Hyperthyroidism
If your thyroid is making too much hormone, your body's "engine" runs too fast. Hyperthyroidism (an overactive thyroid) can cause a racing heart, unexplained weight loss, shakiness, anxiety, and trouble sleeping — symptoms that are easy to mistake for stress or a heart problem. The good news is that hyperthyroidism is very treatable, and most people feel dramatically better once the diagnosis is made and treatment begins. This page explains what hyperthyroidism is, what causes it, how doctors test for it, and the main treatment options — in plain language, but grounded in major medical guidelines. It is health information, not a substitute for your own doctor's advice.
Interactive Visualization How Your Thyroid Is Controlled — run the feedback loop Watch TSH drive the thyroid, T4 convert to T3, and the loop feed back — then switch on Hashimoto's, Graves', or iodine deficiency. Launch →
Table of Contents
- What Hyperthyroidism Is
- Symptoms
- Causes
- Diagnosis
- Treatment
- Thyroid Storm — The Emergency
- When to See a Doctor & Living With It
- Research Papers
- Connections
- Featured Videos
What Hyperthyroidism Is
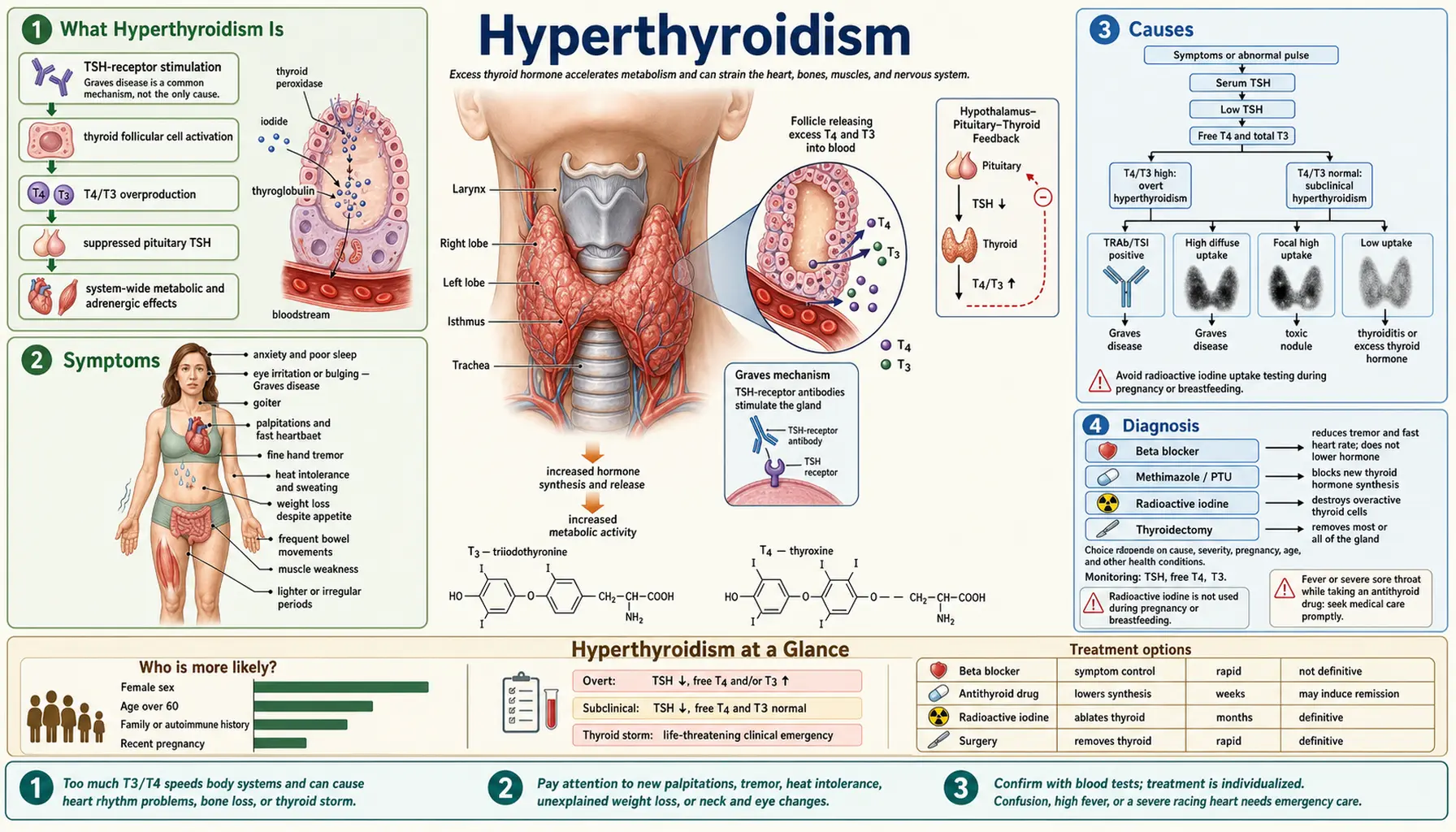
Your thyroid is a small, butterfly-shaped gland in the front of your neck. It makes hormones — mostly thyroxine (T4) and triiodothyronine (T3) — that set the pace of your metabolism, the speed at which nearly every cell in your body uses energy. In hyperthyroidism, the gland makes too much hormone, so your metabolism runs faster than it should. Your heart beats quicker, you burn through calories, and your nervous system runs "hot."
