approaches that reduce sleep-related monitoring and increase acceptance of sleep variability are also effective.
- 5. Sleep Hygiene Education — as above; necessary adjunct but not the driver of improvement in CBT-I outcomes.
Digital CBT-I
Access to trained CBT-I therapists is severely limited. Digital CBT-I programs fill this gap with good evidence. Somryst is the only FDA-cleared prescription digital therapeutic for chronic insomnia (de novo 510(k) clearance, 2020). Sleepio has strong randomized trial evidence and is recommended by NHS England. SHUTi (Sleep Healthy Using the Internet) has been validated in multiple academic trials. These programs deliver full CBT-I including sleep restriction, stimulus control, cognitive restructuring, and relaxation, adapted for self-paced digital delivery. Meta-analyses confirm efficacy comparable to face-to-face delivery.
Pharmacotherapy
Medication is appropriate when CBT-I is unavailable, refused, or incompletely effective; when acute insomnia is causing significant functional impairment; or as a bridge during the initial weeks of CBT-I before behavioral techniques take hold. All medications for insomnia should be prescribed at the lowest effective dose and reassessed regularly.
Orexin Antagonists (Preferred First-Line Medications)
Three dual orexin-receptor antagonists (DORAs) are FDA-approved for insomnia: suvorexant (Belsomra, 2014), lemborexant (Dayvigo, 2019), and daridorexant (Quviviq, 2022). These agents block the wake-promoting orexin (hypocretin) peptide system rather than globally suppressing CNS activity. The result is sleep that more closely preserves natural sleep architecture, lower risk of respiratory depression, less cognitive and psychomotor impairment, and lower abuse and dependence potential compared to benzodiazepines and Z-drugs. They are particularly effective for sleep-maintenance insomnia. Key caveats: next-morning motor impairment at higher doses (particularly with suvorexant 20mg); cost (no generics); rare complex sleep behaviors. FDA-recommended starting dose for lemborexant is 5mg (maximum 10mg); daridorexant starts at 25mg (maximum 50mg).
Z-Drugs (Non-Benzodiazepine GABA-A Modulators)
Zolpidem (Ambien), eszopiclone (Lunesta), and zaleplon (Sonata) bind GABA-A receptors with selectivity for the alpha-1 subunit (compared to the less selective benzodiazepines), producing sedation. Zolpidem remains the most prescribed hypnotic in the US. Risks include: complex sleep behaviors (sleepwalking, sleep driving, sleep eating — FDA black-box warning; rare but potentially dangerous; reported even at therapeutic doses); next-morning impairment (especially extended-release formulations); tolerance; rebound insomnia on discontinuation. Women and the elderly require lower doses: women metabolize zolpidem more slowly (FDA recommended dose 5mg for women vs. 10mg for men, or 3.75mg/7.5mg for CR formulation). Zaleplon’s ultra-short half-life (~1 hour) makes it uniquely useful for middle-of-night awakening (taken when waking at 3 AM with at least 4 hours of sleep remaining).
Benzodiazepines
Temazepam, triazolam, and estazolam are FDA-approved for insomnia. They are effective for short-term use (2–4 weeks) but carry a significant risk profile for chronic use: tolerance (requiring dose escalation), physical dependence, next-day sedation, anterograde amnesia, falls and hip fractures (especially in elderly), and cognitive impairment with chronic use. Avoid in older adults (Beers Criteria: high-risk medication in adults 65+). Avoid in obstructive sleep apnea (respiratory depression worsens hypoxemia). Avoid in any history of substance use disorder.
Low-Dose Doxepin (3–6 mg)
At these ultra-low doses, doxepin acts as a highly selective histamine H1 antagonist without meaningful anticholinergic effects at typical tricyclic doses. FDA-approved for sleep-maintenance insomnia. Particularly useful in older adults where DORAs may be cost-prohibitive and benzodiazepines/Z-drugs are contraindicated. The evidence base at 3–6 mg doses is solid, with robust randomized trial data.
