Sciatica
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
1. Overview
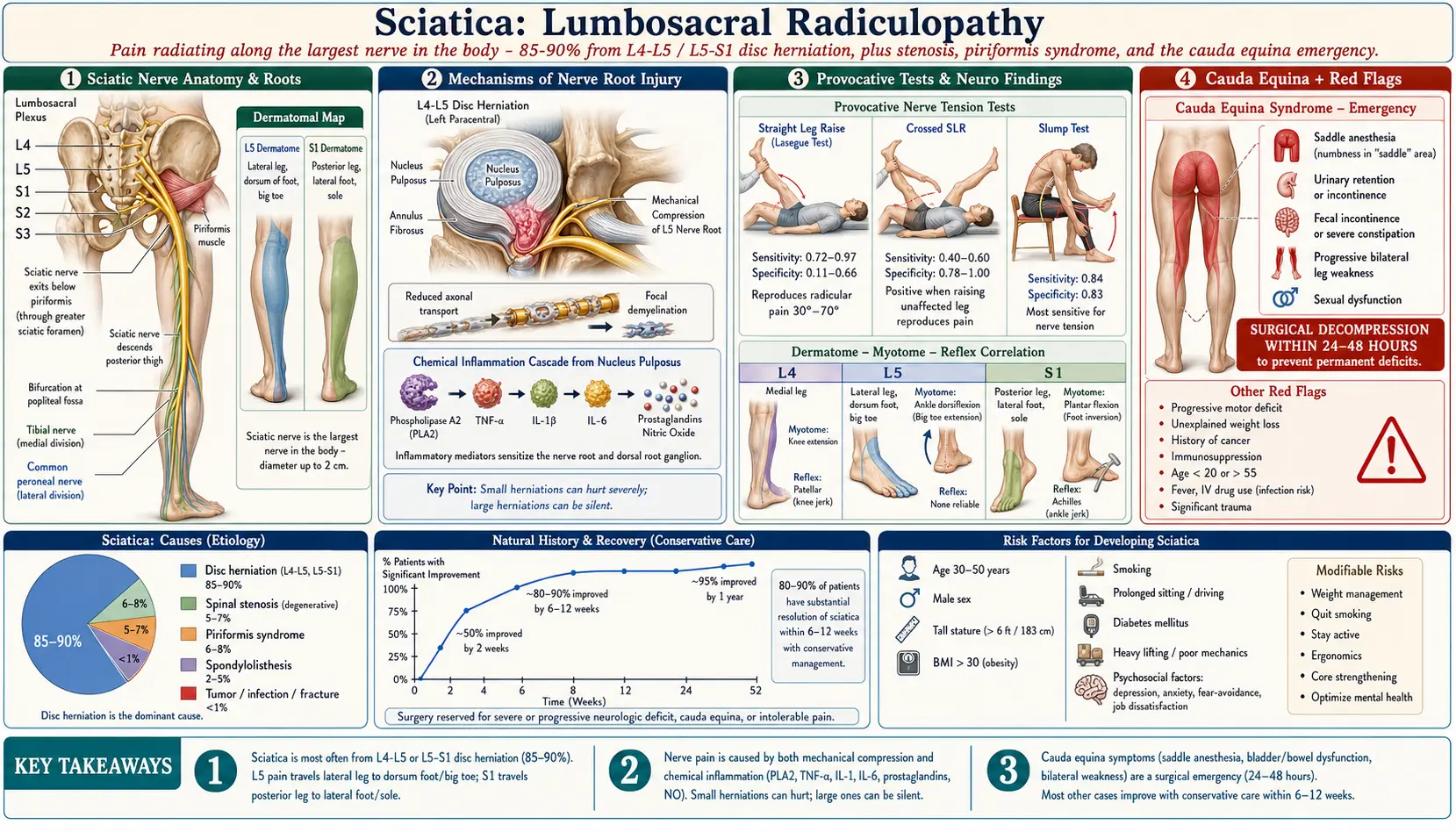
Sciatica is a clinical syndrome characterized by pain radiating along the distribution of the sciatic nerve, which extends from the lower back through the buttock and down the posterior or lateral aspect of the leg, often reaching below the knee into the calf, ankle, or foot. The term describes a symptom complex rather than a specific diagnosis, and it is most commonly caused by compression or irritation of the lumbosacral nerve roots (L4, L5, S1, S2, or S3) that form the sciatic nerve. The sciatic nerve is the largest and longest nerve in the human body, measuring approximately 2 cm in diameter and extending from the lumbosacral plexus to the distal lower extremity.