To understand the blood tests, it helps to know the feedback loop. Your pituitary gland (in your brain) releases TSH (thyroid-stimulating hormone), which tells the thyroid how hard to work. When thyroid hormone levels rise too high, the pituitary senses it and turns TSH down to try to slow the gland. So in hyperthyroidism the classic pattern is a LOW (suppressed) TSH with HIGH free T4 and/or T3. This is the mirror image of hypothyroidism (underactive thyroid), where TSH is high and thyroid hormone is low.
Doctors describe two levels of severity. In overt hyperthyroidism, TSH is low and the thyroid hormones (free T4 and/or T3) are clearly high. In subclinical hyperthyroidism, TSH is low but the thyroid hormone levels are still within the normal range — an early or mild form that may cause few symptoms but can still affect the heart and bones over time, especially in older adults. Hyperthyroidism is real and important, but it is worth knowing that it is less common than hypothyroidism; an underactive thyroid is the far more frequent thyroid problem.
Symptoms
Because metabolism is sped up, the symptoms tend to be ones of "too much, too fast." Common ones include:
- Unintentional weight loss — often despite a normal or even increased appetite, because the body is burning energy faster.
- A rapid, pounding, or irregular heartbeat (palpitations) — sometimes the first thing people notice.
- Heat intolerance and increased sweating — feeling hot when others are comfortable.
- Anxiety, nervousness, or irritability — a "wired," on-edge feeling.
- A fine tremor — usually a subtle shaking of the hands or fingers.
- More frequent bowel movements (not always diarrhea, just more often).
- Trouble sleeping and feeling restless or unable to wind down.
- Muscle weakness, often in the thighs and upper arms (for example, difficulty climbing stairs).
- Lighter or less frequent menstrual periods in women.
Symptoms don't look the same in everyone. In older adults, hyperthyroidism can be subtle and easy to miss — instead of looking anxious and revved up, an older person may seem tired, low, withdrawn, or simply have a new irregular heartbeat. Doctors call this quieter presentation apathetic hyperthyroidism. If you or an older family member has unexplained weight loss, fatigue, or a new irregular pulse, a thyroid test is reasonable to ask about.
One symptom deserves a separate note. In Graves' disease (described below), some people develop Graves' eye disease — also called Graves' orbitopathy or thyroid eye disease. The eyes can become red, gritty, watery, or appear to bulge forward (a "staring" look), and in more serious cases vision can be affected. This is a related but separate condition driven by the same autoimmune process, and it can flare on its own timeline — sometimes even after the thyroid itself is treated. It needs its own specialist care (see below).
Causes
Hyperthyroidism is not one disease but a final common result of several different problems. The main causes are:
- Graves' disease — by far the most common cause, especially in younger and middle-aged adults. It is an autoimmune condition: the immune system makes antibodies that mistakenly switch the thyroid "on" and keep it overproducing hormone. Graves' is also the cause most often linked to the eye disease described above.
- Toxic multinodular goiter and toxic adenoma — one or more lumps (nodules) in the thyroid become overactive and pump out hormone on their own, independent of the body's normal control. These nodular causes become more common with age.