Ramelteon
Ramelteon is a melatonin MT1/MT2 receptor agonist with FDA approval for sleep-onset insomnia. It has no abuse potential and is not a scheduled substance — a significant advantage in patients with substance use histories. Effect size is modest for primary insomnia but more meaningful for circadian rhythm disorders. Safe in elderly patients. Often used in long-term care settings where benzodiazepines are especially dangerous.
Melatonin
Melatonin’s primary indication is circadian rhythm disorders (jet lag, delayed sleep phase syndrome, shift work), not primary insomnia. Timing matters more than dose: physiological doses (0.5–3 mg) taken at dusk (7–9 PM) advance the circadian phase and improve sleep onset in delayed sleep phase. The OTC doses commonly available in the US (3–10 mg taken at bedtime) are pharmacological rather than physiological and have limited evidence for primary insomnia. The melatonin supplement market is poorly regulated — a 2017 analysis found actual content ranged from 83% below to 478% above the labeled dose.
Trazodone
Trazodone (25–150 mg at bedtime) is the most widely prescribed off-label hypnotic in the US, despite modest evidence in primary insomnia. Its sedating properties arise from histamine H1 and alpha-1 adrenergic blockade. Advantages: no abuse potential, useful in patients with concurrent depression or anxiety, inexpensive generic, and no respiratory depression. Key adverse effect to counsel: priapism (rare, approximately 1 in 6,000, but a urological emergency; men must be counseled to seek immediate care for erection lasting >4 hours).
Special Populations
Older Adults
Several normal age-related changes in sleep architecture are frequently misidentified as insomnia and should not be treated: earlier sleep phase (older adults become sleepy earlier in the evening and wake earlier — advanced sleep phase tendency); more fragmented sleep with more time in lighter NREM stages (N1, N2); reduced slow-wave (N3) sleep; and slightly shorter total sleep time. These changes are physiologic and do not require intervention unless they cause significant distress or dysfunction.
When genuine insomnia disorder is present in older adults: CBT-I remains first-line and has been validated in multiple trials in this age group with excellent results. For pharmacotherapy, avoid benzodiazepines and Z-drugs (Beers Criteria high-risk; falls and hip fractures are a leading cause of morbidity and mortality in older adults; cognitive impairment worsens dementia risk). Preferred medications: low-dose doxepin (3–6 mg), ramelteon, and orexin antagonists at low doses. OSA is underdiagnosed in elderly patients and should be screened for before treating insomnia pharmacologically.
Pregnancy
Sleep disturbance affects 70–80% of pregnant women, particularly in the third trimester (positional discomfort, heartburn, fetal movement, frequent urination, leg cramps). CBT-I is first-line and safe throughout pregnancy. Avoid benzodiazepines, especially in the first trimester (associated with increased risk of oral cleft; withdrawal in the neonate). Melatonin has limited safety data in pregnancy (animal studies show neurological effects at high doses; human data insufficient). If a hypnotic is judged necessary, diphenhydramine (Benadryl) is the most commonly used option, but it should be used sparingly and for short durations.
Shift Workers
Shift work sleep disorder is defined as insomnia or excessive sleepiness caused by a work schedule that conflicts with the circadian system — rotating shifts, permanent night shifts, and early-morning starts. Management is multifaceted: melatonin (taken at the target new bedtime, not the clock time) for circadian advancement; strategic bright-light exposure at the appropriate circadian phase (light is the most powerful zeitgeber); and modafinil or armodafinil (FDA-approved for shift work disorder) for alertness during the work shift. Blackout curtains, earplugs, and family/social schedule adjustments are essential non-pharmacologic supports.
