Post-Traumatic Stress Disorder (PTSD)
Interactive Visualization Memory & LTP — strengthen a synapse into a memory Watch two neurons that fire together wire together — the NMDA receptor detects the coincidence, calcium floods in, and the synapse strengthens — then block it with alcohol and watch the memory fail to form. Launch →
Table of Contents
- What is PTSD?
- DSM-5 Diagnostic Criteria
- Four Symptom Clusters
- Prevalence and Epidemiology
- Neurobiological Underpinnings
- Complex PTSD (ICD-11)
- Pharmacotherapy
- Trauma-Focused Psychotherapy
- MDMA-Assisted Therapy
- Comorbidities and Special Populations
- Research Papers
- Connections
- Featured Videos
What is PTSD?
Post-Traumatic Stress Disorder (PTSD) is a psychiatric disorder that can occur in people who have experienced or witnessed a traumatic event such as a natural disaster, serious accident, terrorist act, war or combat, rape, or other violent personal assault. PTSD was first formally recognized in the DSM-III in 1980, though the clinical syndrome — then called "shell shock" or "combat fatigue" — had been described in veterans since World War I. It affects people of all ages and backgrounds, not just military veterans.
PTSD is distinguished from normal stress reactions by its duration (symptoms persist beyond one month), severity (significant functional impairment), and specific symptom constellation involving re-experiencing, avoidance, negative alterations in cognition and mood, and hyperarousal. Unlike Adjustment Disorder, PTSD requires a formally "traumatic" Criterion A stressor — not merely a difficult life event.
DSM-5 Diagnostic Criteria
The DSM-5 (2013) defines PTSD under "Trauma- and Stressor-Related Disorders." The diagnosis requires all of the following:
Criterion A: Traumatic Stressor
Exposure to actual or threatened death, serious injury, or sexual violence via one or more of these routes:
- Direct exposure: experiencing the traumatic event oneself
- Witnessing: observing the event as it happened to others in person
- Indirect — close person: learning that a traumatic event occurred to a close family member or close friend (violent or accidental death must be actual or threatened)
- Repeated/extreme indirect exposure: first-hand, repeated exposure to aversive details of traumatic events — applies to emergency workers, forensic investigators, etc. Note: exposure through media (news, photographs, video) does NOT qualify unless it is occupational
This Criterion A requirement is the formal boundary that distinguishes PTSD from Adjustment Disorder. A painful divorce, job loss, or financial crisis — while genuinely distressing — does not meet Criterion A unless it involved actual or threatened death, serious injury, or sexual violence.
Additional Criteria
- Criterion B (Intrusion): at least 1 intrusion symptom present
- Criterion C (Avoidance): at least 1 avoidance symptom
- Criterion D (Negative alterations in cognition/mood): at least 2 symptoms
- Criterion E (Arousal/reactivity alterations): at least 2 symptoms
- Duration: disturbance lasts more than 1 month (distinguishes from Acute Stress Disorder)
- Functional impairment: significant distress or impairment in social, occupational, or other important areas
- Not attributable to substances or medical condition
Specifiers include: With dissociative symptoms (depersonalization or derealization) and With delayed expression (full criteria not met until at least 6 months after the event).
Four Symptom Clusters
Criterion B: Intrusion Symptoms (1 or more required)
Intrusion symptoms represent the involuntary, unwanted re-experiencing of the trauma:
- Intrusive memories: recurrent, involuntary, distressing memories of the traumatic event
- Nightmares: recurrent distressing dreams related to the event
- Flashbacks: dissociative reactions where the person feels or acts as if the traumatic event is recurring (can range from brief intrusions to complete loss of awareness of present surroundings)
- Intense psychological distress at cues: marked emotional distress when exposed to internal or external cues that symbolize or resemble an aspect of the traumatic event
- Physiological reactions to cues: marked physiological reactions (racing heart, sweating, trembling) to trauma-related cues — a distinguishing feature from ordinary sad memories
Criterion C: Avoidance (1 or more required)
Persistent effortful avoidance of stimuli associated with the traumatic event:
- Internal avoidance: avoidance of or efforts to avoid distressing memories, thoughts, or feelings about or closely associated with the traumatic event
- External avoidance: avoidance of or efforts to avoid external reminders (people, places, conversations, activities, objects, situations) that arouse distressing memories, thoughts, or feelings
Avoidance is the mechanism that prevents natural recovery. By not processing the memory, the fear network remains active and the memory is never contextualized as "past." This is why avoidance-based coping perpetuates PTSD and why all effective trauma therapies involve confronting rather than avoiding the memory.
