Anorexia Nervosa
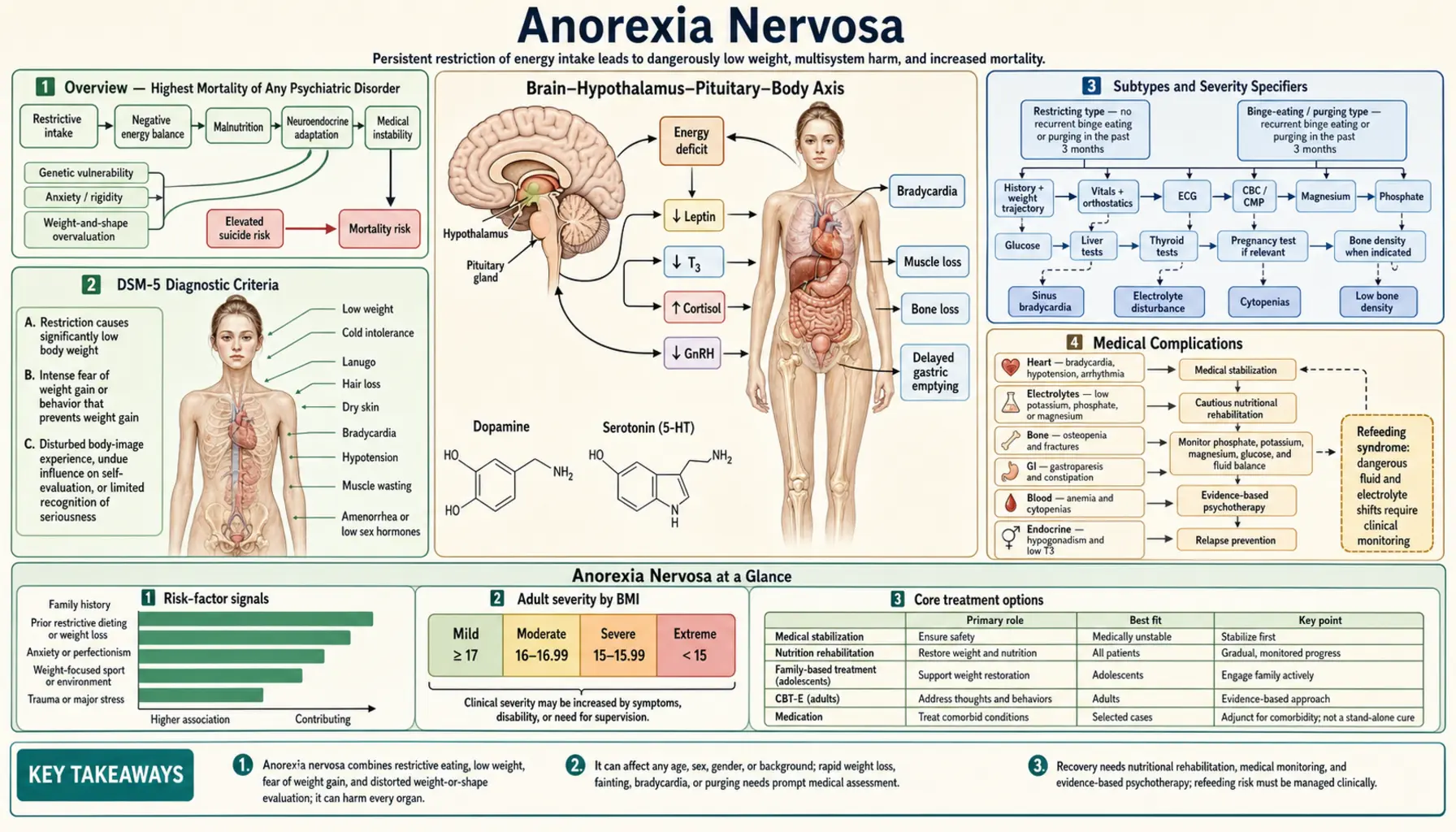
Table of Contents
- Overview — Highest Mortality of Any Psychiatric Disorder
- DSM-5 Diagnostic Criteria
- Subtypes and Severity Specifiers
- Medical Complications
- Refeeding Syndrome
- Differential Diagnosis — ARFID
- Pharmacological Treatment
- Psychotherapeutic Treatment
- Levels of Care and Prognosis
- Research Papers
- Connections
- Featured Videos
Overview — Highest Mortality of Any Psychiatric Disorder
Anorexia nervosa is a serious eating disorder characterized by self-imposed food restriction, intense fear of weight gain, and a distorted perception of body image. It carries the highest mortality rate of any psychiatric disorder, making early recognition and treatment critically important.
