Raynaud's Disease
1. Overview
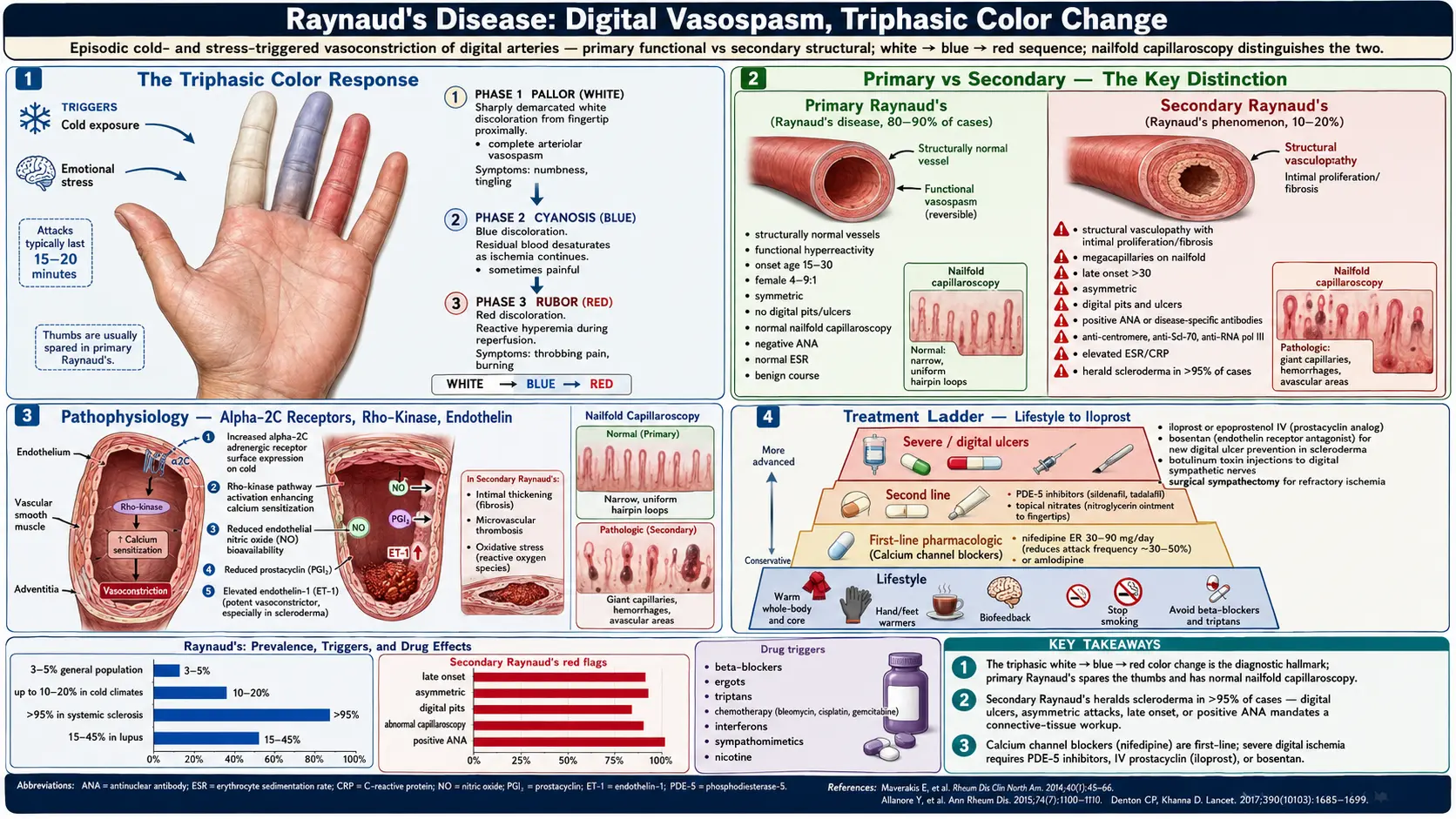
Raynaud's disease (also known as Raynaud's phenomenon or Raynaud's syndrome) is a vascular disorder characterized by episodic, reversible vasospasm of the digital arteries and arterioles in response to cold exposure or emotional stress. During an attack, affected fingers or toes undergo the classic triphasic color change sequence: white (pallor from ischemia), followed by blue (cyanosis from deoxygenation), and finally red (rubor from reactive hyperemia during reperfusion). These episodes, commonly called "Raynaud's attacks," cause numbness, tingling, pain, and in severe cases, digital ulceration and tissue necrosis.
