Endometriosis: History and Discovery
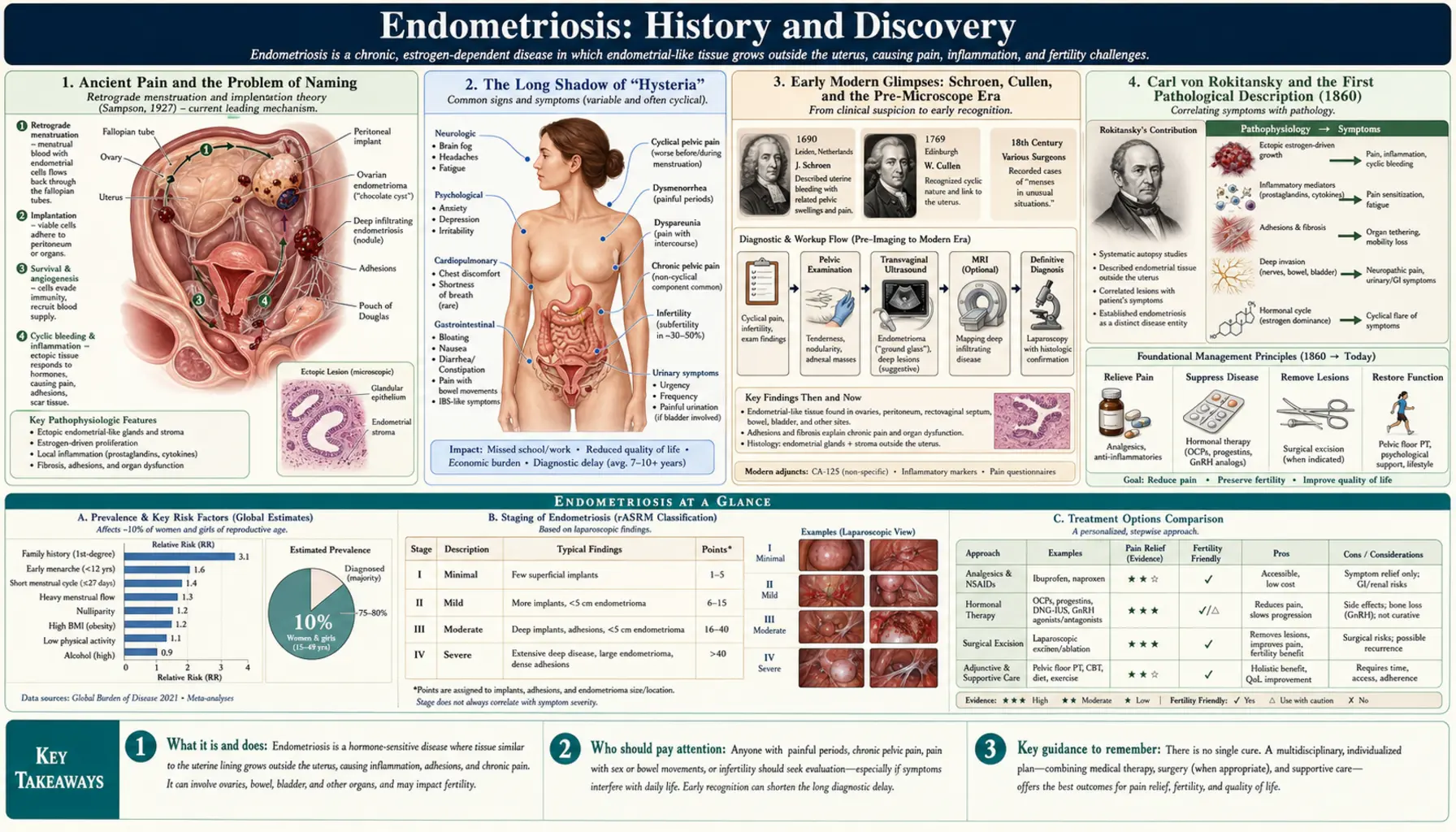
Endometriosis — tissue resembling the uterine lining growing outside the uterus — has almost certainly affected people for as long as there have been menstruating bodies, yet its written history is short, contested, and shadowed by centuries of disbelief. The microscope gave it a face in 1860, when the Vienna pathologist Carl von Rokitansky described the disease under the lens; a name and an enduring theory arrived in the 1920s through the New York gynecologist John A. Sampson. But long before either, the same pain was often dismissed as “hysteria,” and to this day the fundamental question — why does this tissue appear where it does not belong? — has no settled answer. This is a history worth telling honestly, because so much of it is a record of women not being believed.