Mortality and Epidemiology
- All-cause mortality rate: approximately 5–10% (roughly 5% per decade of illness)
- Standardized mortality ratio (SMR): 5.86 — meaning individuals with anorexia nervosa die at nearly 6 times the expected rate (Arcelus et al., 2011 meta-analysis)
- Suicide mortality: approximately 1% die by suicide; suicide risk is elevated 30–50 times that of the general population
- Causes of death: medical complications (cardiac, electrolyte, organ failure) and suicide are the two leading causes
- Onset: bimodal peak — adolescence (ages 14–18) and young adulthood; a smaller peak occurs in the mid-20s
- Sex distribution: predominantly female, with approximately a 9:1 female-to-male ratio, although male cases are underdiagnosed
- Lifetime prevalence: approximately 0.9% in women and 0.3% in men (DSM-5)
- Onset trigger: often follows a period of dieting, a stressful life event, or puberty; perfectionism, anxiety, and obsessive-compulsive traits are common premorbid features
DSM-5 Diagnostic Criteria
All three criteria (A, B, and C) must be present for a diagnosis of anorexia nervosa:
Criterion A — Restricted Energy Intake
Restriction of energy intake relative to requirements, leading to a significantly low body weight in the context of age, sex, developmental trajectory, and physical health. "Significantly low" is defined as a weight that is less than minimally normal or, for children and adolescents, less than minimally expected.
Criterion B — Intense Fear of Weight Gain
Intense fear of gaining weight or of becoming fat, or persistent behavior that interferes with weight gain, even at a significantly low weight. This fear often does not diminish as weight is lost — it may intensify.
Criterion C — Disturbance in Body Image
Disturbance in the way one's body weight or shape is experienced, undue influence of body weight or shape on self-evaluation, or persistent lack of recognition of the seriousness of the current low body weight. Patients may feel "fat" even when objectively emaciated.
Subtypes and Severity Specifiers
Restricting Type (AN-R)
During the past 3 months, the person has not engaged in recurrent episodes of binge eating or purging. Weight loss is accomplished primarily through dieting, fasting, and/or excessive exercise. This is the classic presentation most people associate with anorexia nervosa.
Binge-Purge Type (AN-BP)
During the past 3 months, the person has engaged in recurrent episodes of binge eating or purging behavior (i.e., self-induced vomiting or the misuse of laxatives, diuretics, or enemas). Crucially, these patients are still at significantly low body weight — this distinguishes AN-BP from bulimia nervosa (BN), where patients are typically at normal or above-normal weight.
DSM-5 Severity Specifiers (Based on BMI)
- Mild: BMI ≥17.0 kg/m²
- Moderate: BMI 16.0–16.99 kg/m²
- Severe: BMI 15.0–15.99 kg/m²
- Extreme: BMI <15.0 kg/m²
Severity can be increased above BMI-based levels to reflect clinical symptoms, degree of functional disability, and need for supervision.
Medical Complications
Anorexia nervosa causes widespread medical complications due to starvation, malnutrition, and purging behaviors. Every organ system can be affected.
Cardiovascular
- Bradycardia: most common cardiovascular finding; the most frequent cause of sudden cardiac death in anorexia nervosa
- Hypotension and orthostatic hypotension: due to volume depletion and autonomic dysfunction
- Prolonged QTc interval: increases risk of ventricular arrhythmia (torsades de pointes)
- Mitral valve prolapse: occurs in a subset due to loss of supporting cardiac tissue
- Pericardial effusion: can develop in severe malnutrition
Dermatological
- Lanugo: fine, downy body hair that grows as a thermoregulatory response to loss of subcutaneous fat
- Dry skin (xerosis) and brittle nails
- Telogen effluvium: diffuse hair thinning and loss caused by nutritional deficiency and physiological stress
- Russell's sign: calluses or scarring on the dorsal surface of the knuckles, caused by repeated trauma from self-induced vomiting (shared with bulimia nervosa)
- Carotenemia: yellowish skin discoloration from elevated carotene (common in restrictive AN)
Endocrine and Metabolic
- Hypothermia: impaired thermoregulation due to loss of fat insulation and reduced metabolic rate
- Amenorrhea: functional hypothalamic amenorrhea caused by suppressed GnRH pulsatility → low LH and FSH → low estrogen; historically required for diagnosis (removed from DSM-5 to allow male/pre-pubertal inclusion)
- Euthyroid sick syndrome (low T3 syndrome): body conserves energy by converting less T4 to active T3; TSH is usually normal — this is adaptive, not primary thyroid disease
- Low IGF-1: growth hormone resistance; impairs bone and muscle maintenance
- Hypoglycemia: depleted glycogen stores; can cause altered mental status