Raynaud's phenomenon is classified into two distinct forms. Primary Raynaud's disease (Raynaud's disease) occurs in the absence of any underlying associated condition and is generally benign, affecting young women most commonly. Secondary Raynaud's phenomenon occurs in association with an underlying disease, most frequently autoimmune connective tissue diseases such as systemic sclerosis (scleroderma), systemic lupus erythematosus, and mixed connective tissue disease. The distinction between primary and secondary forms is clinically critical, as secondary Raynaud's carries a risk of serious complications including digital ischemia, ulceration, gangrene, and may herald the development of a systemic autoimmune disease.
The condition is remarkably common, affecting 3-5% of the general population, making it one of the most prevalent vascular disorders worldwide. While most individuals with primary Raynaud's experience nothing more than uncomfortable but harmless episodes of digital color changes, secondary Raynaud's can be a significant source of morbidity, requiring aggressive medical management and close surveillance for the development of associated connective tissue diseases.
2. Epidemiology
Raynaud's phenomenon is one of the most common vascular conditions encountered in clinical practice. The prevalence varies considerably by geographic region, climate, and study methodology, but is generally estimated at 3-5% of the general population, with rates as high as 10-20% in cold climates (Scandinavia, Northern Europe, Canada). In the United States, approximately 5-10 million people are affected. There is a strong female predominance, with a female-to-male ratio of approximately 4-9:1 for primary Raynaud's, though this ratio narrows for secondary forms.
Primary Raynaud's accounts for approximately 80-90% of all cases and typically presents between ages 15 and 30. Secondary Raynaud's tends to develop later, usually after age 30-40. Among patients initially presenting with Raynaud's phenomenon, approximately 10-15% will eventually develop a connective tissue disease (most commonly systemic sclerosis), with the highest risk occurring within the first 2-5 years of symptom onset. The rate of transition to secondary Raynaud's increases with the presence of antinuclear antibodies, abnormal nailfold capillaroscopy, or disease-specific autoantibodies. Raynaud's phenomenon is extremely common in systemic sclerosis, affecting greater than 95% of patients, and is often the first clinical manifestation, preceding other disease features by months to years.
3. Pathophysiology
Vascular Mechanisms
The core pathological mechanism in Raynaud's phenomenon is exaggerated digital vascular reactivity to cold and sympathetic stimulation. Under normal conditions, cold exposure causes mild, physiological vasoconstriction of digital arteries mediated by alpha-2 adrenergic receptors on vascular smooth muscle cells. In Raynaud's, this vasoconstrictive response is dramatically amplified, resulting in complete cessation of blood flow to affected digits. The underlying vascular abnormalities differ between primary and secondary forms, though both involve an imbalance between vasoconstriction and vasodilation.
Primary Raynaud's: Functional Vasospasm
In primary Raynaud's, the digital vasculature is structurally normal but functionally hyperreactive. Key mechanisms include:
- Increased alpha-2 adrenergic receptor sensitivity — cold exposure causes translocation of alpha-2C adrenergic receptors to the smooth muscle cell surface, amplifying vasoconstrictor responses
- Rho-kinase pathway activation — cold-induced activation of RhoA/Rho-kinase signaling enhances calcium sensitization of vascular smooth muscle, promoting sustained vasoconstriction
- Impaired endothelial vasodilatory function — reduced nitric oxide (NO) bioavailability and decreased production of other vasodilators (prostacyclin, calcitonin gene-related peptide)
- Central and local thermoregulatory dysfunction — exaggerated sympathetic nervous system responses to cold stimuli
Secondary Raynaud's: Structural Vasculopathy
In secondary Raynaud's, particularly when associated with systemic sclerosis, there are structural abnormalities of the digital vasculature that compound the functional vasospasm:
- Endothelial cell injury and activation — leading to release of endothelin-1 (a potent vasoconstrictor), decreased NO production, and increased expression of adhesion molecules
- Intimal proliferation and fibrosis — progressive narrowing of digital artery lumen
- Microvascular thrombosis — platelet activation and fibrin deposition contribute to digital ischemia
- Capillary loss and architectural distortion — visible on nailfold capillaroscopy as enlarged, distorted capillaries (megacapillaries) and avascular areas
- Oxidative stress — ischemia-reperfusion injury during Raynaud's attacks generates reactive oxygen species that further damage the endothelium
The Triphasic Color Response
The characteristic triphasic color change reflects the sequential phases of digital ischemia: white (pallor) results from complete cessation of blood flow due to arteriolar vasospasm; blue (cyanosis) develops as residual blood in the capillaries desaturates; red (rubor) occurs during the recovery phase as vasospasm resolves and reactive hyperemia delivers oxygenated blood to the previously ischemic tissues. Not all patients demonstrate the complete triphasic sequence; biphasic changes (white and blue, or white and red) are common and sufficient for diagnosis.