The most frequent cause of sciatica is a lumbar disc herniation, accounting for approximately 85-90% of cases, with the L4-L5 and L5-S1 levels most commonly involved. Other important causes include lumbar spinal stenosis, spondylolisthesis, piriformis syndrome, and less commonly, tumors, infections, or vascular malformations. The hallmark of sciatica is lumbar radiculopathy, a term that specifically refers to the neurological state in which nerve root function is compromised, resulting in a combination of radicular pain, sensory changes (numbness, paresthesias), motor weakness, and diminished reflexes in a dermatomal and myotomal distribution.
Sciatica is distinguished from nonspecific low back pain by the presence of leg-dominant pain that follows a dermatomal pattern, typically extending below the knee. The pain is often described as sharp, shooting, burning, or electric-shock-like in quality. It may be constant or intermittent and is frequently exacerbated by sitting, coughing, sneezing, or straining (activities that increase intradiscal pressure). Sciatica is a common and often debilitating condition that significantly impacts quality of life, work productivity, and healthcare utilization.
2. Epidemiology
Sciatica is one of the most common pain syndromes encountered in clinical practice. The lifetime prevalence of sciatica ranges from 13% to 40%, depending on the definition used and the population studied. The annual incidence is estimated at 1-5% of the general population. Sciatica accounts for approximately 5% of patients presenting with low back pain to primary care, yet it is disproportionately responsible for healthcare costs and disability.
The peak incidence occurs between ages 40 and 59, with a slight male predominance overall (male-to-female ratio of approximately 1.2-1.5:1), attributed to greater occupational mechanical loading. However, disc herniation-related sciatica shows relatively equal sex distribution, while spinal stenosis-related sciatica is slightly more common in women after age 60. In the United States, sciatica results in approximately $100 billion annually in direct and indirect costs, including medical care, lost wages, and disability payments.
Risk factors for sciatica include age 30-50 years (peak age for disc herniation), male sex, tall stature (height >180 cm), obesity (BMI >30), smoking, occupational exposure to heavy lifting, whole-body vibration, and prolonged sitting or driving. Diabetes mellitus increases the susceptibility of nerve roots to compression injury. Psychosocial factors including depression, anxiety, and job dissatisfaction are strongly associated with the transition from acute to chronic sciatica and predict poorer treatment outcomes.
3. Pathophysiology
Anatomy of the Sciatic Nerve
The sciatic nerve is formed from the ventral rami of the L4, L5, S1, S2, and S3 nerve roots, which converge in the pelvis to form the lumbosacral plexus. The nerve exits the pelvis through the greater sciatic foramen, typically passing below the piriformis muscle (though anatomical variants exist in approximately 12-21% of the population). It descends through the posterior thigh between the greater trochanter and the ischial tuberosity, passing deep to the gluteus maximus and the long head of the biceps femoris. At approximately the level of the popliteal fossa (posterior knee), the sciatic nerve divides into its two terminal branches: the tibial nerve (mediating plantar flexion and sensation to the sole) and the common peroneal nerve (mediating dorsiflexion, eversion, and sensation to the dorsum of the foot and lateral leg).
Mechanisms of Nerve Root Injury
The pathophysiology of sciatica involves two primary mechanisms that typically occur in combination:
- Mechanical compression: Direct physical compression of the nerve root by a herniated disc, osteophyte, or narrowed foramen reduces axonal transport, impairs nerve blood supply (vasa nervorum), and causes focal demyelination. The degree of compression correlates with the severity of motor and sensory deficits but does not always correlate with pain intensity.
- Chemical inflammation: The nucleus pulposus of a herniated disc contains potent inflammatory mediators including phospholipase A2, tumor necrosis factor-alpha (TNF-alpha), interleukin-1 (IL-1), interleukin-6 (IL-6), prostaglandins, and nitric oxide. These substances cause direct nerve root inflammation, increased capillary permeability, and sensitization of nociceptors even in the absence of direct mechanical compression. This explains why patients with small herniations can have severe pain, while large herniations may be asymptomatic.