Criterion D: Negative Alterations in Cognitions and Mood (2 or more required)
These symptoms represent the persistent emotional and cognitive consequences of trauma — often the hardest for loved ones to recognize as PTSD symptoms rather than character flaws:
- Dissociative amnesia: inability to remember an important aspect of the traumatic event (not due to head injury, alcohol, or drugs)
- Persistent negative beliefs: persistent and exaggerated negative beliefs or expectations about oneself, others, or the world (e.g., "I am bad," "No one can be trusted," "The world is completely dangerous")
- Distorted blame: persistent, distorted cognitions about the cause or consequences of the traumatic event that lead to blaming oneself or others
- Persistent negative emotions: persistent negative emotional states (fear, horror, anger, guilt, shame)
- Diminished interest: markedly diminished interest or participation in significant activities
- Feelings of detachment or estrangement: feeling alienated or detached from others
- Emotional numbing: persistent inability to experience positive emotions (inability to experience happiness, satisfaction, or loving feelings) — this is distinct from depression's anhedonia and reflects a specific constriction of emotional range
Criterion E: Alterations in Arousal and Reactivity (2 or more required)
The hyperarousal cluster reflects the nervous system remaining in a state of threat-readiness long after the danger has passed:
- Irritability and aggressive outbursts: irritable behavior and angry outbursts (with little or no provocation), typically expressed as verbal or physical aggression toward people or objects
- Reckless or self-destructive behavior
- Hypervigilance: a state of heightened alertness and sensitivity to potential threats — scanning the environment, sitting with back to walls, never feeling safe in public spaces
- Exaggerated startle response: jumping at sudden sounds or movements that others would barely notice
- Concentration difficulties: problems with concentration that can impair work and daily functioning
- Sleep disturbance: difficulty falling or staying asleep, or restless sleep — often compounded by trauma nightmares from Criterion B
Prevalence and Epidemiology
PTSD is more common than many people realize, affecting millions worldwide. Rates vary sharply by trauma type and population group:
General Population
- US past-year prevalence: 3.6% of adults (National Comorbidity Survey)
- US lifetime prevalence: 6.8% (NCS-R, Kessler et al, 1995)
- Global lifetime prevalence: approximately 2.4% — lower than US estimates, partly reflecting methodology and cultural variation in trauma exposure and reporting
- Gender gap: women are approximately twice as likely as men to develop PTSD after trauma exposure — reflecting differences in trauma type (sexual assault rates), biological factors (estrogen effects on fear circuitry), and socialization around help-seeking
High-Risk Populations
- Combat veterans: 10-30% depending on conflict era and intensity; Vietnam veterans up to 30%; Gulf War and Iraq/Afghanistan veterans 10-20%
- Sexual assault survivors: 33-50% — the highest rates of any trauma type, reflecting the unique combination of violation, betrayal, shame, and self-blame
- Disaster survivors: 5-10% in general populations; higher following technological disasters (oil spills, nuclear accidents) vs natural disasters
- Refugees and displaced persons: 30-50% in many studies
- Emergency responders and first responders: 10-20%; higher with frequent trauma exposure
- Children and adolescents: 3-15% following disasters; higher following interpersonal trauma
Risk and Resilience Factors
- Pre-trauma risk factors: prior trauma history, childhood adversity, pre-existing anxiety or depression, family history of mental illness, lower socioeconomic status
- Peri-trauma risk factors: high trauma severity, perceived life threat, peritraumatic dissociation, lack of social support during event
- Post-trauma risk factors: lack of social support, ongoing stress, additional traumas, avoidance coping, negative appraisals of the trauma
Importantly, PTSD does not develop in the majority of trauma-exposed individuals. Approximately 70-80% of adults experience at least one Criterion A event in their lifetime, yet only about 6.8% develop PTSD. Resilience is the norm; PTSD represents a failure of normal recovery processes, not a character weakness or inevitability of trauma.