4. Etiology and Risk Factors
Primary Raynaud's Disease
- Female sex — approximately 80% of primary Raynaud's patients are women; estrogen may influence vascular reactivity
- Young age — typical onset between 15-30 years
- Family history — first-degree relatives of patients with Raynaud's have a 2-3 fold increased risk; concordance in monozygotic twins is approximately 30-60%
- Cold climate — higher prevalence in cooler geographic regions
- Genetic predisposition — variants in genes regulating vascular tone, including NOS3 (endothelial nitric oxide synthase) and adrenergic receptor genes
- Emotional stress and anxiety — sympathetic nervous system activation can trigger attacks
- Low body mass index — thin individuals have less insulation and are more susceptible
Causes of Secondary Raynaud's Phenomenon
Autoimmune Connective Tissue Diseases
- Systemic sclerosis (scleroderma) — Raynaud's in greater than 95%; often the earliest manifestation; most common cause of severe secondary Raynaud's
- Mixed connective tissue disease — Raynaud's in 75-85%
- Systemic lupus erythematosus — Raynaud's in 15-45%
- Sjogren's syndrome — Raynaud's in 15-30%
- Dermatomyositis/polymyositis — Raynaud's in 10-20%
- Rheumatoid arthritis — Raynaud's in 5-10%
Occupational and Environmental Causes
- Vibration white finger (hand-arm vibration syndrome) — prolonged use of vibrating tools (jackhammers, chain saws, pneumatic drills)
- Hypothenar hammer syndrome — repetitive trauma to the ulnar artery from using the palm as a hammer
- Vinyl chloride exposure — industrial chemical causing acro-osteolysis and Raynaud's
- Frostbite injury — previous cold injury can damage digital vasculature
Medications and Substances
- Beta-blockers — particularly non-selective agents (propranolol)
- Ergotamine and triptans — ergot-containing migraine medications
- Chemotherapy agents — bleomycin, cisplatin, vinblastine, gemcitabine
- Interferon-alpha and interferon-beta
- Cyclosporine
- Nicotine and cocaine — vasoconstrictor effects
- Sympathomimetic decongestants — pseudoephedrine, phenylephrine
Vascular and Hematological Causes
- Atherosclerosis — particularly in older men with cardiovascular risk factors
- Thromboangiitis obliterans (Buerger's disease) — in young male smokers
- Thoracic outlet syndrome — compression of subclavian artery or brachial plexus
- Cryoglobulinemia and cold agglutinin disease
- Polycythemia vera — blood hyperviscosity impairs digital perfusion
- Antiphospholipid syndrome
5. Clinical Presentation
Typical Raynaud's Attack
The classic Raynaud's attack follows a predictable pattern triggered by cold exposure or emotional stress. Affected digits develop sharply demarcated pallor (white), typically beginning at the fingertips and progressing proximally. The thumbs are usually spared in primary Raynaud's. During the ischemic phase, patients experience numbness, tingling, and loss of sensation. As the vasospasm persists, the affected digits turn cyanotic (blue) due to deoxygenation. The recovery phase is characterized by erythema (red) as blood flow returns, often accompanied by throbbing pain, burning, and swelling. Attacks typically last 15-20 minutes but can persist for hours in severe cases.