Neuroimmune Response
When disc material contacts the nerve root, an autoimmune-mediated inflammatory cascade is triggered. The nucleus pulposus, normally sequestered from the immune system within the avascular disc, is recognized as foreign when exposed through herniation. Macrophages and T-lymphocytes infiltrate the herniation site, releasing cytokines that further sensitize nerve fibers. This immune response, while responsible for pain generation, also plays a crucial role in the natural resorption of herniated disc material. Phagocytic resorption of the herniated fragment typically occurs over 6-12 months, with larger extrusions paradoxically showing faster and more complete resorption than smaller contained protrusions.
Central Sensitization
In chronic sciatica, central sensitization develops in the dorsal horn of the spinal cord and supraspinal pain processing centers. Persistent nociceptive input from the inflamed nerve root causes upregulation of NMDA receptors, wind-up phenomena, and expansion of receptive fields, resulting in amplified pain perception, allodynia (pain from normally non-painful stimuli), and hyperalgesia (exaggerated pain response). Central sensitization contributes to the persistence of pain even after the peripheral pathology has resolved and is a key target for treatment in chronic sciatica.
4. Etiology and Risk Factors
Lumbar Disc Herniation (85-90% of cases)
- L5-S1 disc herniation: The most common level, compressing the S1 nerve root. Produces pain radiating down the posterior thigh and calf to the lateral foot, diminished ankle jerk reflex, and weakness of plantar flexion (difficulty standing on tiptoes).
- L4-L5 disc herniation: Compresses the L5 nerve root. Produces pain radiating down the lateral thigh and leg to the dorsum of the foot and great toe, weakness of ankle dorsiflexion and great toe extension (foot drop), and no characteristic reflex change.
- L3-L4 disc herniation: Compresses the L4 nerve root. Produces pain radiating to the medial leg and ankle, weakness of knee extension (quadriceps), and diminished patellar reflex. Less common than L4-L5 and L5-S1.
Lumbar Spinal Stenosis
- Central stenosis: Narrowing of the central spinal canal, typically from degenerative disc disease, facet joint hypertrophy, and ligamentum flavum thickening. Causes neurogenic claudication: bilateral leg pain, numbness, and weakness worsened by walking and standing, relieved by sitting and forward flexion.
- Foraminal stenosis: Narrowing of the neural foramen where the nerve root exits, often from a combination of disc height loss, facet hypertrophy, and osteophyte formation. Produces unilateral radiculopathy.
- Lateral recess stenosis: Narrowing of the lateral recess where the traversing nerve root passes, typically from facet and ligamentum flavum hypertrophy.
Piriformis Syndrome
- Compression of the sciatic nerve by the piriformis muscle as it passes through the greater sciatic foramen
- Accounts for an estimated 6-8% of sciatica cases, though the true prevalence is debated
- More common in women (6:1 female-to-male ratio)
- Associated with anatomical variants: in 12-21% of the population, the sciatic nerve pierces the piriformis muscle or splits around it
- Provocative tests include the FAIR test (flexion, adduction, internal rotation), Pace sign, and Freiberg test
Other Causes
- Spondylolisthesis: Forward slippage of one vertebra on another, causing foraminal narrowing and nerve root compression
- Tumors: Primary or metastatic tumors of the spine, nerve sheath tumors (schwannomas, neurofibromas)
- Infections: Epidural abscess, vertebral osteomyelitis, discitis
- Sacroiliac joint dysfunction: May refer pain into the buttock and posterior thigh, mimicking sciatica
- Endometriosis: Cyclical sciatic pain in women from endometrial implants on the sciatic nerve
- Vascular causes: Iliac artery aneurysm, pelvic venous congestion
- Trauma: Pelvic fractures, hip dislocations, penetrating injuries
5. Clinical Presentation
Cardinal Symptoms
The defining feature of sciatica is unilateral leg pain that follows a dermatomal distribution, typically radiating from the lower back or buttock through the posterior or posterolateral thigh and below the knee. Key symptom characteristics include:
- Pain quality: Sharp, shooting, burning, or electric shock-like. Often described as lancinating or stabbing. The leg pain is typically worse than the back pain.
- Pain distribution: Follows the dermatome of the affected nerve root. L5 radiculopathy produces pain along the lateral leg to the dorsum of the foot. S1 radiculopathy produces pain along the posterior leg to the lateral foot and sole.
- Aggravating factors: Sitting, coughing, sneezing, straining (Valsalva maneuver), forward bending, and prolonged standing.
- Relieving factors: Lying supine with knees bent, walking (for disc herniation), sitting (for spinal stenosis, opposite of disc-related sciatica).
