Eating Disorders: History and Discovery
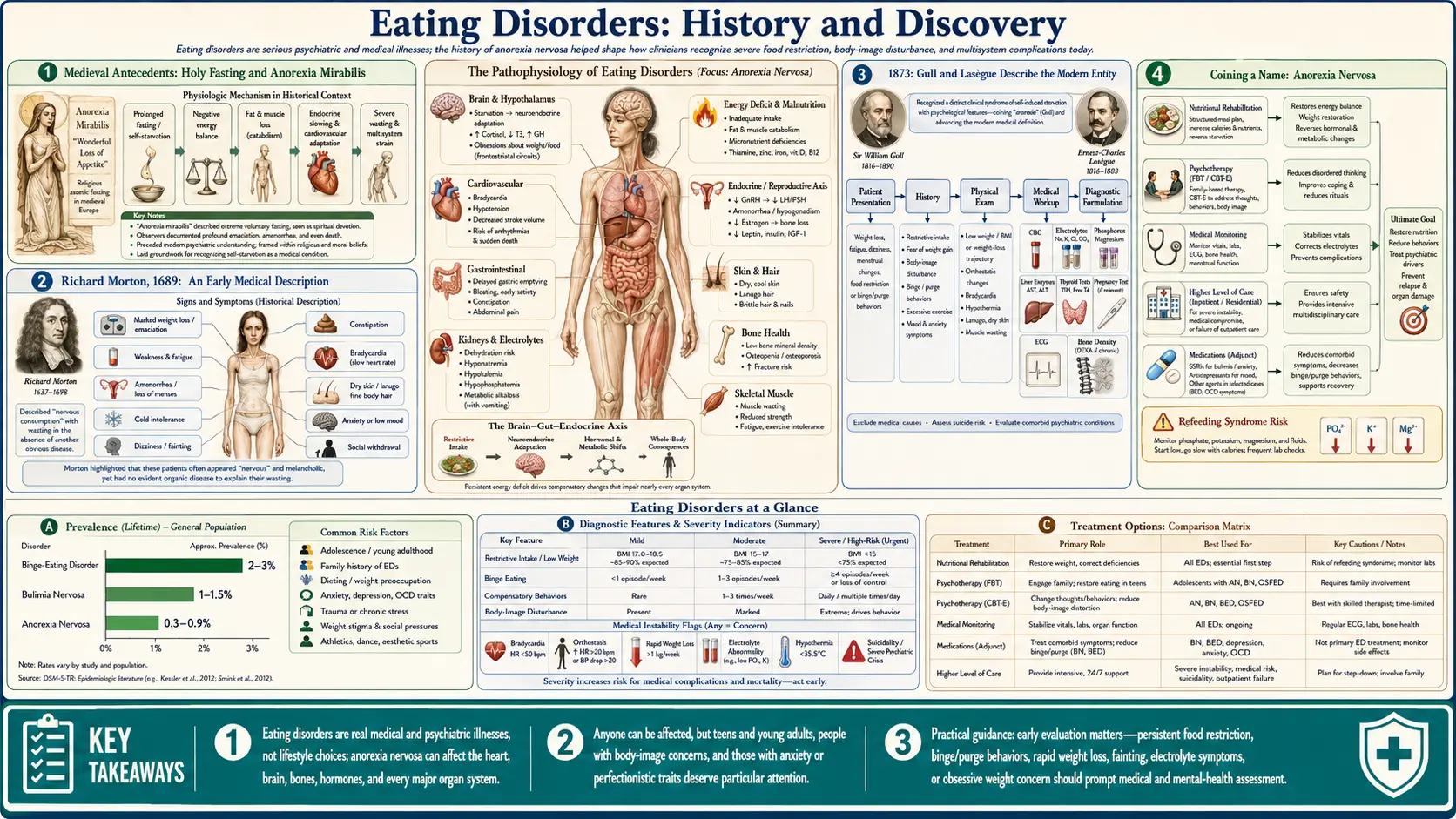
Eating disorders are among the most serious of all psychiatric illnesses, and their history is unusually long. Self-starvation appears in the medieval record as religiously framed fasting; it received an early medical description from Richard Morton in 1689; and in 1873 two physicians—Sir William Gull in England and Charles Lasègue in France—independently described the modern entity, with Gull supplying the enduring name anorexia nervosa. Bulimia nervosa was named only in 1979, and binge eating disorder gained formal standing in 2013. This page traces that medical history with care. It is written for understanding, not instruction: it deliberately avoids any detail about weights, methods, or behaviours that could function as a “how-to,” and it foregrounds the modern understanding of these illnesses as treatable, biologically rooted conditions from which people recover. If you or someone you love is struggling, help exists and is listed at the end.