- Low cortisol reserve: relative adrenal insufficiency can occur in extreme cases
Bone
- Osteopenia and osteoporosis: one of the most serious long-term complications, driven by estrogen deficiency, low IGF-1, malnutrition, and cortisol elevation
- Fracture risk: significantly elevated, including stress fractures during exercise
- Peak bone mass: because anorexia often begins in adolescence (the critical window for peak bone accrual), bone loss may be irreversible even after full weight restoration
Renal and Electrolyte
- Dehydration: from restriction and/or purging
- Hypokalemia: particularly with vomiting or laxative use; causes muscle weakness, arrhythmias
- Hyponatremia: from excessive water intake (psychogenic polydipsia) to suppress hunger
- Metabolic alkalosis: from vomiting (loss of HCl)
- Metabolic acidosis: from laxative abuse (bicarbonate loss)
- Renal impairment: chronic dehydration can cause pre-renal azotemia and, in severe cases, chronic kidney disease
Neurological
- Cerebral atrophy: both gray and white matter loss visible on MRI; largely reversible with sustained weight restoration
- Peripheral neuropathy: from B-vitamin deficiencies (especially B1 and B12)
- Cognitive impairment: executive function, attention, and processing speed are all affected; partially related to starvation-induced cerebral changes
- Wernicke's encephalopathy risk: thiamine (B1) deficiency, especially during aggressive refeeding
Refeeding Syndrome
Refeeding syndrome is a potentially fatal metabolic complication that occurs when severely malnourished patients receive rapid nutritional replenishment — whether via oral feeding, enteral tube feeding, or parenteral nutrition. It is a critical safety concern in the inpatient management of anorexia nervosa.
Mechanism
During starvation, the body shifts from carbohydrate to fat metabolism, and total body stores of phosphate, potassium, and magnesium become severely depleted (although serum levels may appear normal). When carbohydrates are reintroduced, insulin surges, driving rapid cellular uptake of these electrolytes:
- Hypophosphatemia is the hallmark finding — phosphate is essential for ATP synthesis
- ATP depletion causes: cardiac arrhythmia (potentially fatal), respiratory muscle failure, hemolytic anemia, seizures, rhabdomyolysis, and altered mental status
- Hypokalemia and hypomagnesemia potentiate cardiac and neuromuscular effects
Prevention Protocol
- "Start low, go slow": NICE guidelines recommend beginning at 5–10 kcal/kg/day in patients with BMI <14 or after prolonged starvation; increase gradually over 4–7 days; maximum weight gain rate of 0.5–1.0 kg/week (inpatient) or 0.5 kg/week (outpatient)
- Electrolyte supplementation before and during refeeding: correct phosphate, potassium, and magnesium prophylactically; monitor electrolytes daily for the first 2 weeks
- Thiamine (Vitamin B1) BEFORE refeeding: administer 200–300 mg/day IV or IM thiamine for at least 30 minutes before any glucose/carbohydrate is given to prevent Wernicke's encephalopathy
- Monitor closely: daily weight, fluid balance, electrolytes, glucose, phosphate, magnesium, potassium; ECG monitoring in high-risk patients
- NICE 2017 and MARSIPAN (UK Royal Colleges) guidelines both identify hypophosphatemia as the primary refeeding danger and mandate pre-emptive supplementation
Differential Diagnosis — ARFID
Several conditions can present with significant food restriction and low weight. The most important differential is Avoidant/Restrictive Food Intake Disorder (ARFID):
ARFID vs. Anorexia Nervosa
- ARFID: restriction based on sensory properties of food (texture, color, smell), fear of aversive consequences (choking, vomiting), or apparent lack of interest in eating — there is no body image disturbance and no fear of weight gain
- AN: restriction is driven by fear of weight gain and distorted body image — the "why" is fundamentally different
- ARFID is common in autism spectrum disorder and ADHD; AN peaks in adolescent girls without autism
- ARFID is not better explained by cultural or religious food practices
Other Differentials
- Bulimia nervosa (BN): binge-purge pattern at normal or above-normal weight (vs. AN-BP which is at significantly low weight)
- Major depressive disorder: appetite loss without body image disturbance or fear of weight gain
- Celiac disease / IBD: weight loss and food avoidance from GI symptoms — rule out with labs
- OCD: food rituals can overlap; the cognitive content distinguishes (contamination/symmetry vs. weight/shape)
- Somatic symptom disorder: food avoidance from vague physical complaints
Pharmacological Treatment
Pharmacotherapy for anorexia nervosa has limited evidence compared to bulimia nervosa, and no medication is FDA-approved specifically for anorexia nervosa.