Neurobiological Underpinnings
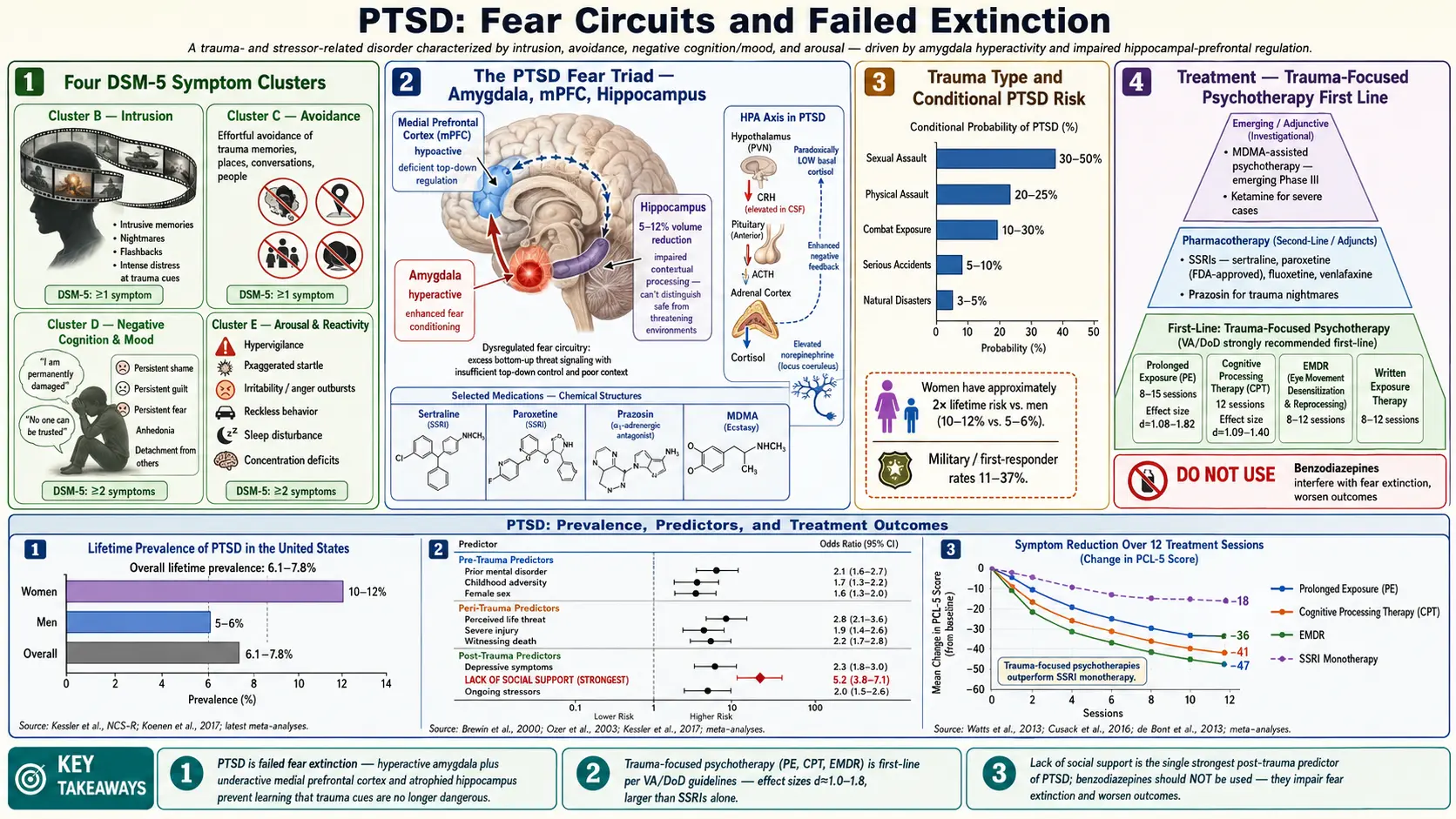
PTSD represents a disorder of fear memory — specifically, a failure of fear extinction and contextual memory. Four brain regions and one endocrine system are central to understanding its biology:
Amygdala Hyperreactivity
The amygdala encodes emotional memories, particularly fear. In PTSD, the amygdala is hyperreactive to trauma-related cues — responding as if the threat is present even when it is not. Neuroimaging studies (Rauch, Shin, and Phelps, 2006) consistently show increased amygdala activation to threat cues in PTSD versus controls. This hyperactivity drives the intrusion and hyperarousal symptom clusters. The amygdala's "smoke detector" function is set permanently to high sensitivity, triggering a full threat response to stimuli that merely resemble elements of the original trauma.