Table of Contents
- Medieval Antecedents: Holy Fasting and Anorexia Mirabilis
- Richard Morton, 1689: An Early Medical Description
- 1873: Gull and Lasègue Describe the Modern Entity
- Coining a Name: Anorexia Nervosa
- Gerald Russell, 1979: Naming Bulimia Nervosa
- Binge Eating Disorder and the Road to DSM-5
- From Blame to Biology: A Biopsychosocial Illness
- A Serious Illness: Mortality, Recovery, and Hope
- Research Papers and References
- Connections
- Featured Videos
Medieval Antecedents: Holy Fasting and Anorexia Mirabilis
Long before medicine had a name for it, the historical record describes individuals—overwhelmingly women—who refused food to the point of severe wasting. In the late medieval period this took an explicitly religious form that later historians have called anorexia mirabilis (“miraculous lack of appetite”) or, in the phrase of the historian Rudolph Bell, “holy anorexia.” Within the devotional world of the Middle Ages, extreme fasting could be read as a sign of sanctity: a way of imitating the suffering of Christ, of demonstrating purity and humility, and—some scholars argue—of exercising a rare form of agency in a world that gave women little control over their own lives. The best-known case is Saint Catherine of Siena (1347–1380), whose extraordinarily restricted intake is documented in contemporary accounts and is thought to have contributed to her death at thirty-three.
It is important to present this material carefully and as historical context rather than as a clean “first case” of a modern disease. Whether medieval holy fasting can be equated with present-day anorexia nervosa is a genuine and unresolved scholarly debate. The medieval historian Caroline Walker Bynum argued influentially that this fasting belonged to its own religious and cultural framework and should not simply be retrofitted with a twentieth-century psychiatric diagnosis; the motivations, the meaning, and the social setting were profoundly different from those of a patient today. Others see real continuities in the underlying behaviour. Both readings can be held at once: the antecedents are real and worth knowing, but they are antecedents—not proof that the modern illness existed unchanged across the centuries.
What the medieval record does establish is that self-starvation is not a uniquely modern phenomenon and not simply a product of contemporary media or fashion. The cultural framing of food refusal has shifted dramatically—from the sacred to the medical—but the human capacity for it is old. That long backdrop is the proper starting point for the medical history that follows.
Richard Morton, 1689: An Early Medical Description
The first description usually credited as medical rather than religious comes from the English physician Richard Morton (1637–1698). In his 1689 treatise Phthisiologia, seu Exercitationes de Phthisi (“Phthisiologia, or a Treatise of Consumptions”), Morton set out to distinguish the various wasting diseases of his day. Among them he described a condition he called nervous consumption or nervous atrophy (phthisis nervosa): a profound wasting of the body that occurred, strikingly, without the fever, cough, and shortness of breath that marked tuberculosis (the “consumption” of the era). Instead it featured loss of appetite, poor digestion, and a progressive falling away of the flesh.
Morton reported two cases—a young woman and a young man—and his account is notable for what it gets right. He linked the wasting to states of mind, attributing it to “sadness and anxious cares,” and he recorded the patients’ curious lack of concern about their own emaciation—an observation that anticipates the modern clinical picture by more than two centuries. For these reasons later writers have called him the “limner” (portrayer) of anorexia nervosa, and his 1689 description is widely regarded as the earliest in the Western medical literature.
Two cautions keep the history honest. First, Morton described the condition; he did not name it anorexia nervosa—that term lay nearly two hundred years in the future. Second, a seventeenth-century case report cannot be diagnosed with modern confidence, and reading present-day criteria back onto Morton’s patients is necessarily an interpretation. What is secure is that, in 1689, a physician set down a recognizable clinical sketch of self-starvation tied to emotional distress and treated it as a disease.