- Numbness and paresthesias: Tingling, pins-and-needles, or reduced sensation in the affected dermatome.
- Weakness: In the myotome of the affected root. L5: foot drop, difficulty walking on heels. S1: difficulty walking on tiptoes, reduced push-off during gait.
Red Flag Symptoms Requiring Urgent Evaluation
Certain features warrant urgent investigation to rule out serious underlying pathology:
- Cauda equina syndrome: Bilateral leg pain or weakness, saddle anesthesia (numbness of the perineum, inner thighs, and buttocks), urinary retention or incontinence, fecal incontinence, progressive bilateral motor weakness. This is a surgical emergency requiring decompression within 24-48 hours.
- Progressive motor deficit: Rapidly worsening weakness, particularly foot drop, indicates worsening nerve compression requiring urgent surgical evaluation.
- Constitutional symptoms: Unexplained weight loss, fever, night sweats, or severe unremitting pain at rest suggest possible malignancy or infection.
- History of cancer: New sciatica in a patient with known malignancy raises concern for spinal metastasis.
- Immunosuppression, IV drug use, or recent spinal procedure: Risk factors for epidural abscess.
- Age <20 or >55: First-time sciatica in these age groups warrants broader evaluation beyond disc herniation.
Physical Examination Findings
- Straight leg raise (SLR/Lasegue's test): Reproduction of sciatic pain at 30-70 degrees of passive hip flexion with the knee extended. Sensitivity: 91%; specificity: 26%. Pain must radiate below the knee to be considered positive.
- Crossed SLR (contralateral SLR): Reproduction of the affected leg's pain when the unaffected leg is raised. Lower sensitivity (29%) but high specificity (88%) for disc herniation.
- Slump test: Patient sits with spine flexed, neck flexed, and the affected leg is passively extended. More sensitive than SLR for detecting neural tension.
- Dermatomal sensory testing: Reduced light touch or pinprick sensation in the affected dermatome.
- Motor strength testing: Ankle dorsiflexion (L4-L5), great toe extension (L5), ankle plantar flexion (S1), hip abduction (L5).
- Deep tendon reflexes: Diminished patellar reflex (L4), diminished ankle jerk (S1).
6. Diagnosis
Clinical Diagnosis
Sciatica is primarily a clinical diagnosis based on history and physical examination. Imaging is not routinely indicated in the initial evaluation unless red flag symptoms are present or symptoms persist beyond 6-8 weeks of conservative treatment. The clinical diagnosis is supported by the combination of radicular leg pain below the knee, positive provocative nerve tension tests, and neurological findings consistent with a specific nerve root level.
Imaging Studies
- MRI of the lumbar spine: The gold standard imaging modality for evaluating sciatica. MRI provides excellent visualization of disc herniations, nerve root compression, spinal stenosis, tumors, and infections without radiation exposure. Important caveat: MRI has a high rate of incidental findings, studies demonstrate that 30-40% of asymptomatic adults have disc herniations visible on MRI. Therefore, imaging findings must always be correlated with clinical symptoms.
- CT scan: Provides superior bony detail compared to MRI and is useful for evaluating foraminal stenosis, spondylolisthesis, and fractures. CT myelography is the preferred alternative when MRI is contraindicated.
- Plain radiographs (X-rays): Limited role in evaluating sciatica but useful for assessing spinal alignment, spondylolisthesis, fractures, and bony tumors. Flexion-extension lateral views assess for instability.
Electrodiagnostic Studies
- Electromyography (EMG) and nerve conduction studies (NCS): Useful when the diagnosis is uncertain, when clinical and imaging findings are discordant, or when the severity of nerve root injury needs to be quantified. EMG can differentiate radiculopathy from peripheral neuropathy, plexopathy, or other neuromuscular conditions. Fibrillation potentials on needle EMG indicate active denervation and confirm physiologically significant nerve root compression. EMG findings typically take 2-3 weeks to develop after the onset of nerve injury.
Diagnostic Nerve Blocks
- Selective nerve root blocks (SNRB): Fluoroscopically or CT-guided injection of local anesthetic and corticosteroid around a specific nerve root. Concordant pain relief confirms the symptomatic level, which is particularly valuable in multilevel degenerative disease where the primary pain generator is uncertain.