Table of Contents
- Ancient Pain and the Problem of Naming
- The Long Shadow of “Hysteria”
- Early Modern Glimpses: Schroen, Cullen, and the Pre-Microscope Era
- Carl von Rokitansky and the First Pathological Description (1860)
- John A. Sampson, the Name, and Retrograde Menstruation (1920s)
- Rival Theories of Origin — a Debate That Never Closed
- The Diagnostic Delay: Decades of Waiting
- The Modern Era: Laparoscopy, Advocacy, and Open Questions
- Research Papers and References
- Connections
- Featured Videos
Ancient Pain and the Problem of Naming
Did people in the ancient world have endometriosis? Almost certainly — the disease is not a modern invention, and severe menstrual pain, chronic pelvic pain, and infertility are described in the oldest surviving medical texts. Some historians point to the Hippocratic writings (around the fifth and fourth centuries BCE), and to Greek, Roman, Egyptian, and later medieval sources, as containing descriptions of suffering that could match endometriosis. On that reading, the condition may have afflicted people for two thousand years or more, hiding in plain sight under names that no longer mean anything to us.
But here an honest history has to slow down. There is a genuine scholarly debate about whether these ancient descriptions truly represent endometriosis or simply describe non-specific symptoms — pelvic pain, heavy or prolonged bleeding, difficulty conceiving — that many conditions can cause. One careful line of argument holds that a disease “remains nameless until recognized, described, and named by a medical scientist,” and that reading endometriosis back into texts whose authors had no concept of ectopic endometrial tissue risks projecting modern knowledge onto people who lacked it. The opposing view, advanced notably by the surgeon and historian Camran Nezhat and colleagues, argues that the symptom patterns and even some macroscopic autopsy descriptions are too consistent to dismiss.
The fair conclusion is the uncomfortable one: we cannot be certain. What we can say is that the experience — cyclical, disabling pelvic pain — is ancient, even if the diagnosis is young. That gap between an old suffering and a young name is the central tension of this entire history, and it matters because the people living with that pain were, for most of recorded time, given explanations that were wrong.
The Long Shadow of “Hysteria”
For much of Western history, women reporting pelvic pain were not diagnosed with a gynecologic disease at all. They were diagnosed with hysteria — a now-discredited catch-all disorder whose very name derives from the Greek hystera, meaning uterus, reflecting the ancient belief that a “wandering womb” or a disordered female reproductive system produced emotional and physical chaos. Hysteria was treated for centuries as fundamentally psychological, a sign of a weak or unstable female mind rather than of organic disease.
A provocative modern hypothesis, again associated with Nezhat and colleagues, proposes that a substantial share of what was historically labeled “hysteria” may in fact have been undiagnosed endometriosis. If that is even partly true, the implication is staggering: it would represent one of the largest sustained misdiagnoses in medical history, one that, over the centuries, helped subject women to disbelief, confinement in asylums, and lifetimes of untreated physical suffering. This remains a hypothesis, not an established fact — we cannot diagnose the dead — and it should be read as a compelling argument about the past rather than a proven claim. But it is a hypothesis grounded in a documented reality: the centuries-old habit of treating women’s pelvic pain as a problem of the mind.
That habit did not vanish with the rise of scientific medicine. The cultural reflex linking female pelvic pain to emotional fragility cast a long shadow over the twentieth century and, many advocates argue, persists today in the routine dismissal of severe period pain as “normal” or “in your head.” Understanding the history of hysteria is therefore not an antiquarian exercise; it is part of understanding why endometriosis was — and still is — so often missed.
Early Modern Glimpses: Schroen, Cullen, and the Pre-Microscope Era
Before the microscope made the disease legible, a handful of physicians recorded findings that, in hindsight, point toward endometriosis without quite grasping it. The German physician Daniel Schroen (the name is sometimes spelled Shroen or Schron) is frequently credited with one of the earliest such accounts in 1690, describing ulcer-like lesions on the peritoneum and pelvic organs of reproductive-age women. It is an important early observation — but it is worth being precise: Schroen described lesions, not the defining feature we now use, namely endometrial-type tissue growing outside the uterus. That concept did not yet exist.