1873: Gull and Lasègue Describe the Modern Entity
The modern medical entity crystallized in a single remarkable year. In 1873, two physicians—one English, one French, working independently and apparently without knowledge of each other’s ongoing work—published descriptions of the disorder we now recognize. The English physician Sir William Withey Gull (1816–1890), one of the most eminent doctors of Victorian Britain and a physician to Queen Victoria’s household, presented and then published an account that he titled, in 1873, Anorexia Nervosa. In the same year the French physician Ernest-Charles Lasègue (1816–1883) published De l’anorexie hystérique (“On hysterical anorexia”) in the Archives Générales de Médecine.
The two papers are complementary. Gull gave a clear clinical and physiological portrait—the emaciation, the slowed pulse and breathing, the restlessness, the absence of any underlying organic disease—and emphasized careful refeeding and nursing. Lasègue contributed something Gull’s account largely lacked: a psychological and family perspective, describing the course of the illness, the patient’s resistance, and the fraught dynamics that developed around meals within the household. Read together, they frame the condition as Gull’s physiology plus Lasègue’s psychology—a combination close to how clinicians think about it today.
Which man was “first” has been debated ever since, and the honest answer is that it is a near-tie. Gull is often granted slight priority because he had made a brief, rather cryptic reference to such a condition in an 1868 address at Oxford (where he used the phrase apepsia hysterica); when he asserted that priority in 1873, Lasègue replied that he had been entirely unaware of the obscure 1868 remark. The fairest historical statement is the one most modern reviews adopt: Gull and Lasègue described the modern disorder independently and almost simultaneously in 1873, and the field owes the entity to both.
Coining a Name: Anorexia Nervosa
It is worth separating two things that are easy to blur: who first described the illness and who supplied its enduring name. The name anorexia nervosa is Gull’s. His own terminology evolved—from apepsia hysterica in his 1868 remark, to anorexia hysterica, and finally to anorexia nervosa, which he settled on by 1873–1874. He chose “nervosa” over “hysterica” deliberately, reasoning that the disorder was not confined to women (he had seen it in young men) and that “hysteria,” with its narrow and gendered connotations, was the wrong frame.
The literal meaning of the name is itself a small historical irony that still causes confusion. Anorexia means “loss of appetite,” yet clinicians have long understood that people with anorexia nervosa do not simply lose their appetite—the relationship to hunger and eating is far more complex than the word implies. The term has nonetheless endured for a century and a half, partly because Gull’s prestige helped fix it in the medical vocabulary and partly through sheer momentum. Lasègue’s anorexie hystérique, by contrast, faded as the “hysteria” framework fell out of medicine.
So the precise, defensible statement—the kind this history aims for—is this: Richard Morton gave an early medical description in 1689; Gull and Lasègue independently described the modern entity in 1873; and the term anorexia nervosa was coined by Gull (1873/1874). Keeping the first-descriptions, the independent French parallel, and the eponymous naming distinct from one another is the difference between accurate history and tidy myth.
Gerald Russell, 1979: Naming Bulimia Nervosa
For most of the century after 1873, “eating disorder” effectively meant anorexia nervosa. The recognition of a distinct second syndrome came surprisingly late and is attributable to one physician and one paper. The British psychiatrist Gerald Russell (1928–2018), working at the Royal Free Hospital in London, observed a group of patients who shared a particular pattern that did not fit the classic anorexic picture, and in 1979 he described and named it bulimia nervosa in the journal Psychological Medicine. He characterized it, memorably, as “an ominous variant of anorexia nervosa.”
Russell’s 1979 paper is the founding document of bulimia nervosa as a diagnosis, and its core description has held up well. He identified the central features as recurrent episodes of overeating, a powerful and distressing preoccupation with body weight, and behaviours intended to counteract food intake—a triad still at the heart of the modern definition. (In keeping with this page’s purpose, those compensatory behaviours are named only in general terms here.) Crucially, Russell noted that many of these patients had a prior history of anorexia nervosa, drawing a clinical link between the two conditions that subsequent research has repeatedly confirmed.
There is an old debate, distinct from Russell’s work, about whether bulimic-type behaviour existed in earlier eras—some historians point to descriptions of overeating and purging in antiquity. What is not in dispute is the medical milestone: bulimia nervosa was identified and named as a discrete clinical syndrome by Gerald Russell in 1979. That act gave clinicians a vocabulary, and patients a recognized diagnosis, for an illness that had previously hidden in the gaps of the classification.