7. Treatment
Conservative Management (First-Line)
The majority of sciatica cases (80-90%) resolve with conservative treatment within 6-12 weeks. Guidelines recommend an initial trial of conservative therapy before considering invasive interventions:
- Activity modification: Avoid prolonged bed rest (limit to 1-2 days if needed). Early return to normal activities as tolerated is strongly recommended. Gentle walking is encouraged.
- Pharmacotherapy:
- NSAIDs (ibuprofen 400-800 mg TID, naproxen 500 mg BID): First-line analgesics, providing anti-inflammatory and pain-relieving effects.
- Acetaminophen: May be used as an alternative or adjunct, though evidence for efficacy in sciatica specifically is limited.
- Oral corticosteroids: Short-course prednisone taper (60 mg tapering over 5-7 days) provides modest short-term benefit.
- Gabapentin (300-3600 mg daily) or pregabalin (75-300 mg BID): For neuropathic pain components (burning, shooting, electric shock sensations).
- Muscle relaxants (cyclobenzaprine 10 mg TID, tizanidine 4 mg TID): For associated muscle spasm.
- Opioids: Reserved for severe acute sciatica unresponsive to other measures; limited to short courses (7-14 days) due to addiction risk and lack of long-term benefit evidence.
Physical Therapy
- McKenzie method (Mechanical Diagnosis and Therapy): A systematic approach using directional preference exercises to centralize and reduce radicular pain. Extension-based exercises are effective for most posterior disc herniations.
- Core stabilization: Strengthening of the transversus abdominis, multifidus, and pelvic floor muscles to improve spinal stability and reduce recurrence.
- Neural mobilization (neurodynamics): Specific exercises to mobilize the sciatic nerve and reduce neural tension, including sciatic nerve sliders and tensioners.
- Manual therapy: Spinal mobilization and manipulation can reduce pain and improve function in the acute phase.
Interventional Pain Management
- Epidural steroid injections (ESIs): Injection of corticosteroid (methylprednisolone 80 mg or triamcinolone 80 mg) with local anesthetic into the epidural space. Three approaches exist: interlaminar (most common), transforaminal (most target-specific), and caudal. ESIs provide significant short-term pain relief (2-6 weeks) in 60-84% of patients and serve as a bridge to allow participation in physical therapy. Generally limited to 3 injections per year.
- Selective nerve root blocks: Targeted injection around the specific affected nerve root under fluoroscopic guidance.
Surgical Treatment
Surgery is indicated for patients who fail 6-12 weeks of conservative treatment, those with progressive neurological deficits, or patients presenting with cauda equina syndrome:
- Microdiscectomy: The gold standard surgical procedure for disc-related sciatica. Through a small incision (2-3 cm), the surgeon uses an operating microscope to remove the herniated disc fragment compressing the nerve root. Success rate: 85-92% for relief of leg pain. Average recovery time: 4-6 weeks. The landmark SPORT trial demonstrated that surgery provides faster pain relief than conservative treatment, but long-term outcomes (4-year, 8-year) are comparable.
- Laminectomy/laminotomy: Removal of a portion of the lamina to decompress the spinal canal and nerve roots. Primary treatment for spinal stenosis-related sciatica.
- Lumbar fusion: Indicated when sciatica is accompanied by instability (spondylolisthesis) or significant degenerative disc disease requiring stabilization.
- Artificial disc replacement: An alternative to fusion for single-level disc disease, preserving motion at the treated segment.
8. Complications
- Chronic sciatica: Approximately 20-30% of patients with acute sciatica develop chronic pain lasting beyond 12 weeks, significantly impacting quality of life and functional capacity.
- Cauda equina syndrome: A rare but devastating complication of large disc herniations, occurring in approximately 1-3% of disc herniation patients. Delay in surgical decompression beyond 48 hours significantly increases the risk of permanent bladder dysfunction, bowel dysfunction, and sexual dysfunction.
- Foot drop: Progressive L5 radiculopathy can cause significant ankle dorsiflexion weakness (foot drop), requiring an ankle-foot orthosis and potentially surgical decompression. Recovery depends on the duration and severity of nerve compression.
- Muscle atrophy: Chronic denervation of affected myotomes leads to progressive muscle wasting, particularly of the tibialis anterior (L5), gastrocnemius (S1), and quadriceps (L4).
- Chronic pain and disability: Central sensitization, psychological comorbidities (depression, anxiety, catastrophizing), and deconditioning contribute to chronic pain states.