Hippocampal Volume Reduction
The hippocampus is critical for contextual memory — encoding not just "what happened" but "when and where," allowing the brain to recognize that a past threat is not a current one. In PTSD, multiple studies show 5-20% reduction in hippocampal volume. This means trauma memories lack proper temporal context: a car backfiring does not register as "a car backfiring in 2024" but triggers the amygdala as if it were gunfire years earlier. The chicken-and-egg debate (pre-existing smaller hippocampus as risk factor vs. stress-induced reduction) has largely been resolved by prospective twin studies: both mechanisms contribute.
Prefrontal Cortex Hypoactivity
The medial prefrontal cortex (mPFC), particularly the ventromedial PFC, normally inhibits amygdala activity and facilitates fear extinction — the learned suppression of fear responses to stimuli that are no longer dangerous. In PTSD, mPFC activity is reduced, impairing this top-down inhibitory control. This is the neurological rationale for exposure-based therapies: they repeatedly activate the mPFC-amygdala extinction circuit, strengthening it through learning until it can reliably inhibit the fear response.
HPA Axis Dysregulation — Low Cortisol in Chronic PTSD
One of the most counterintuitive findings in PTSD biology: unlike major depression (which features elevated cortisol), chronic PTSD is typically associated with low basal cortisol and enhanced cortisol suppression on the low-dose dexamethasone suppression test — indicating a hypersensitive HPA negative feedback loop. Yehuda's pioneering research showed this clearly. The low cortisol state reflects both enhanced glucocorticoid receptor sensitivity and a failure to mobilize the cortisol stress response appropriately. This has treatment implications: hydrocortisone administration before extinction training has shown promise in early trials.
Noradrenergic Dysregulation
The locus coeruleus-norepinephrine system is chronically over-activated in PTSD, driving hyperarousal, exaggerated startle, and trauma nightmares. This is the mechanism underlying the efficacy of prazosin (an alpha-1 adrenergic antagonist) for trauma nightmares: by blocking noradrenergic signaling during REM sleep, it reduces nightmare frequency and intensity. The noradrenergic system also explains why beta-blockers given acutely after trauma may reduce PTSD risk by blunting the norepinephrine surge that consolidates traumatic memories — though this remains investigational.
Complex PTSD (ICD-11)
The ICD-11 (2019) introduced Complex PTSD (CPTSD) as a separate diagnostic category — recognition of decades of clinical observation that survivors of prolonged, repeated interpersonal trauma (childhood abuse, prolonged domestic violence, torture, captivity) present with a more severe and pervasive syndrome than standard PTSD describes.