Primary Raynaud's Features
- Symmetric involvement — both hands typically affected equally
- Fingers more than toes — feet involved in approximately 40% of cases
- Thumbs typically spared
- No digital pitting, ulceration, or tissue loss
- Normal nailfold capillaroscopy
- No features of underlying connective tissue disease
- Onset before age 30
- Negative antinuclear antibody (ANA)
- Normal ESR
Secondary Raynaud's Features (Red Flags)
- Late onset (after age 30-40)
- Severe, asymmetric, or painful attacks
- Digital pitting scars, ulceration, or gangrene
- Skin thickening (sclerodactyly)
- Abnormal nailfold capillaroscopy — megacapillaries, capillary loss, hemorrhages
- Positive ANA or disease-specific antibodies (anti-centromere, anti-Scl-70, anti-RNA polymerase III)
- Elevated ESR or CRP
- Associated constitutional symptoms — arthralgias, Sicca symptoms, skin rash, myalgias
- Thumb involvement
Other Affected Sites
- Toes — involved in 40% of primary and more commonly in secondary Raynaud's
- Ears, nose, and nipples — less commonly affected, but can occur
- Tongue — rarely reported, causes dysarthria during attacks
6. Diagnosis
Clinical Diagnosis
The diagnosis of Raynaud's phenomenon is primarily clinical, based on a characteristic history of episodic, well-demarcated digital color changes triggered by cold or stress. Patients should be asked about the triphasic or biphasic color sequence (white, blue, red), the distribution of affected digits, attack frequency and duration, associated symptoms, and the presence of features suggesting an underlying cause. Photographs taken during attacks by patients can be highly valuable for confirming the diagnosis.
Distinguishing Primary from Secondary
The key diagnostic challenge is differentiating primary (benign) from secondary (potentially serious) Raynaud's. The following investigations are recommended for all patients presenting with Raynaud's phenomenon:
- Nailfold capillaroscopy — the single most important test for distinguishing primary from secondary Raynaud's; performed using a dermatoscope, ophthalmoscope, or dedicated capillaroscopy device; normal capillary architecture virtually excludes systemic sclerosis spectrum disease; abnormal findings include megacapillaries (greater than 50 micrometers), capillary hemorrhages, avascular areas, and architectural disorganization
- Antinuclear antibody (ANA) — positive in approximately 20-30% of secondary Raynaud's patients; specific antibodies guide further workup
- Disease-specific autoantibodies — anti-centromere (limited systemic sclerosis), anti-Scl-70/anti-topoisomerase I (diffuse systemic sclerosis), anti-RNA polymerase III (diffuse systemic sclerosis with renal crisis risk), anti-U1 RNP (mixed connective tissue disease)
- Complete blood count — to assess for hematological disorders
- ESR and CRP — markers of systemic inflammation
- Complement levels (C3, C4)
- Cryoglobulins — when cryoglobulinemia is suspected
- Thyroid function tests — hypothyroidism can contribute to cold sensitivity
Vascular Assessment
- Digital artery pressures — measured using photoplethysmography or laser Doppler; reduced pressures indicate fixed arterial obstruction rather than purely vasospastic disease
- Cold provocation testing — cooling the hands in water (10-15 degrees Celsius) while monitoring digital temperature recovery; abnormal recovery time supports the diagnosis but is poorly standardized
- Duplex ultrasound — for evaluating proximal arterial disease (thoracic outlet syndrome, subclavian or ulnar artery occlusion)
- CT angiography or MR angiography — for evaluating proximal arterial stenosis or occlusion when suspected
LeRoy and Medsger Criteria
The widely used LeRoy and Medsger criteria (1992, updated 2001) classify primary Raynaud's as: episodic vasospastic attacks, no tissue necrosis/ulceration/gangrene, normal nailfold capillaries, negative ANA (or titer less than 1:100), and normal ESR. The presence of any abnormality in these criteria suggests secondary Raynaud's and warrants further investigation and monitoring.