Adolescents and Teens
A biological shift toward a later chronotype is normal in puberty and early adulthood, mediated by delayed melatonin onset. This means a 16-year-old who cannot fall asleep until midnight is often experiencing a physiologic delayed sleep phase, not behavioral defiance. When school start times require waking at 6–7 AM, the result is chronic sleep restriction. Distinguishing physiologic delayed phase from behavioral sleep restriction (late-night phones, social media, gaming) requires a sleep diary. Modified CBT-I for adolescents is effective; strategic morning light exposure helps phase-advance. The American Academy of Pediatrics has formally recommended that middle and high schools not start before 8:30 AM to align with adolescent biology.
Comorbid Insomnia and Mental Health
Insomnia and Depression: Bidirectional Risk
The relationship between insomnia and depression is not hierarchical (depression causes insomnia) but bidirectional. Chronic insomnia approximately doubles the lifetime risk of developing a major depressive episode, independent of all other risk factors. Insomnia is frequently the first symptom of an emerging depressive episode, appearing weeks before mood changes. This makes insomnia an important target for early depression prevention. Conversely, depression — especially melancholic depression — causes distinctive early-morning awakening. The clinical implication: treat insomnia and depression as independent targets simultaneously rather than waiting for one to improve the other.
PTSD and Insomnia
In PTSD, insomnia arises from multiple mechanisms: trauma-related nightmares (REM dysregulation), hypervigilance maintaining cortical arousal at night, and hyperstartle responses causing microarousals. Two evidence-based treatments exist for PTSD-related nightmares that are distinct from standard insomnia treatment:
- Prazosin — an alpha-1 adrenergic receptor blocker originally used for hypertension. Supported by VA/DoD clinical practice guidelines for PTSD nightmares. Reduces nightmare frequency, nightmare intensity, and sleep-disrupting arousal. Starting dose 1 mg at bedtime; typical therapeutic dose 5–15 mg. The 2018 NEJM trial by Raskind and colleagues (the largest prazosin RCT in military veterans) showed robust reduction in nightmare frequency and PTSD severity. Key side effect: orthostatic hypotension — titrate slowly.
- Image Rehearsal Therapy (IRT) — a cognitive technique for recurring nightmares. The patient selects a recurring nightmare, rewrites it with a different (non-threatening) ending during the day, and rehearses the new version daily. After 3–5 IRT sessions, nightmare frequency and distress typically decrease substantially. IRT is the best-evidenced behavioral treatment for PTSD nightmares and is endorsed by the AASM.
Anxiety Disorders
CBT-I is effective for comorbid insomnia and anxiety disorders. The stimulus control and sleep restriction components directly address the anticipatory anxiety and hyperarousal that drive sleep-onset insomnia in anxious patients. Cognitive restructuring in CBT-I overlaps extensively with cognitive techniques for generalized anxiety disorder, making the treatments synergistic. Benzodiazepines should be used cautiously in anxiety-comorbid insomnia due to dependence risk; DORAs and CBT-I are preferred.
Bipolar Disorder
Sleep disruption is both a prodromal sign and a trigger for manic episodes in bipolar disorder. A patient with bipolar disorder who develops insomnia may be entering hypomania — an important clinical distinction from primary insomnia. Sleep restriction therapy (a core CBT-I component) requires caution in bipolar disorder because building homeostatic sleep debt can precipitate hypomania or mania. If sleep restriction is used, it should be implemented gradually and under mood stabilizer coverage, in coordination with the patient’s psychiatric care provider.
Sleep Study Indications and Evaluation
Polysomnography (In-Lab)
Full polysomnography (PSG) involves multichannel recording of EEG, electrooculography (EOG), chin and leg EMG, ECG, oronasal airflow, respiratory effort belts, pulse oximetry, body position, and video. PSG is not routinely indicated for the diagnosis of primary insomnia — insomnia is a clinical diagnosis made from history. PSG is indicated when:
- Obstructive sleep apnea is suspected (snoring; witnessed apneas; obesity; neck circumference >17 inches in men, >16 inches in women; STOP-BANG score ≥3).