- Thyroiditis (inflammation of the thyroid) — when the gland becomes inflamed, it can leak its stored hormone into the bloodstream, causing a temporary period of hyperthyroidism. This includes subacute thyroiditis (often after a viral illness, sometimes with a tender, painful thyroid) and postpartum thyroiditis (in the months after giving birth). Crucially, the gland here is not overproducing — it is releasing what it already had — so this form is usually self-limited and is treated differently (see Treatment).
- Excess iodine and certain medications — the thyroid uses iodine to make hormone, so a large iodine load can sometimes tip it into overactivity. The heart-rhythm drug amiodarone, which is rich in iodine, is a well-known cause of thyroid trouble.
- Too much thyroid medication — less commonly, taking more levothyroxine than the body needs (for treated hypothyroidism) can push hormone levels too high. This is corrected by adjusting the dose.
Sorting out which cause you have matters a great deal, because the treatment is different depending on the answer — which is exactly what the diagnostic tests are designed to figure out.
Diagnosis
Hyperthyroidism is diagnosed with simple blood tests, sometimes followed by an antibody test and a scan.
- TSH is the key screening test. Because the pituitary turns TSH down when thyroid hormone is high, a low (suppressed) TSH is the most sensitive early sign of an overactive thyroid.
- Free T4 and T3 measure the actual thyroid hormone in your blood. In overt hyperthyroidism these are high; measuring them alongside TSH tells the doctor how active and how severe the problem is.
- TSH-receptor antibodies — usually reported as TRAb or TSI (thyroid-stimulating immunoglobulin) — help confirm Graves' disease. These are the antibodies that switch the thyroid on, so a positive result points to Graves' as the cause.
- A radioactive iodine uptake scan looks at how eagerly the thyroid takes up iodine, which separates the two big groups of causes. An overactive gland (Graves' disease or hot nodules) shows high uptake, because it is busy making hormone. A leaking, inflamed gland (thyroiditis) shows low uptake, because it isn't manufacturing new hormone — it's just releasing stored hormone. This single distinction often changes the entire treatment plan, which is why the scan can be so useful.
Not everyone needs every test. Often TSH plus free T4/T3 and an antibody test are enough, especially when the picture clearly points to Graves'. The scan is added when the cause is unclear or when telling overproduction apart from leakage will change what treatment makes sense.
Treatment
The right treatment depends on the cause, your age, whether you are pregnant, how severe the symptoms are, and your own preferences. For the overactive causes (Graves' disease and hot nodules), there are three main definitive options, and major guidelines present them as legitimate choices to weigh together with your doctor rather than ranking one as universally "best."
- Antithyroid drugs. These medications slow the thyroid's hormone production. Methimazole is the usual first-line choice for most adults. Propylthiouracil (PTU) is generally reserved for specific situations — notably the first trimester of pregnancy and the management of thyroid storm (see below) — because of differences in their safety profiles at those times. Antithyroid drugs can sometimes bring Graves' disease into lasting remission after a course of treatment (often around 12 to 18 months), though relapse is possible.
- Radioactive iodine therapy. A measured dose of radioactive iodine is taken by mouth; it concentrates in the overactive thyroid tissue and gradually shrinks and quiets it. It is a long-established, effective treatment for Graves' disease and toxic nodules.
- Surgery (thyroidectomy). Removing all or part of the thyroid is a definitive option, often chosen for a very large goiter, when there are suspicious nodules, when other treatments aren't suitable or haven't worked, or in certain cases of significant eye disease.
Beta-blockers (such as propranolol) deserve special mention. They don't treat the thyroid itself, but they rapidly calm the most distressing symptoms — the racing heart, palpitations, tremor, and anxiety — while a definitive treatment is being arranged or begins to take effect. Many people feel noticeably better within days of starting one.
An important exception: hyperthyroidism caused by thyroiditis (the "leaking" type) is usually self-limited — it tends to settle on its own as the inflammation passes. Because the gland isn't overproducing hormone, antithyroid drugs don't help here; instead, it is typically managed with beta-blockers for symptom relief and time, with monitoring.