7. Treatment
Non-Pharmacological Measures
- Cold avoidance and body warming — the most important intervention; wearing insulated gloves, layered clothing, hand warmers, and heated gloves; keeping the core body warm (trunk and head) is as important as hand protection
- Smoking cessation — nicotine is a potent vasoconstrictor; smoking cessation is essential
- Avoidance of vasoconstricting medications — discontinue beta-blockers, ergotamines, sympathomimetics, and other offending agents when possible
- Stress management — biofeedback, relaxation techniques, and cognitive behavioral therapy may reduce attack frequency
- Regular exercise — improves cardiovascular fitness and peripheral circulation
- Avoidance of vibrating tools — for occupational Raynaud's
- Hand care — protecting skin integrity, moisturizing, avoiding trauma to digits
Pharmacological Therapy: First-Line
- Dihydropyridine calcium channel blockers — first-line pharmacotherapy; nifedipine (30-60 mg/day sustained-release) is the most studied agent; reduces attack frequency by approximately 33% and severity by 50%; side effects include headache, flushing, ankle edema, and hypotension; amlodipine (5-10 mg/day) is an alternative with fewer side effects
Pharmacological Therapy: Second-Line
- Phosphodiesterase-5 (PDE5) inhibitors — sildenafil (20 mg three times daily), tadalafil (20 mg on alternate days), or vardenafil; increase nitric oxide-mediated vasodilation; particularly useful for severe Raynaud's with digital ulceration; a meta-analysis showed significant improvement in attack frequency, duration, and severity
- Topical nitroglycerin — 0.2-2% topical ointment or patches applied to affected digits; local vasodilation; limited by headache and tolerance
- Angiotensin receptor blockers — losartan (50-100 mg/day); modest benefit demonstrated in some trials
- Selective serotonin reuptake inhibitors (SSRIs) — fluoxetine (20 mg/day); may reduce attack frequency and severity through serotonin-mediated vascular effects
- Alpha-1 adrenergic receptor blockers — prazosin (1-5 mg twice daily); limited by orthostatic hypotension and tachyphylaxis
Treatment of Severe and Refractory Disease
- Intravenous iloprost (prostacyclin analogue) — most effective treatment for severe Raynaud's with digital ulceration; infused over 3-5 days; produces sustained improvement lasting weeks to months; standard of care for digital ischemia in systemic sclerosis; not available in all countries
- Endothelin receptor antagonists — bosentan (62.5-125 mg twice daily) reduces new digital ulcer formation in systemic sclerosis (RAPIDS-2 trial); does not heal existing ulcers; requires liver function monitoring
- Botulinum toxin type A injection — injected around digital arteries or into the palm; blocks sympathetic vasoconstriction; case series show improvement in pain, blood flow, and ulcer healing; limited controlled trial data
- Sympathectomy — surgical (cervical or digital sympathectomy) interrupts sympathetic nerve supply to affected digits; cervical sympathectomy has fallen out of favor due to complications and recurrence; digital sympathectomy (periarterial adventitial stripping) may be considered for severe refractory digital ischemia
- Low-dose aspirin or anticoagulation — for cases with thrombotic digital ischemia
Management of Digital Ulcers
- Wound care — moist wound healing, appropriate dressings, debridement of necrotic tissue
- Pain management — opioids may be required for ischemic pain during acute digital ischemia
- Infection management — prompt treatment of secondary infection with appropriate antibiotics
- IV prostanoids (iloprost) — primary treatment for critical digital ischemia
- Surgical amputation — required for irreversible gangrene; limited to the minimum necessary tissue
8. Complications
- Digital ulceration — occurs in approximately 30-50% of secondary Raynaud's (especially systemic sclerosis); painful, slow-healing ulcers on fingertips and over bony prominences
- Digital gangrene — irreversible tissue necrosis requiring amputation in severe cases; rare in primary Raynaud's but can occur in secondary forms
- Digital pitting scars — small, depressed scars on fingertips from healed ischemic episodes
- Calcinosis — calcium deposits in soft tissues, particularly in systemic sclerosis-associated Raynaud's; can ulcerate through the skin
- Secondary infection of digital ulcers — osteomyelitis of the distal phalanx is a serious complication
- Chronic pain and disability — impaired fine motor function, difficulty with daily activities in cold environments
- Progression to connective tissue disease — approximately 10-15% of patients initially presenting with isolated Raynaud's eventually develop a systemic autoimmune disease, most commonly systemic sclerosis
- Psychosocial impact — anxiety about attacks, avoidance of cold environments, and occupational limitations
- Acro-osteolysis — resorption of the distal phalanges in severe, chronic secondary Raynaud's (especially systemic sclerosis)
9. Prognosis
The prognosis of Raynaud's phenomenon depends entirely on whether the condition is primary or secondary. Primary Raynaud's disease has an excellent prognosis. Attacks tend to remain stable or may even improve over time, particularly after menopause. There is no risk of digital tissue loss in primary Raynaud's, and the condition does not affect life expectancy. However, quality of life can be significantly impacted by the inconvenience of frequent attacks and the need for cold avoidance.