CPTSD Diagnostic Requirements
CPTSD requires meeting all PTSD criteria plus disturbances in self-organization (DSO) across three domains:
- Affect dysregulation: problems with emotional regulation — intense, difficult-to-control emotional reactions; difficulty returning to baseline after upset; emotional explosiveness or complete emotional shutdown; persistent feelings of emptiness or deadness
- Negative self-concept: persistent beliefs about oneself as diminished, defeated, or worthless — often expressed as deep shame, guilt, or a pervasive sense of being permanently damaged or fundamentally different from other people
- Relational disturbances: persistent difficulties feeling close to others; sense that relationships are dangerous or will inevitably lead to abandonment or betrayal; difficulty trusting even genuinely safe people; chronic interpersonal isolation
DSM-5-TR Status and the BPD Debate
CPTSD is not in the DSM-5 or DSM-5-TR. This represents a genuine ongoing scientific debate. Critics argue that CPTSD symptoms overlap substantially with Borderline Personality Disorder (BPD) — both involve affect dysregulation, negative self-concept, and relationship difficulties. Proponents (Brewin et al, 2017; the ICD-11 working group) argue the two are empirically distinct: CPTSD lacks BPD's identity disturbance, frantic abandonment avoidance, self-harm behaviors, and rapidly shifting self-image, and has a more coherent trauma etiology with a different temporal course. The practical implication for clinicians: a patient with PTSD plus pervasive shame, chronic emptiness, and relationship avoidance (rather than BPD's relationship intensity and instability) likely has CPTSD by ICD-11 criteria and may need stabilization-phase work before intensive trauma processing — standard Prolonged Exposure may be less effective as a standalone without prior affect regulation and safety work.
Pharmacotherapy
Medications for PTSD are adjunctive — they reduce symptom severity but do not process the trauma. The VA/DoD 2023 Clinical Practice Guidelines recommend trauma-focused psychotherapy as first-line; medications are recommended when therapy is unavailable, declined, or insufficient.
FDA-Approved Medications
- Sertraline (Zoloft) — SSRI; FDA-approved for PTSD in 1999; dose range 50-200 mg/day; number needed to treat (NNT) approximately 4-5; primarily reduces hyperarousal and re-experiencing symptoms; modest effect on emotional numbing and avoidance. Brady et al (2000) was the pivotal FDA approval trial showing sertraline significantly superior to placebo on the Clinician-Administered PTSD Scale (CAPS) total score.
- Paroxetine (Paxil) — SSRI; FDA-approved for PTSD; similar efficacy to sertraline; significant concern about discontinuation syndrome due to its short half-life and potent serotonin reuptake inhibition — tapering over weeks to months is essential. Tucker et al (2001) demonstrated paroxetine's efficacy in a controlled trial.
Both SSRIs primarily address hyperarousal and re-experiencing; their effect on the avoidance and numbing clusters is less robust — which is why combining them with trauma-focused psychotherapy typically produces better outcomes than either alone.
Prazosin for Trauma Nightmares
Prazosin is an alpha-1 adrenergic receptor antagonist used at CNS-active doses specifically to reduce trauma nightmares. Dosing: typically 1-5 mg at bedtime, titrated up to 15 mg if tolerated; always start at 1 mg to avoid orthostatic hypotension. Mechanism: by blocking norepinephrine signaling during REM sleep, prazosin reduces the intensity and frequency of trauma nightmares — without sedation or blunting of daytime emotions. The Raskind et al JAMA 2018 randomized trial in veterans found prazosin superior to placebo on nightmare frequency, sleep quality, and overall PTSD symptom severity. The VA/DoD 2023 guidelines strongly recommend prazosin specifically for sleep disturbance and nightmares in PTSD.