- Surgical complications: Recurrent disc herniation (5-15%), dural tear (1-7%), nerve root injury (<1%), infection (1-2%), epidural hematoma, and failed back surgery syndrome.
- Medication-related complications: NSAID-induced gastropathy, opioid dependence, gabapentinoid sedation and dizziness.
- Depression and psychosocial deterioration: Chronic sciatica is strongly associated with depression (prevalence 40-60%), anxiety, sleep disturbance, and reduced social participation.
- Featured Videos
9. Prognosis
The natural history of sciatica is generally favorable. The majority of patients (80-90%) experience significant improvement within 6-12 weeks, regardless of whether the underlying cause is a disc herniation. This favorable prognosis reflects the natural resorption of herniated disc material by the immune system, with imaging studies demonstrating partial or complete resorption of herniated disc fragments in 60-70% of cases over 6-12 months. Larger disc extrusions and sequestrations paradoxically show faster and more complete resorption than smaller contained protrusions.
For patients treated with microdiscectomy, immediate surgical outcomes are excellent, with 85-92% of patients reporting significant relief of leg pain within days of surgery. The SPORT trial and other landmark studies have demonstrated that while surgery provides faster relief than conservative treatment, the long-term outcomes at 4-10 years are comparable between surgical and non-surgical groups. However, patients with severe pain and significant functional limitations may benefit from earlier surgical intervention to reduce the duration of suffering and disability.
Negative prognostic factors for recovery include longer duration of symptoms before treatment, severe motor deficit at presentation, smoking, psychological comorbidities (depression, anxiety, catastrophizing), workers' compensation or litigation involvement, lower education level, and heavy physical job demands. Patients with spinal stenosis-related sciatica tend to have a more gradual onset and slower progression, but symptoms may worsen over time without surgical decompression. The recurrence rate of sciatica after a first episode is approximately 25-30% over 5 years, emphasizing the importance of long-term preventive strategies.
10. Prevention
- Core muscle strengthening: A strong core (transversus abdominis, multifidus, pelvic floor) provides dynamic stability to the lumbar spine and reduces the mechanical load on intervertebral discs. Regular engagement in programs such as Pilates, yoga, or targeted core exercises reduces sciatica recurrence by up to 30-50%.
- Proper lifting mechanics: Bend at the knees and hips rather than the waist, keep the load close to the body, avoid twisting while lifting, and use mechanical aids for heavy objects. Intradiscal pressure is minimized with a neutral spine posture during lifting.
- Maintain healthy body weight: Every additional 10 pounds of body weight increases compressive forces on the lumbar spine by approximately 40 pounds. Weight loss in obese patients significantly reduces sciatica risk and recurrence.
- Smoking cessation: Smoking accelerates disc degeneration by reducing blood flow to the disc, impairing nutrient delivery, and promoting inflammatory pathways. Cessation improves disc health and treatment outcomes.
- Ergonomic workplace design: Adjustable chairs with lumbar support, sit-stand workstations, proper monitor height, and regular movement breaks reduce sustained compressive loading on the lumbar spine.
- Regular physical activity: Moderate aerobic exercise (walking, swimming, cycling) maintains disc hydration and nutrition, promotes spinal flexibility, and reduces inflammatory mediators.
- Avoid prolonged static postures: Prolonged sitting increases intradiscal pressure by 40% compared to standing. Take breaks every 30-45 minutes to stand, stretch, and walk.
- Hamstring and hip flexor flexibility: Tight hamstrings and hip flexors alter pelvic mechanics and increase stress on the lumbar spine. Regular stretching programs reduce mechanical loading on the discs.
- Sleep posture: Sleeping in a side-lying position with a pillow between the knees or supine with a pillow under the knees maintains neutral spinal alignment.
11. Recent Research and Advances
Recent research in sciatica has focused on refining treatment algorithms, developing novel therapeutics, and improving patient selection for surgery. The NERVES trial (2020), a large pragmatic randomized trial, investigated early referral for MRI and possible surgery versus continued primary care management, finding that early MRI did not lead to better outcomes at 12 months, reinforcing the recommendation to reserve imaging for persistent or red-flag cases.
Biological therapies targeting the inflammatory cascade are under active investigation. Anti-TNF-alpha agents (adalimumab, infliximab, etanercept) have been studied in several randomized trials for sciatica refractory to conventional treatment, with mixed results. Intradiscal injection of mesenchymal stem cells (MSCs) is being explored for disc regeneration, with early phase trials showing promising results in promoting disc hydration and reducing pain. Platelet-rich plasma (PRP) injected epidurally or periradicularly has shown encouraging results in small trials, potentially offering longer-lasting relief than corticosteroid injections through anti-inflammatory and regenerative mechanisms.