Patients with primary Raynaud's should be monitored for transition to secondary disease, which occurs in approximately 3-5% of cases initially classified as primary when stringent diagnostic criteria (normal capillaroscopy, negative ANA) are applied. When transition occurs, it typically manifests within the first 2-5 years and most commonly evolves into systemic sclerosis spectrum disease. Risk factors for transition include positive ANA (especially anti-centromere or anti-Scl-70), abnormal nailfold capillaroscopy at any point, asymmetric attacks, and severe symptoms.
Secondary Raynaud's prognosis is determined by the underlying disease. In systemic sclerosis, digital ulceration occurs in 30-50% of patients over the disease course, and digital amputation is required in approximately 5-10%. Digital ulcers are associated with significant morbidity, including chronic pain, functional disability, and secondary infection. The introduction of endothelin receptor antagonists (bosentan) and IV prostanoids (iloprost) has improved outcomes for digital ischemia, reducing new ulcer formation by approximately 30-50%.
10. Prevention
Prevention strategies for Raynaud's phenomenon focus on reducing attack frequency and severity and preventing the development of complications:
- Cold protection — the most effective preventive measure; wearing insulated, waterproof gloves and mittens; using chemical or battery-powered hand warmers; warming the car before driving; wearing gloves when handling cold items (refrigerator, frozen foods); maintaining warm core body temperature with layered clothing
- Home environment — maintaining warm indoor temperatures, using heated blankets, avoiding air-conditioned environments when possible
- Smoking cessation — absolutely essential; nicotine constricts blood vessels and worsens symptoms; secondhand smoke exposure should also be minimized
- Medication review — avoiding or replacing medications that worsen Raynaud's (beta-blockers, ergotamines, sympathomimetics, certain migraine medications)
- Regular exercise — aerobic exercise improves peripheral circulation and vascular function; avoid exercising in cold environments without adequate protection
- Caffeine moderation — caffeine can cause vasoconstriction in some individuals, though evidence is mixed
- Stress reduction — stress management techniques reduce sympathetically mediated vasospasm
- Occupational modifications — for workers exposed to vibrating tools or cold environments; ergonomic assessment and workplace adaptations
- Digital protection — avoiding trauma to fingers; wearing protective gloves during manual tasks; keeping nails trimmed to avoid nail bed injuries
- Monitoring for secondary disease — patients with isolated Raynaud's should have periodic clinical assessment, nailfold capillaroscopy, and ANA testing to detect early signs of connective tissue disease
Interactive Visualization Cryotherapy: How Cold Changes Your Body Press cold onto the skin and watch the blood vessel clamp shut and the pain nerve slow to a crawl until the ache fades — then push too far and ice crystals form, the same freezing a surgeon uses on purpose to take off a wart or a tumour. Launch →
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Research Papers
- Connections
- Featured Videos
Research Papers
Curated PubMed topic searches on Raynaud's Disease. Each link opens a live PubMed query so the result set stays current as new studies are indexed.
- PubMed topic search: Raynaud phenomenon review
- PubMed topic search: Primary secondary Raynaud
- PubMed topic search: Calcium channel blocker Raynaud
- PubMed topic search: Nifedipine Raynaud trial
- PubMed topic search: Sildenafil Raynaud
- PubMed topic search: Iloprost Raynaud digital ischemia
- PubMed topic search: Bosentan digital ulcer
- PubMed topic search: Systemic sclerosis Raynaud
- PubMed topic search: Nailfold capillaroscopy
- PubMed topic search: Raynaud cold exposure management
- PubMed topic search: Ginkgo Raynaud
- PubMed topic search: Botulinum toxin Raynaud
Connections
- Cryotherapy: How Cold Changes Your Body & the cold response — interactive animation
- Lupus
- Sjogren's Syndrome
- Arthritis
- Magnesium
- Vitamin D3
- Ginkgo Biloba
- Ginger
- Hypertension
- Cold Hands and Feet
- Atherosclerosis
- Calcium
- Ankylosing Spondylitis
- Migraine
- Stress Management
- Edema
- ANA dsDNA and Lupus Autoantibodies
- Lupus and Sjögren's Overlap
- Cutaneous Lupus and Photoprotection
- Rheumatoid Arthritis
- Cryotherapy Safety, Risks and Contraindications