Second-Line and Adjunctive Medications
- Venlafaxine (Effexor, SNRI) — 150-300 mg/day; evidence base approaching that of SSRIs; useful when depression is a prominent comorbidity or when SSRI response is inadequate
- Mirtazapine — noradrenergic and specific serotonergic antidepressant (NaSSA); some RCT evidence for PTSD; useful when insomnia and appetite loss are severe; weight gain is a common adverse effect
- Imipramine (TCA) — older evidence base; useful in severe, treatment-resistant PTSD; limited by anticholinergic side effects and cardiac risk in overdose
- Topiramate — some evidence for intrusion symptoms; also useful if comorbid alcohol use disorder is present
- Benzodiazepines — NOT recommended for PTSD: evidence suggests they may worsen long-term outcomes by impairing fear extinction, promoting avoidance, and contributing to substance dependence; they are not merely inactive in PTSD — they may be counterproductive to recovery
Trauma-Focused Psychotherapy
Multiple meta-analyses confirm that trauma-focused therapies outperform supportive therapy, non-trauma-focused CBT, and waitlist control by a large margin (effect sizes d = 1.0-1.8 vs waitlist, d = 0.5-0.8 vs active non-trauma-focused comparison). The key feature of effective PTSD treatment is direct engagement with the traumatic memory — either through exposure or cognitive restructuring — rather than supportive discussion of symptoms at a distance.
Prolonged Exposure (PE) — Foa et al
Developed by Edna Foa at the University of Pennsylvania, PE is based on emotional processing theory: traumatic memories fail to integrate into normal memory networks because they are avoided. PE has two core components:
- Imaginal exposure: the patient retells the trauma narrative aloud in the present tense, repeatedly within sessions (typically 45-60 minutes of imaginal retelling per session) — activating the fear memory so it can be processed and extinguished through habituation and reappraisal
- In vivo exposure: gradual confrontation with avoided real-world situations that are objectively safe but have been avoided due to trauma associations
Format: 8-15 sessions of approximately 90 minutes. Effect sizes: d = 1.08 to 1.82 versus waitlist — among the largest effect sizes in all of psychotherapy research. PE has the strongest and most extensive evidence base of any PTSD treatment modality.
Cognitive Processing Therapy (CPT) — Resick et al
Developed by Patricia Resick, CPT targets the cognitive disruptions trauma produces — specifically stuck points: maladaptive beliefs that interfere with recovery. Common stuck points include: "It was my fault," "I should have done something," "The world is completely unsafe," "I am permanently damaged," "I cannot trust anyone." CPT teaches patients to identify these beliefs, examine the evidence, and develop more balanced and accurate perspectives through structured worksheets and dialogue.
- Format: 12 sessions; can be delivered individually or in group format — both are effective
- Effect sizes: d = 1.09 to 1.40 versus waitlist
- Particularly well-studied in sexual assault survivors and military veterans
- A written trauma account is included in the standard CPT protocol; CPT without the account (CPT-C) has also shown efficacy
Eye Movement Desensitization and Reprocessing (EMDR) — Shapiro
Developed by Francine Shapiro in 1989, EMDR involves having the patient briefly focus on the traumatic memory while simultaneously engaging in bilateral stimulation — typically side-to-side eye movements following the therapist's finger, but also alternating taps or auditory tones. The trauma memory is processed through repeated short exposures interspersed with bilateral stimulation sets.
- Format: 8-12 sessions
- Effect sizes comparable to PE and CPT
- Mechanism: actively debated — it remains unclear whether the eye movements are the active ingredient or whether exposure to the trauma memory is the therapeutic mechanism; dismantling studies have yielded mixed results. The WHO and VA/DoD 2023 guidelines both recommend EMDR as first-line
- May be advantageous for patients who find extended verbal narration too overwhelming to sustain PE's imaginal exposure format
Trauma-Focused CBT for Children (TF-CBT)
The evidence-based adaptation of trauma therapy for children ages 3-18 involves parallel child and parent sessions, with gradual trauma narration, cognitive coping skills, and psychoeducation. The non-offending caregiver component is a key differentiator from adult treatments — caregiver involvement significantly improves child outcomes and is a core component of the model, not optional.
MDMA-Assisted Therapy (Phase 3)
The most significant development in PTSD treatment in decades is MDMA-assisted therapy (MDMA-AT), investigated by the Multidisciplinary Association for Psychedelic Studies (MAPS) through Phase 2 open-label studies and two Phase 3 randomized controlled trials.