Binge Eating Disorder and the Road to DSM-5
The third major eating disorder to be formally recognized, binge eating disorder (BED), travelled the longest road to official status. Its clinical roots reach back to 1959, when the American psychiatrist Albert Stunkard described a distinctive pattern of recurrent overeating among some people living with obesity—a pattern that did not involve the compensatory behaviours seen in bulimia nervosa. For decades, however, this observation had no diagnostic home of its own.
Formal recognition came in two stages. In 1994, the fourth edition of the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM-IV) introduced binge eating disorder only as a provisional category—a set of research criteria placed in an appendix and folded clinically under the catch-all label “Eating Disorder Not Otherwise Specified” (EDNOS), explicitly flagged as needing further study. It was not yet a stand-alone diagnosis. That changed in 2013, when the fifth edition (DSM-5), published in May of that year, established binge eating disorder as a distinct, free-standing eating disorder for the first time.
This matters for more than bookkeeping. Formal recognition in DSM-5 meant that BED—now understood to be more common than anorexia nervosa or bulimia nervosa—could be studied systematically, diagnosed consistently, billed and reimbursed by insurers, and treated with approaches validated for it specifically. The precise, verifiable claim is straightforward: binge eating disorder was first clinically described by Stunkard in 1959, was included provisionally in DSM-IV in 1994, and was added as a formal, standalone diagnosis in DSM-5 in 2013.
From Blame to Biology: A Biopsychosocial Illness
The way medicine explains why eating disorders happen has shifted profoundly, and the direction of that shift is humane. Earlier frameworks often located the cause in the individual or, worse, in the family—treating these illnesses as wilful behaviour, vanity, a “phase,” or the fault of parents. The modern consensus is very different: eating disorders are now understood as serious psychiatric illnesses arising from a biopsychosocial interplay of factors. Genetics and neurobiology, individual psychology and temperament, and social and cultural pressures all contribute, and no single one of them is the whole story.
The biological strand has become especially clear. Twin studies have long estimated the heritability of anorexia nervosa at roughly 50–60%, on the order of other major psychiatric disorders. In 2019 a large genome-wide association study led by Cynthia Bulik and the international Eating Disorders Working Group—combining nearly 17,000 cases with tens of thousands of controls—identified eight genetic loci and, importantly, found genetic correlations not only with other psychiatric conditions but also with metabolic traits. The authors proposed reconceptualizing anorexia nervosa as a “metabo-psychiatric” disorder. This is presented here as a leading and well-supported hypothesis rather than a closed case: it reframes part of the illness as rooted in biology that the person did not choose, which is both scientifically important and, for patients and families long burdened by blame, profoundly validating.
None of this erases the social dimension. Cultural pressures around thinness, appearance, and dieting are real and can act as triggers or amplifiers—but the modern view is careful to keep them in proportion: such pressures are one factor among many, not the sole cause, which is why eating disorders also occur in people and places far removed from any particular media environment, across genders, ages, body sizes, and cultures. The practical upshot of the biopsychosocial model is that eating disorders are treatable medical conditions deserving evidence-based care and compassion—not moral failings to be judged.
A Serious Illness: Mortality, Recovery, and Hope
The history of eating disorders has to include a sober fact, because taking these illnesses seriously is itself part of treating them with respect: anorexia nervosa carries one of the highest mortality rates of any psychiatric illness. Large reviews spanning decades of research find that people with anorexia nervosa die at several times the rate expected for their age, from a combination of the physical complications of starvation and from suicide. This is not stated to frighten anyone, and this page gives no figures that could be read as a grim “target”; it is stated because under-recognition and minimization—the old habit of dismissing these disorders as trivial or self-inflicted—cost lives, and because early, adequate treatment measurably improves the odds.
The far more important truth sits alongside it: eating disorders are treatable, and people recover. Effective, evidence-based treatments exist—including family-based treatment, which has a strong record for adolescents with anorexia nervosa, and structured psychotherapies such as cognitive behavioural therapy for bulimia nervosa and binge eating disorder—together with nutritional rehabilitation and medical care, and medication where appropriate. Recovery is not only possible but common, and the earlier help begins, the better it tends to go. Full, durable recovery happens at every age and every stage of illness.