Olanzapine
The antipsychotic olanzapine has the most supporting evidence for AN, specifically for modest weight gain and reduction in obsessional thinking about food and weight:
- OLANZAN trial (Attia et al., 2019, NEJM): multicenter RCT (N=152) found olanzapine produced significantly greater weight gain than placebo (BMI increase of 0.259 vs. 0.095 per month) but did not significantly improve psychological features of AN
- Typical dose: 2.5–10 mg/day; start low given sedation and metabolic sensitivity in underweight patients
- Monitoring: QTc interval, fasting glucose, lipids, extrapyramidal symptoms
- Considered in treatment-resistant AN, particularly when weight gain is the primary goal and obsessional features are prominent; not recommended as first-line
SSRIs
- SSRIs (particularly fluoxetine) are NOT effective for weight restoration in underweight AN patients — serotonin synthesis is impaired by starvation, so serotonergic agents have minimal effect
- SSRIs may reduce relapse risk and help manage comorbid OCD, anxiety, or depression after weight restoration to a healthy range
Medications to Avoid
- Bupropion: lowers seizure threshold; the risk is amplified by malnutrition and purging-induced electrolyte disturbances — contraindicated in AN
- High-dose antipsychotics: avoid medications with significant QTc-prolonging potential in the context of existing cardiac vulnerability
Psychotherapeutic Treatment
Psychotherapy is the foundation of treatment for anorexia nervosa. The choice of modality depends primarily on patient age and level of care.
Family-Based Treatment (FBT) — Maudsley Approach
FBT is the gold standard for adolescents with anorexia nervosa. It consists of three phases:
- Phase 1 — Externalization and parental control: parents take full control of all food decisions and refeeding; the eating disorder is "externalized" — treated as a separate entity that has hijacked the adolescent, not the adolescent's fault
- Phase 2 — Gradual return of autonomy: as weight is restored, food control is gradually returned to the adolescent
- Phase 3 — Healthy adolescent identity: establishing identity and developmental trajectory independent of the eating disorder
Lock et al. (2010, Arch Gen Psychiatry) RCT demonstrated FBT superiority over individual therapy in adolescents at 1-year follow-up.
CBT-E (Enhanced Cognitive-Behavioural Therapy, Fairburn)
For adults, CBT-E is an extended, individualized form of CBT adapted specifically for eating disorders. It addresses not just eating, weight, and shape concerns, but also "transdiagnostic" maintaining factors including perfectionism, low self-esteem, and interpersonal difficulties. Standard duration is 40 sessions over approximately 40 weeks. Fairburn's CBT-E manual (2008) is the canonical reference.
MANTRA (Maudsley Anorexia Nervosa Treatment for Adults)
MANTRA is a cognitive-interpersonal model developed by Schmidt et al. at King's College London. It explicitly addresses maintaining factors specific to AN: obsessive-compulsive traits, rigid thinking, avoidant emotional processing, and close-others' responses to the illness. Schmidt et al. (2015, Lancet Psychiatry) RCT showed MANTRA was non-inferior to SSCM and both were superior to specialist supportive therapy.
Specialist Supportive Clinical Management (SSCM)
SSCM combines clinical management focused on weight restoration with elements of supportive therapy. It is direct, focuses on the link between eating and symptoms, and is less cognitively demanding than CBT-E or MANTRA. Used particularly in outpatient settings for adults with moderate illness.