MAPS MAPP1 Phase 3 Trial (Mitchell et al, Nature Medicine 2021)
The pivotal Phase 3 trial enrolled 90 patients with severe, chronic PTSD (mean CAPS-5 score 44.7 — in the severe range; many had failed prior treatments). Participants received 3 MDMA sessions (80 mg with an optional 40 mg booster dose) or placebo, each within a structured 8-hour therapy session, supported by 12 non-drug integrative therapy sessions. Results:
- 67% no longer met PTSD diagnostic criteria in the MDMA-AT group versus 32% in the placebo-plus-therapy group
- 33% achieved functional remission in MDMA-AT versus 5% placebo
- Primary outcome (CAPS-5 change from baseline): MDMA group −24.4 points versus −13.9 placebo — clinically and statistically significant
- Adverse effects were transient (nausea, muscle tightness, elevated heart rate during sessions); no serious adverse events attributable to MDMA
- Particularly notable efficacy in participants who had failed prior PTSD treatments and in those with comorbid depression, alcohol use disorder, and dissociative symptoms
Proposed Mechanism
MDMA's therapeutic mechanism in trauma processing involves several converging effects:
- Reduced amygdala reactivity to threatening stimuli — creating a therapeutic window where the trauma memory can be approached without triggering overwhelming fear activation or avoidance
- Increased oxytocin release — enhancing feelings of trust and social connection, strengthening the therapeutic alliance and reducing the shame that typically prevents full trauma disclosure
- Enhanced fear extinction learning — animal studies show MDMA facilitates extinction of conditioned fear responses through hippocampal and amygdalar mechanisms
- Emotional openness without sedation — unlike benzodiazepines, MDMA allows full cognitive engagement with trauma material while simultaneously reducing avoidance, enabling processing that is blocked in ordinary states
Regulatory Status as of 2025
An FDA advisory committee reviewed MAPS data in June 2024 and voted against recommending approval, citing concerns about trial design (functional unblinding given MDMA's subjective effects) and requests for additional confirmatory data. MDMA-AT remains unapproved by the FDA as of 2025 but is available through expanded access protocols for treatment-resistant cases. Australia approved MDMA-AT for PTSD in 2023, becoming the first country to authorize a psychedelic-assisted therapy for a psychiatric condition. The Phase 3 data represent a transformative signal for the field even as the US regulatory path remains uncertain.
Comorbidities and Special Populations
Common Comorbidities
- Major Depressive Disorder: 50-80% of patients with chronic PTSD meet criteria for MDD; the two disorders share emotional numbing, sleep disturbance, and concentration difficulties but have distinct pathophysiology — low cortisol in PTSD versus high cortisol in melancholic depression
- Substance Use Disorders: 30-50% comorbidity; alcohol and cannabis use particularly common as self-medication for hyperarousal and sleep disturbance; integrated treatment addressing both simultaneously is essential — treating PTSD alone or the substance use disorder alone yields inferior outcomes compared to integrated care
- Chronic Pain: high comorbidity, particularly in veterans; overlapping mechanisms including central sensitization and shared noradrenergic dysregulation
- Traumatic Brain Injury (TBI): significant overlap in veterans; overlapping cognitive symptoms (concentration, memory) complicate differential diagnosis; PTSD and TBI can co-occur and compound each other's impairment
- Suicidality: PTSD is an independent risk factor for suicidal ideation and attempts, above and beyond comorbid depression; the triad of PTSD plus MDD plus substance use disorder carries particularly elevated risk and warrants close monitoring and safety planning
Veterans and Military Personnel
Combat PTSD has unique clinical features: moral injury (having committed acts or witnessed failures that violate one's moral code, beyond simple fear-based threat), military sexual trauma (MST), traumatic brain injury co-occurrence, and powerful institutional and cultural barriers to help-seeking. The VA/DoD 2023 Clinical Practice Guidelines represent the largest investment in PTSD treatment research in any population and are updated regularly as evidence accumulates.
Perinatal PTSD
Childbirth can constitute a Criterion A traumatic event — particularly in cases involving perceived threat to life, emergency procedures, loss of control, or obstetric violence. Perinatal PTSD is estimated at 3-4% of deliveries overall and up to 30% in women with high-risk deliveries or prior trauma histories. It is frequently unrecognized by healthcare providers and can interfere with mother-infant bonding, breastfeeding initiation, and subsequent reproductive decisions.