Across the eighteenth and nineteenth centuries, scattered anatomical and clinical reports accumulated, but they were not yet recognized as describing a single, coherent disease. Toward the end of the nineteenth century the picture sharpened. The Canadian-American gynecologist and pathologist Thomas Cullen, working at Johns Hopkins, produced detailed clinical and pathological descriptions in the 1890s and early 1900s, characterizing adenomyoma and related lesions and documenting hallmark symptoms such as severe lower-abdominal pain and abnormally prolonged menstruation. Around the same period the gynecologist William Wood Russell reported (in 1898) ovarian lesions containing endometrial-like tissue — an early description of what would later be called an endometrioma.
These figures matter because they show the discovery of endometriosis was not a single eureka moment but a slow convergence of observations. Each physician saw a piece; none yet saw the whole. The instrument that would let someone finally name the pattern was the microscope, and the person who used it most consequentially had already done his decisive work decades earlier, in Vienna.
Carl von Rokitansky and the First Pathological Description (1860)
The figure most often credited with the first definitive scientific description of endometriosis is Carl von Rokitansky (Karl Freiherr von Rokitansky, 1804–1878), the towering Austrian pathologist of the Vienna Medical School. In 1860, examining tissue under the microscope, Rokitansky identified glands and stroma resembling the lining of the uterus in places where they did not belong — both within the muscular wall of the uterus itself (what we now call adenomyosis) and beyond it. He recognized that this endometrial-type tissue invaded the uterine muscle, a genuinely pioneering pathological insight for his era.
Rokitansky’s 1860 account is rightly regarded as a foundational milestone, but historical accuracy requires two clarifications. First, the vocabulary of his time was different: he and his contemporaries described these growths using terms such as cystosarcoma adenoides uterinum, sometimes framing ovarian and uterine lesions as tumors or sarcomas, because the modern concept — and the word endometriosis — did not yet exist. Second, for roughly the following half-century, what we now distinguish as endometriosis (tissue outside the uterus) and adenomyosis (tissue within the uterine muscle) were largely treated as a single entity. The disentangling of the two would not be completed until the first decades of the twentieth century.
None of this diminishes Rokitansky’s achievement. He gave the disease its first rigorous, microscope-based pathological description and established that abnormally located endometrial tissue was a real, observable phenomenon rather than a vague clinical impression. What he did not provide — because no one yet could — was a name for it and a theory of where it came from. Both would arrive together, two generations later, in upstate New York.
John A. Sampson, the Name, and Retrograde Menstruation (1920s)
The name we use today, and the single most influential theory of how the disease arises, both come from John Albertson Sampson (1873–1946), an American gynecologist and surgeon based in Albany, New York. In a series of landmark papers through the 1920s, Sampson introduced and popularized the term “endometriosis” into medical usage and, crucially, distinguished it as a condition of endometrial tissue growing outside the uterus — finally separating it conceptually from the in-wall disease (adenomyosis) with which Rokitansky’s era had merged it. He also described the dark, altered blood within ovarian endometriotic cysts, coining the still-used clinical term “chocolate cysts.”
Sampson’s most famous contribution is his theory of retrograde menstruation (also called the implantation or transplantation theory). In his work of the early-to-mid 1920s — his foundational papers are commonly dated to around 1921 and a key, often-cited account to 1927 — he proposed that during menstruation, some menstrual blood and viable endometrial fragments flow backward through the fallopian tubes into the pelvic cavity, where they implant on the ovaries, peritoneum, and other surfaces and continue to grow and bleed in response to hormonal cycles. He further suggested that fragments might spread through lymphatic or venous channels, an idea sometimes called his metastatic theory.
Retrograde menstruation remains, a century later, the most widely cited explanation for endometriosis, and Sampson’s name is permanently attached to it. But it has always faced a stubborn problem, one Sampson himself could not fully resolve: retrograde menstrual flow is extremely common — observed in the large majority of menstruating people — yet only a minority develop endometriosis. Backward flow alone, in other words, cannot be the whole story. Something else — about the cells, the immune system, the local environment, or genetics — must determine who develops the disease. That unanswered question opened the door to a set of competing theories that has never fully closed.