- Narcolepsy is suspected (cataplexy, sleep paralysis, hypnagogic hallucinations, excessive daytime sleepiness regardless of night sleep). PSG is followed by a multiple sleep latency test (MSLT) the next day, which documents pathologically short sleep latency and sleep-onset REM periods.
- Periodic limb movement disorder requires objective documentation.
- REM sleep behavior disorder (acting out dreams, often violently) must be monitored and distinguished from other parasomnias.
- Insomnia fails to respond to adequate CBT-I and adequate pharmacotherapy — ruling out occult OSA or PLMD.
Home Sleep Apnea Testing (HSAT)
Home sleep apnea tests (Watch-PAT, ApneaLink, ResMed device) measure oximetry, respiratory effort, heart rate, and body position. They are validated and cost-effective for high-pretest-probability OSA in otherwise healthy adults without significant comorbidities. HSAT is not appropriate when central sleep apnea, complex medical illness, or other sleep disorders (narcolepsy, RLS) are suspected alongside OSA.
Actigraphy
Wrist actigraphy uses accelerometry to estimate sleep–wake cycles over days to weeks. It is particularly useful for: mapping actual circadian patterns in shift workers or delayed sleep phase; objectively tracking the sleep window during CBT-I sleep restriction; and diagnosing circadian rhythm disorders (advanced and delayed sleep phase, non-24-hour rhythm disorder in blind individuals). Insurance coverage for actigraphy is increasing for circadian disorder indications. Actigraphy cannot replace PSG and cannot diagnose OSA or PLMD.
Sleep Diary
The two-week prospective sleep diary is the cornerstone of insomnia assessment and CBT-I delivery. Patients record bedtime, estimated sleep latency, number and duration of nocturnal awakenings, final wake time, time out of bed, and subjective sleep quality each morning. From this, the clinician or digital program calculates: average total sleep time, average sleep efficiency (total sleep time / time in bed × 100%), and sleep-schedule variability. The initial CBT-I sleep window is set based on the diary-derived average sleep time. Diaries are also used to track treatment response over the course of CBT-I.
Validated Questionnaires
- Insomnia Severity Index (ISI) — 7-item self-report; scores 0–28; a score ≥15 indicates moderate to severe insomnia disorder; widely used as a primary outcome measure in clinical trials and as a treatment-response tracker.
- Pittsburgh Sleep Quality Index (PSQI) — assesses seven sleep domains over the past month; global score >5 indicates poor sleep quality; useful as a broad screen but less sensitive to treatment changes than the ISI.
- Epworth Sleepiness Scale (ESS) — measures daytime sleepiness across eight common situations; scores ≥11 suggest pathological sleepiness and should prompt workup for OSA or narcolepsy rather than primary insomnia (which typically causes fatigue but not pathological sleepiness).
- STOP-BANG — Snoring, Tired, Observed apneas, Pressure (hypertension), BMI >35, Age >50, Neck >40 cm, Gender (male); score ≥3 indicates intermediate-to-high risk of OSA; essential initial screen when maintenance insomnia is present.
When to Seek Medical Care
- Sleep difficulty present three or more nights per week for more than three months with daytime impairment.
- Loud snoring, witnessed apneas, gasping awakenings, or unrefreshing sleep despite adequate time in bed (consider OSA).
- Depression, hopelessness, or thoughts of self-harm or suicide.
- Acting out of dreams, sleepwalking, or other parasomnia behaviors that pose a safety risk.
- Excessive daytime sleepiness with episodes of falling asleep at the wheel or during conversations (consider narcolepsy or severe OSA).
- Sudden worsening of insomnia in older adults — can herald depression, dementia, delirium, or a new medical illness.
- Evening leg discomfort relieved by movement (restless legs syndrome).
- Insomnia tied to a new medication, dose change, or substance (alcohol, cannabis, stimulants).