Moral Injury
Moral injury — the damage done when a person does something, fails to prevent something, or witnesses something that violates their deeply held moral beliefs — is distinct from but often co-occurs with PTSD in veterans, healthcare workers, and first responders. It is characterized by shame, guilt, spiritual crisis, and loss of meaning rather than fear-based symptoms. Standard exposure-based PTSD treatments targeting fear extinction are less effective for moral injury; Adaptive Disclosure Therapy and other meaning-focused approaches have been developed specifically to address it.
Research Papers
Background
PTSD was formally introduced into the DSM-III in 1980, largely driven by advocacy from Vietnam War veterans and their clinicians. The diagnosis unified previously fragmented labels — shell shock, combat fatigue, traumatic neurosis, rape trauma syndrome — under a single diagnostic framework. The past 45 years have produced explosive growth in PTSD neuroscience and treatment research, transforming understanding of trauma from a narrative of "psychological weakness" to a diagnosable disorder with neurobiological underpinnings, validated assessment tools, and a range of effective treatments. The field continues to evolve rapidly, particularly in the areas of psychedelic-assisted therapies, biomarker research, and precision medicine approaches to matching patients to optimal treatments.
Key Research Papers
- Mitchell JM et al. MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nature Medicine. 2021;27:1025-1033.
- Foa EB et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring. Journal of Consulting and Clinical Psychology. 2005;73(5):953-964.
- Resick PA et al. A comparison of cognitive-processing therapy with prolonged exposure and a waiting condition for the treatment of chronic posttraumatic stress disorder in female rape victims. Journal of Consulting and Clinical Psychology. 2002;70(4):867-879.
- Shapiro F. Eye movement desensitization: A new treatment for post-traumatic stress disorder. Journal of Behavior Therapy and Experimental Psychiatry. Search PubMed
- Brady K et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial. JAMA. Search PubMed
- Tucker P et al. Paroxetine in the treatment of chronic posttraumatic stress disorder: results of a placebo-controlled, flexible-dosage trial. Journal of Clinical Psychiatry. Search PubMed
- Raskind MA et al. Trial of prazosin for post-traumatic stress disorder in military veterans. JAMA. 2018;320(8):753-763.
- Yehuda R et al. Post-traumatic stress disorder. Nature Reviews Disease Primers. Search PubMed
- Rauch SL, Shin LM, Phelps EA. Neurocircuitry models of posttraumatic stress disorder and extinction: human neuroimaging research — past, present, and future. Biological Psychiatry. 2006;60(4):376-382.
- Brewin CR et al. Proposal for inclusion of complex PTSD in ICD-11. World Psychiatry. 2017;16(1):112-113.
- Kessler RC et al. Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry. 1995;52(12):1048-1060.
- VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder. Version 4.0 (2023).
PubMed Topic Searches
- PubMed: PTSD prolonged exposure therapy
- PubMed: PTSD cognitive processing therapy
- PubMed: PTSD EMDR efficacy
- PubMed: PTSD sertraline RCT
- PubMed: prazosin PTSD nightmares
- PubMed: PTSD amygdala hippocampus neuroimaging
- PubMed: PTSD HPA axis cortisol
- PubMed: complex PTSD ICD-11
- PubMed: MDMA-assisted therapy PTSD
- PubMed: PTSD prevalence epidemiology
- PubMed: PTSD moral injury veterans
- PubMed: PTSD comorbidity depression substance use
Connections
- How Memories Form: Synaptic Plasticity (LTP) — interactive animation
- Anxiety
- Depression
- Bipolar Disorder
- OCD
- Addiction
- Insomnia
- Burnout
- Grief
- Schizophrenia
- Stress Management
- Sleep Hygiene
- Magnesium
- Vitamin D3
- Omega-3 Fatty Acids
- NAC and Mental Health