Rival Theories of Origin — a Debate That Never Closed
It is essential to be clear, especially for anyone living with this disease: the cause of endometriosis is still not settled. More than a century after Sampson, researchers continue to debate how endometriotic tissue arises, and the leading explanations are generally regarded as complementary rather than mutually exclusive — different mechanisms may operate in different people, or even together in the same person. What follows are the principal hypotheses, presented as the open questions they remain.
The retrograde-menstruation / implantation theory (Sampson) holds that refluxed endometrial fragments implant and grow in the pelvis. The coelomic metaplasia theory, proposed by the German pathologist Robert Meyer in the 1920s, argues instead that cells lining the pelvic and abdominal cavity (the coelomic epithelium, which shares an embryonic origin with the reproductive tract) can transform — undergo metaplasia — into endometrial-type tissue. This theory has the advantage of explaining the rare cases of endometriosis found in people without a functioning uterus, far from the reproductive tract, or even, in extraordinarily rare reports, in men. A related idea, the embryonic-rest or Müllerian-remnant theory (with roots in the work of Friedrich von Recklinghausen and others in the late nineteenth century), proposes that leftover embryonic cells of Müllerian or Wolffian origin, misplaced during fetal development, later differentiate into endometriotic lesions.
More recent decades have added the stem-cell theory — that stem or progenitor cells, possibly originating in the bone marrow or the endometrium itself, seed and sustain lesions — alongside growing emphasis on immune dysfunction (a failure to clear refluxed or ectopic cells), hormonal and inflammatory signaling, and genetic and epigenetic susceptibility, since endometriosis clearly runs in families. The honest scientific consensus today is that none of these theories, alone, explains the full diversity of the disease; the underlying pathogenesis remains incompletely understood, and active research continues on every front. For patients, the practical meaning is simple and worth stating plainly: not knowing the exact cause is a limitation of current science, not a sign that the disease is imaginary. The pain and the lesions are real even where the mechanism is unresolved.
The Diagnostic Delay: Decades of Waiting
If one thread runs unbroken from the ancient mislabeling of pelvic pain to the present day, it is delay. Endometriosis has long been notorious for the gap between a person’s first symptoms and an accurate diagnosis. Numerous studies and patient surveys across many countries have repeatedly found average delays measured not in months but in years — commonly cited figures range from roughly four to eleven years, depending on the country and era studied. Behind every such number is a person whose pain was, for years, normalized, dismissed, or attributed to something else.
The reasons for this delay are layered, and several descend directly from the history told on this page. Cultural normalization teaches that severe period pain is simply part of being a woman, so symptoms go unreported and, when reported, are often minimized. The old reflex of treating female pelvic pain as psychological — the long afterlife of “hysteria” — lingers in the under-investigation of pain. There is a genuine medical obstacle too: for most of the modern era, definitive diagnosis required surgery. Because endometriosis is frequently invisible on standard imaging, confirmation has traditionally depended on laparoscopy — looking inside the pelvis directly, ideally with a biopsy — which is invasive, costly, and not undertaken lightly.
Acknowledging this delay is not a historical footnote; it is, arguably, the most important practical lesson of the whole story. A disease that took two thousand years to name, sixty years to separate from its anatomical cousin, and a further century to begin explaining, has also taken far too long to find in the individual patient. Recognizing that pattern — and refusing to dismiss severe, cyclical, life-limiting pelvic pain — is how the diagnostic delay finally begins to shorten. (For the modern diagnostic pathway in depth, see Endometriosis Diagnosis Delay and Imaging.)
The Modern Era: Laparoscopy, Advocacy, and Open Questions
The later twentieth century transformed how endometriosis is seen — literally. The maturation of laparoscopy, minimally invasive keyhole surgery using a fiber-optic camera, gave surgeons a direct window into the pelvis and made it possible to both diagnose lesions and, in the same operation, treat them by excision or ablation. Laparoscopy became the diagnostic and surgical mainstay, and the refinement of excision techniques gave rise to a generation of specialist surgeons. (Treatment specifics are covered in the deep-dive Fertility and Endometriosis and related articles.)