Advances in minimally invasive surgery continue to reduce morbidity. Full-endoscopic interlaminar and transforaminal discectomy techniques using tubular retractors and endoscopic visualization offer reduced tissue trauma, shorter hospital stays, and faster recovery compared to traditional microdiscectomy, with comparable outcomes. Artificial intelligence and machine learning applications are being developed to predict which patients will benefit most from surgery versus conservative management, potentially enabling personalized treatment decisions. The growing recognition of psychosocial factors in sciatica outcomes has led to the integration of cognitive behavioral therapy (CBT) and acceptance and commitment therapy (ACT) into multidisciplinary treatment programs, with evidence supporting improved outcomes when psychological interventions are combined with physical treatments.
12. References & Research
Historical Background
The term "sciatica" has ancient origins, derived from the Greek word ischiadikos (meaning "pain in the hip joint"). Hippocrates (460-370 BCE) provided the first known clinical description of sciatic pain, referring to it as "ischias." The connection between disc herniation and sciatica was not established until 1934, when William Jason Mixter and Joseph Barr published their landmark paper in the New England Journal of Medicine demonstrating that ruptured intervertebral discs were the primary cause of sciatica, fundamentally changing the understanding and treatment of this condition. Alf Nachemson performed pioneering intradiscal pressure measurements in the 1960s that provided the biomechanical foundation for understanding spinal loading. Robin McKenzie developed his mechanical diagnosis and therapy method in 1981, revolutionizing conservative treatment of disc-related sciatica.
Key Research Papers
- Mixter WJ, Barr JS. Rupture of the intervertebral disc with involvement of the spinal canal. New England Journal of Medicine. 1934;211(5):210-215.
- Weinstein JN, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the SPORT randomized trial. JAMA. 2006;296(20):2441-2450.
- Peul WC, et al. Surgery versus prolonged conservative treatment for sciatica. New England Journal of Medicine. 2007;356(22):2245-2256.
- Jensen MC, et al. Magnetic resonance imaging of the lumbar spine in people without back pain. New England Journal of Medicine. 1994;331(2):69-73.
- Lurie JD, et al. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the SPORT. Spine. 2014;39(1):3-16.
- Koes BW, van Tulder MW, Peul WC. Diagnosis and treatment of sciatica. BMJ. 2007;334(7607):1313-1317.
- Jacobs WC, et al. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review. European Spine Journal. 2011;20(4):513-522.
- Atlas SJ, et al. Long-term outcomes of surgical and nonsurgical management of sciatica. Spine. 2005;30(8):927-935.
- Vroomen PC, et al. Conservative treatment of sciatica: a systematic review. Journal of Spinal Disorders. 2000;13(6):463-469.
- Chou R, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline. Annals of Internal Medicine. 2007;147(7):478-491.
- Battie MC, et al. The Twin Spine Study: contributions to a changing view of disc degeneration. The Spine Journal. 2009;9(1):47-59.
- Stafford MA, et al. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection. British Journal of Anaesthesia. 2007;99(4):461-473.
- Kreiner DS, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. The Spine Journal. 2014;14(1):180-191.
- Ropper AH, Zafonte RD. Sciatica. New England Journal of Medicine. 2015;372(13):1240-1248.
- Konstantinou K, Dunn KM. Sciatica: review of epidemiological studies and prevalence estimates. Spine. 2008;33(22):2464-2472.
Research Papers
- Clinical trials on sciatica — PubMed search
- Systematic reviews of sciatica — PubMed search
- Meta-analyses on sciatica — PubMed search
- Treatment research on sciatica — PubMed search
- Mechanism studies of sciatica — PubMed search
- Epidemiology of sciatica — PubMed search
Connections
- Herniated Disc
- Tendinitis
- Fibromyalgia
- Magnesium
- Turmeric
- Anti-Inflammatory Diet
- Stress Management
- Chronic Pain
- Depression
- Anxiety
- Peripheral Neuropathy
- Carpal Tunnel Syndrome
- Obesity
- Diabetes
- Chronic Low Back Pain Evidence Based Care
- Interventional Pain
- Osteoarthritis
- Plantar Fasciitis
- Low Back Pain