If you or someone you care about is struggling, reaching out is a sign of strength, not weakness, and you do not have to be “sick enough” to deserve help. In the United States, the National Alliance for Eating Disorders runs a clinician-staffed helpline reachable at 1-866-662-1235, and its website (listed in External Authoritative Resources below) offers free support and treatment-finder tools. If you are in immediate crisis or thinking about suicide, call or text the 988 Suicide and Crisis Lifeline (dial 988 in the U.S.) at any hour. Help is real, it works, and it is available now.
Research Papers and References
The list below collects key peer-reviewed and historical sources behind this page’s account—Morton’s 1689 description, the 1873 Gull and Lasègue papers, Russell’s 1979 naming of bulimia nervosa, the medieval antecedents, and the modern genetics and outcome literature. Where a stable DOI or PMID was confidently identified it is linked directly; otherwise a curated PubMed topic search is provided. Each link opens at its source (DOI registrar, PubMed, or the U.S. National Library of Medicine) in a new tab.
- Bhanji S. Richard Morton’s account of “nervous consumption.” International Journal of Eating Disorders. 1985;4(4):589–595. — doi:10.1002/1098-108X(198511)4:4<589::AID-EAT2260040417>3.0.CO;2-P
- Morton R. Phthisiologia, or a Treatise of Consumptions (1689) — historical primary text; the first Western medical description of “nervous consumption.” (Full text, Internet Archive.) — archive.org: Phthisiologia (1689)
- Vandereycken W, van Deth R. A tribute to Lasègue’s description of anorexia nervosa (1873), with completion of its English translation. British Journal of Psychiatry. 1990;157:902–908. — PMID: 2289100
- Contemporary reflections on William Gull’s case studies of anorexia nervosa, 150 years on. European Eating Disorders Review. 2024. — doi:10.1002/erv.3139
- Pearce JMS. Richard Morton: origins of anorexia nervosa. European Neurology. 2004;52(4):191–192. — doi:10.1159/000082033
- Russell G. Bulimia nervosa: an ominous variant of anorexia nervosa. Psychological Medicine. 1979;9(3):429–448. — doi:10.1017/S0033291700031974 (PMID: 482466)
- Espi Forcen F. Anorexia mirabilis: the practice of fasting by Saint Catherine of Siena in the late Middle Ages. American Journal of Psychiatry. 2013;170(4):370–371. — doi:10.1176/appi.ajp.2012.12111457 (PMID: 23545792)
- Watson HJ, Yilmaz Z, Thornton LM, Bulik CM, et al. Genome-wide association study identifies eight risk loci and implicates metabo-psychiatric origins for anorexia nervosa. Nature Genetics. 2019;51(8):1207–1214. — doi:10.1038/s41588-019-0439-2
- Citrome L. Binge-eating disorder and the road to DSM-5 / clinical recognition — review literature. — PubMed: binge eating disorder, DSM-5 history and diagnosis
- Stunkard AJ. Eating patterns and obesity (the original 1959 description of binge eating). Psychiatric Quarterly. 1959;33:284–295. — PubMed: Stunkard, eating patterns and obesity (1959)
- Who was the first to describe anorexia nervosa: Gull or Lasègue? (priority and historiography) — PubMed: Gull vs Lasègue priority debate
- Mortality in anorexia nervosa and eating disorders (standardized mortality ratio; meta-analyses) — PubMed: anorexia nervosa mortality meta-analysis
- Family-based treatment and evidence-based outcomes in eating disorders — PubMed: eating disorder treatment and recovery
- History and conceptual evolution of eating disorders (overview reviews) — PubMed: history of eating disorders (review)
External Authoritative Resources
- National Institute of Mental Health (NIMH) — Eating Disorders
- National Alliance for Eating Disorders — free clinician-staffed helpline (1-866-662-1235) and treatment finder
- 988 Suicide & Crisis Lifeline (U.S.) — call or text 988
Connections
- Psychiatry
- Eating Disorders
- Depression
- Anxiety
- OCD (Obsessive-Compulsive Disorder)
- PTSD
- Anorexia Nervosa — the disorder Gull named in 1873 and the thread this history follows longest.
- All Conditions