Comparative Efficacy
- Adolescents: FBT > individual therapy (CBT or supportive) at 1 year
- Adults: MANTRA ≈ SSCM > specialist supportive therapy; CBT-E shows comparable outcomes; no single modality clearly dominant; weight restoration goal is universal
- Long-term recovery: psychotherapy benefits persist; pharmacotherapy effects are modest and adjunctive
Levels of Care and Prognosis
Stepped Care Model
Treatment intensity is matched to clinical severity and response to lower levels of care:
- Outpatient (OP): weekly or twice-weekly appointments; appropriate for medically stable patients with adequate motivation and social support
- Intensive Outpatient Program (IOP): 3–4 days/week, several hours per day; structured meal support and therapy
- Partial Hospitalization Program (PHP): 5–7 days/week, 6–8 hours/day; daily meal support, medical monitoring, and intensive therapy without overnight stays
- Residential: 24-hour care in a specialized eating disorder facility; for patients who cannot progress in lower levels
- Inpatient medical stabilization: acute hospital admission for medical emergencies
Medical Indications for Inpatient Admission
- Heart rate <50 beats/minute
- Blood pressure <90/60 mmHg
- Potassium (K+) <3.0 mEq/L
- Rapid or uncontrolled weight loss
- Syncopal (fainting) episodes
- QTc >500 ms on ECG
- Blood glucose <60 mg/dL
- BMI <13–14 with physiological compromise
Prognosis
- Full recovery: approximately 50% achieve full recovery at 10-year follow-up (Eddy et al., 2017)
- Partial recovery: approximately 30% have persistent symptoms but improved function
- Chronic course: approximately 20% develop a chronic, treatment-resistant illness
- Mortality: 5–10% over the long term; cardiac complications and suicide are the leading causes
- Predictors of worse outcome: longer duration of illness before treatment, older age at onset, binge-purge subtype, comorbid depression, and previous hospitalizations
- Predictors of better outcome: earlier age of onset, shorter illness duration at presentation, good family support, absence of comorbid substance use
Research Papers
Key Research Papers
- Arcelus J, Mitchell AJ, Wales J, Nielsen S. Mortality rates in patients with anorexia nervosa and other eating disorders: a meta-analysis of 36 studies. Arch Gen Psychiatry. 2011;68(7):724–731. PMID 21727255.
- Treasure J, Claudino AM, Zucker N. Anorexia nervosa. Lancet. Search PubMed
- Attia E, Kaplan AS, Walsh BT, et al. Olanzapine versus placebo for out-patients with anorexia nervosa: a randomised controlled trial (OLANZAN). N Engl J Med. Search PubMed
- Lock J, Le Grange D, Agras WS, Moye A, Bryson SW, Jo B. Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa. Arch Gen Psychiatry. Search PubMed
- Schmidt U, Magill N, Renwick B, et al. The Maudsley outpatient study of treatments for anorexia nervosa and related conditions (MOSAIC): comparison of the Maudsley model of anorexia nervosa treatment for adults (MANTRA) with specialist supportive clinical management (SSCM) in outpatients with broadly defined anorexia nervosa. Lancet Psychiatry. Search PubMed
- Mehler PS, Brown C. Anorexia nervosa — medical complications. J Eat Disord. Search PubMed
- National Institute for Health and Care Excellence (NICE). Eating disorders: recognition and treatment. NICE guideline NG69. Published May 2017.
- Eddy KT, Tabri N, Thomas JJ, et al. Recovery from anorexia nervosa and bulimia nervosa at 22-year follow-up. J Clin Psychiatry. Search PubMed
- Keski-Rahkonen A, Mustelin L. Epidemiology of eating disorders in Europe: prevalence, incidence, comorbidity, course, consequences, and risk factors. Curr Opin Psychiatry. 2016;29(6):340–345. PMID 27662598.
- Fairburn CG. Cognitive Behavior Therapy and Eating Disorders. New York: Guilford Press; 2008. PubMed search: Fairburn CBT eating disorders.
- Mehanna HM, Moledina J, Travis J. Refeeding syndrome: what it is, and how to prevent and treat it. BMJ. Search PubMed
- Strober M, Freeman R, Morrell W. The long-term course of severe anorexia nervosa in adolescents: survival analysis of recovery, relapse, and outcome predictors over 10–15 years in a prospective study. Int J Eat Disord. Search PubMed
PubMed Topic Searches
- PubMed: anorexia nervosa mortality
- PubMed: anorexia nervosa family-based treatment
- PubMed: anorexia nervosa olanzapine
- PubMed: refeeding syndrome anorexia nervosa
- PubMed: anorexia nervosa bone density
- PubMed: anorexia nervosa cardiac complications
- PubMed: anorexia nervosa CBT
- PubMed: anorexia nervosa prognosis recovery
- PubMed: anorexia nervosa brain neuroimaging
- PubMed: ARFID avoidant restrictive food intake disorder
- PubMed: anorexia nervosa hypothalamic amenorrhea
- PubMed: anorexia nervosa suicide risk
Connections
- Psychiatry
- Eating Disorders
- Depression
- Anxiety
- OCD
- Postpartum Depression
- Insomnia
- Burnout
- Phosphorus
- Potassium
- Magnesium
- Vitamin D3
- Vitamin B1 (Thiamine)
- Vitamin B12
- Eating Disorders: History and Discovery — how the condition was described in 1689, named in 1873, and reclassified since.