Connections
- Depression
- Anxiety
- Chronic Pain
- Obstructive Sleep Apnea
- Fatigue
- Fibromyalgia
- Magnesium
- Brain Fog
- Heart Palpitations
- Hashimoto's Thyroiditis
- Graves' Disease
- Insomnia (Psychiatry)
- Sleep Hygiene
- Headache
- PTSD
- Hormone Panel
- Lemon Balm
- Adrenal Fatigue
References & Research
Historical Background
Insomnia has been described for as long as medicine has been written. Hippocrates noted that sleep disturbance accompanied many illnesses and that prolonged sleeplessness foreshadowed worsening disease. For most of the twentieth century, insomnia was treated as a symptom of psychiatric or medical disease rather than a disorder in its own right, and pharmacotherapy with barbiturates and later benzodiazepines was the dominant approach. The intellectual turning point came in 1973, when Arthur Spielman began developing the sleep restriction technique that would become a pillar of modern behavioral treatment, followed by his 3P model of predisposing, precipitating, and perpetuating factors. Through the 1980s and 1990s, Charles Morin, Richard Bootzin (stimulus control), and others assembled these techniques into cognitive behavioral therapy for insomnia (CBT-I). The International Classification of Sleep Disorders, Third Edition (ICSD-3), published in 2014, established the modern formal definition of chronic insomnia disorder and moved away from the old “secondary insomnia” framework, recognizing insomnia as an independent diagnostic target. The first orexin-receptor antagonist, suvorexant, received FDA approval in 2014, marking the first new pharmacologic mechanism for insomnia in decades, and was followed by lemborexant (2019) and daridorexant (2022). The 2016 American College of Physicians guideline formally elevated CBT-I to first-line treatment for chronic insomnia, a position reinforced by the 2021 AASM behavioral treatment guideline and reflected in every major international clinical guideline today.
Key Research Papers
- Morin CM, Benca R. Chronic insomnia. Lancet. 2012;379(9821):1129–1141.
- Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. Management of chronic insomnia disorder in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016;165(2):125–133.
- Sateia MJ. International classification of sleep disorders — third edition: highlights and modifications. Chest. 2014;146(5):1387–1394.
- Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675–700.
- Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an AASM clinical practice guideline. J Clin Sleep Med. 2021;17(2):255–262.
- Herring WJ, Connor KM, Snyder E, et al. Suvorexant in patients with insomnia: results from two 3-month randomized controlled clinical trials. Biol Psychiatry. 2016;79(2):136–148.
- Rosenberg R, Murphy P, Zammit G, et al. Comparison of lemborexant with placebo and zolpidem tartrate extended release for the treatment of older adults with insomnia disorder. JAMA Netw Open. 2019;2(12):e1918254.
- Mignot E, Mayleben D, Fietze I, et al. Safety and efficacy of daridorexant in patients with insomnia disorder: results from two multicentre, randomised, double-blind, placebo-controlled, phase 3 trials. Lancet Neurol. 2022;21(2):125–139.
- Spielman AJ, Saskin P, Thorpy MJ. Treatment of chronic insomnia by restriction of time in bed. Sleep. 1987;10(1):45–56.
- Krystal AD, Durrence HH, Scharf M, et al. Efficacy and safety of doxepin 1 mg, 3 mg, and 6 mg in adults with primary insomnia. Sleep. 2010;33(11):1553–1561.
- Raskind MA, Peskind ER, Chow B, et al. Trial of prazosin for post-traumatic stress disorder in military veterans. N Engl J Med. 2018;378(6):507–517.
- Kryger MH, Roth T, Dement WC. Principles and Practice of Sleep Medicine. 6th ed. Elsevier; 2017. [Reference textbook — no DOI; standard reference in sleep medicine]
PubMed Topic Searches
- Chronic insomnia disorder
- Cognitive behavioral therapy for insomnia (CBT-I)
- Hyperarousal in insomnia
- Orexin-receptor antagonists for insomnia
- Sleep restriction therapy
- Insomnia and depression: bidirectional risk
- Insomnia in special populations
- PTSD nightmares and prazosin