Just as important as the technology was the rise of patient advocacy. Through the late twentieth and into the twenty-first century, patient organizations, researchers, and a growing public conversation pushed endometriosis from a whispered-about “women’s problem” toward recognition as a serious, common, systemic chronic disease — one affecting an estimated one in ten people of reproductive age with a uterus. Awareness campaigns, dedicated research funding drives, and the simple act of patients sharing their long roads to diagnosis have done real work in chipping away at the centuries of dismissal documented above.
And yet the central scientific questions remain genuinely open. There is still no cure, no fully reliable non-surgical diagnostic test in routine universal use, and no consensus on the disease’s ultimate cause. Modern research is pursuing biomarkers and non-invasive diagnostics, better imaging, the genetics and immunology of susceptibility, and treatments that go beyond hormonal suppression and surgery. The history of endometriosis, in the end, is a history still being written — one in which, after two thousand years, the most overdue chapter is simply this: believing the people who live with it.
Research Papers and References
The references below combine peer-reviewed historical and pathogenesis reviews with curated PubMed topic-search links into the primary literature. Where a single authoritative source is identified with confidence a direct link is given; broader themes are provided as PubMed searches so readers can survey the full evidence base. Historical primary descriptions (Schroen 1690, Rokitansky 1860, Cullen 1890s–1900s, Sampson 1920s) are named in the article as historical sources. Each external link opens in a new tab.
- Nezhat C, Nezhat F, Nezhat C. Endometriosis: ancient disease, ancient treatments. Fertility and Sterility. 2012;98(6 Suppl):S1–S62. — doi:10.1016/j.fertnstert.2012.08.001
- Benagiano G, Brosens I. The history of endometriosis: identifying the disease. Human Reproduction. 1991;6(7):963–968. — PubMed: Benagiano & Brosens, history of endometriosis
- Knapp VJ. How old is endometriosis? Late 17th- and 18th-century descriptions of the disease. Fertility and Sterility. 1999;72(1):10–14. — PubMed: Knapp, how old is endometriosis?
- Sampson JA. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. American Journal of Obstetrics and Gynecology. 1927;14(4):422–469. — PubMed: Sampson 1927, retrograde menstruation
- Koninckx PR, et al. Pathogenesis of endometriosis: the genetic/epigenetic theory and beyond Sampson. Fertility and Sterility. 2019;111(2):327–340. — doi:10.1016/j.fertnstert.2018.10.013
- Lagana AS, et al. The pathogenesis of endometriosis: molecular and cell biology insights. International Journal of Molecular Sciences. 2019;20(22):5615. — doi:10.3390/ijms20225615
- The main theories on the pathogenesis of endometriosis (review). International Journal of Molecular Sciences. 2023;24(5):4254. — doi:10.3390/ijms24054254
- Brosens I, Benagiano G. Endometriosis, a modern syndrome of ancient origin? — historical and pathogenesis context. — PubMed: Brosens & Benagiano, origins of endometriosis
- Hysteria, “the wandering womb,” and the historical misdiagnosis of women’s pelvic pain. — PubMed: endometriosis, hysteria, and misdiagnosis
- Coelomic metaplasia theory of endometriosis (Robert Meyer) — historical and modern evaluation. — PubMed: coelomic metaplasia theory
- Müllerian remnant and embryonic-rest theory of endometriosis. — PubMed: Müllerian-remnant theory
- Stem cells in the origin and pathogenesis of endometriosis. — PubMed: stem cells and endometriosis
- Diagnostic delay in endometriosis — magnitude, causes, and consequences. — PubMed: endometriosis diagnostic delay
- History and evolution of laparoscopy in the diagnosis and surgical treatment of endometriosis. — PubMed: laparoscopy and endometriosis history
External Authoritative Resources
- NICHD (NIH) — Endometriosis
- World Health Organization — Endometriosis Fact Sheet
- PubMed — Endometriosis history and pathogenesis
Connections
- Reproductive Medicine
- Endometriosis (Main Page)
- Endometriosis Diagnosis Delay and Imaging
- Endometriosis and Adenomyosis — the Cousin Condition
- Uterine Fibroids
- Ovarian Cysts
- Polycystic Ovary Syndrome (PCOS)
- Perimenopause
- All Conditions