Finally, a practical reality to expect: after radioactive iodine or surgery, many people end up with an underactive thyroid (hypothyroidism), because the treatment has reduced or removed hormone-producing tissue. That is a manageable, expected outcome — it simply means taking a daily levothyroxine (thyroid hormone replacement) tablet, often for life, with periodic blood tests to keep the dose right. Trading a harder-to-control overactive thyroid for a steady, easily-replaced one is a reasonable and common result, not a treatment failure.
Thyroid Storm — The Emergency
Thyroid storm (also called thyrotoxic crisis) is a rare but life-threatening extreme of hyperthyroidism. It is what can happen when thyroid hormone effects become dangerously exaggerated and overwhelm the body. Warning signs include a high fever, a very fast heart rate or a fast irregular rhythm (atrial fibrillation), agitation, confusion, or delirium, and sometimes vomiting, diarrhea, or signs of the heart struggling.
It is often triggered by an added stress on top of untreated or undertreated hyperthyroidism — for example a serious infection or other illness, surgery, trauma, or suddenly stopping antithyroid medication. Thyroid storm is a medical emergency that requires immediate hospital care. If someone with known or suspected hyperthyroidism becomes feverish, severely agitated or confused, or develops a racing heart, call emergency services — do not wait it out at home.
When to See a Doctor & Living With It
See a doctor if you have palpitations or a persistently fast or irregular heartbeat, unexplained weight loss, a new tremor, ongoing anxiety with a racing feeling, or changes in your eyes such as bulging, persistent redness, double vision, or eye pain. These deserve evaluation, and a thyroid blood test is a simple first step.
Graves' eye disease needs specialist care — typically an endocrinologist working with an ophthalmologist (eye specialist). One thing is firmly established and squarely within your control: smoking dramatically worsens thyroid eye disease and makes treatment less effective, so quitting smoking is one of the most important things a person with Graves' can do for their eyes.
Pregnancy is a special situation that needs careful, expert management, because both untreated hyperthyroidism and the medications used carry considerations for mother and baby; treatment is tailored and closely monitored, and (as noted above) the choice of antithyroid drug differs by trimester. If you have hyperthyroidism and are pregnant or planning a pregnancy, tell your care team early.
Living with hyperthyroidism is, for most people, a story of getting better. The key theme afterward is long-term monitoring: regular blood tests to confirm the thyroid is back in balance, to catch a relapse of overactivity, and — very commonly after radioactive iodine or surgery — to detect and treat an underactive thyroid with the right dose of levothyroxine. With treatment and follow-up, the great majority of people return to feeling like themselves again.
Research Papers
- Ross DS, Burch HB, Cooper DS, et al. (2016). 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid 26(10):1343–1421. — The major US clinical guideline; lays out how each cause is diagnosed and the case for antithyroid drugs, radioactive iodine, or surgery.
- De Leo S, Lee SY, Braverman LE (2016). Hyperthyroidism. Lancet 388(10047):906–918. — A clear, comprehensive medical review of the causes, evaluation, and treatment of an overactive thyroid.
- Smith TJ, Hegedüs L (2016). Graves' Disease. New England Journal of Medicine 375(16):1552–1565. — An authoritative review of the most common cause of hyperthyroidism, including the autoimmune mechanism and eye disease.
- Kahaly GJ, Bartalena L, Hegedüs L, et al. (2018). 2018 European Thyroid Association Guideline for the Management of Graves' Hyperthyroidism. European Thyroid Journal 7(4):167–186. — The European counterpart guideline, with detailed guidance on choosing among the antithyroid-drug, radioiodine, and surgical options.
- Alexander EK, Pearce EN, Brent GA, et al. (2017). 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid 27(3):315–389. — The reference guideline for managing thyroid disease in pregnancy, including the trimester-specific choice between PTU and methimazole.
- Bartalena L, Kahaly GJ, Baldeschi L, et al. (2021). The 2021 European Group on Graves' Orbitopathy (EUGOGO) Clinical Practice Guidelines for the Medical Management of Graves' Orbitopathy. European Journal of Endocrinology 185(4):G43–G67. — The specialist guideline for Graves' eye disease, including the strong evidence that smoking worsens it.
Connections
- Endocrinology
- How Your Thyroid Is Controlled — interactive animation
- Hypothyroidism
- Graves' Disease
- Thyroid Disorders
- Hashimoto's Thyroiditis
- Thyroid Panel
- Essential Tremor