Concussion
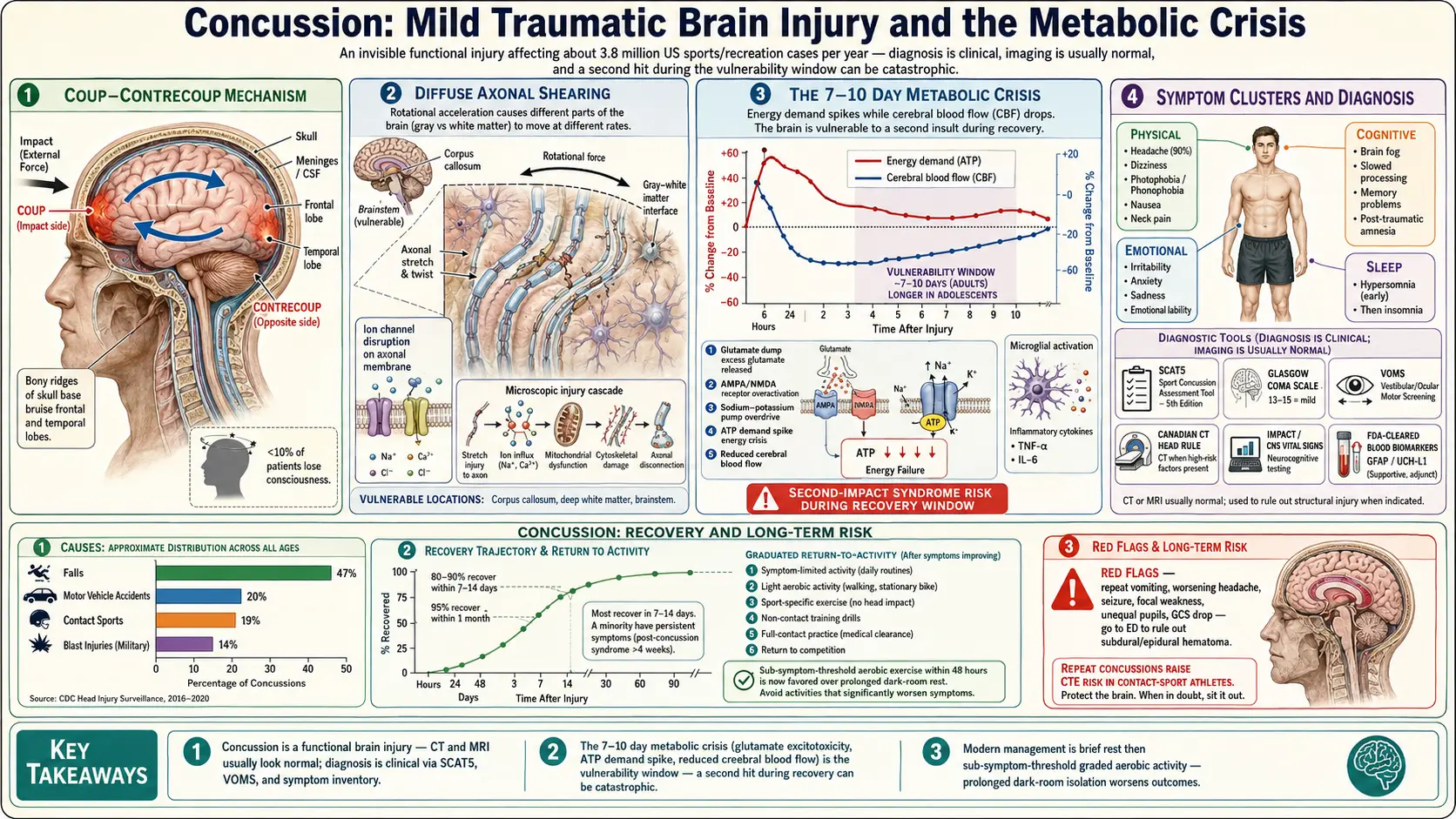
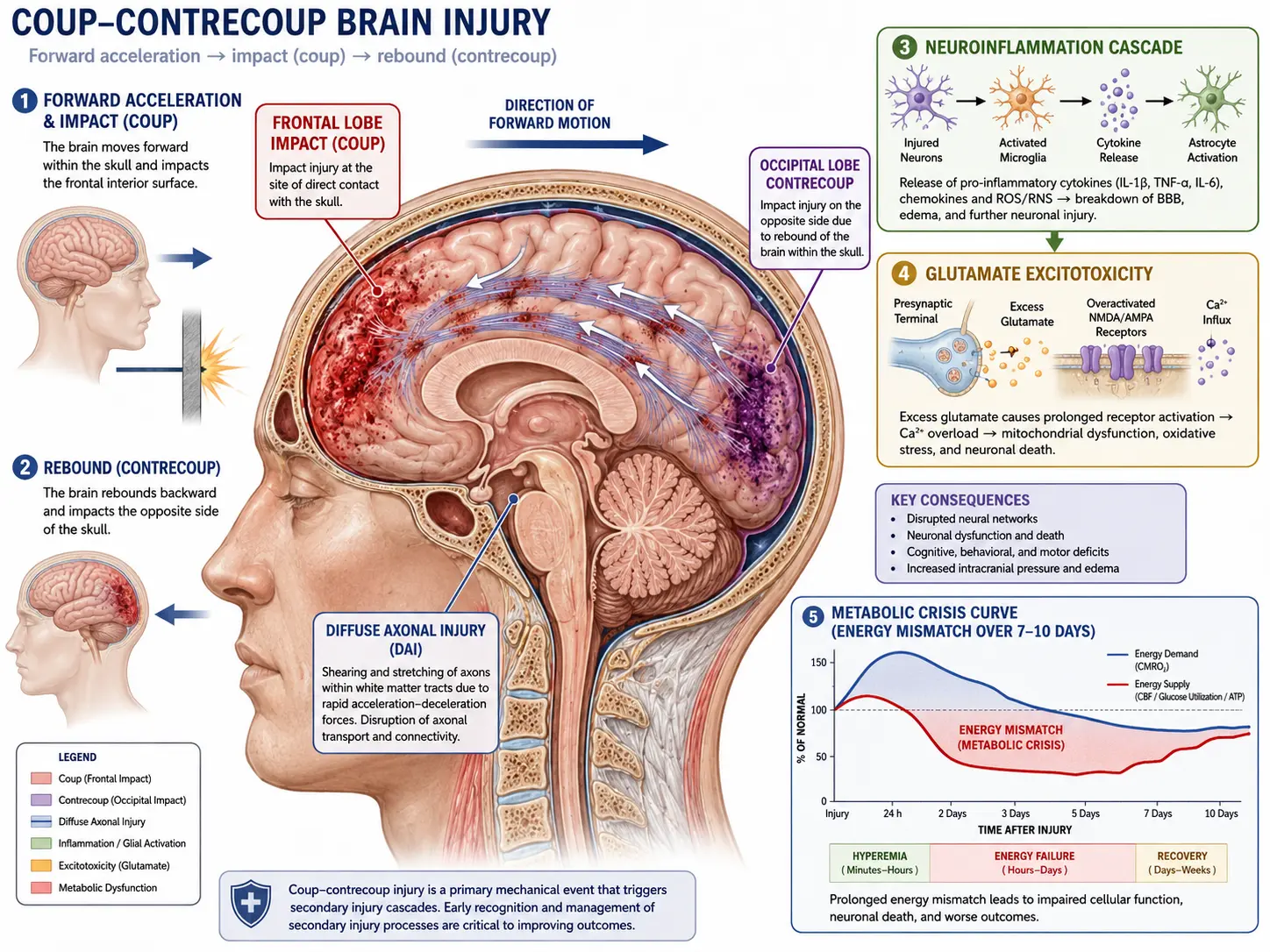
Table of Contents
- What is a Concussion?
- Mechanism of Injury
- Symptoms
- Diagnosis
- Management and Recovery
- Post-Concussion Syndrome and CTE Concerns
- Prevention
- Research Papers
- Connections
- Featured Videos
What is a Concussion?
A concussion is a mild traumatic brain injury (mTBI) caused by a bump, blow, or jolt to the head — or by a hit to the body that causes the head and brain to move rapidly back and forth. Even though the word "mild" is used, a concussion is a real brain injury that temporarily disrupts how nerve cells signal each other and how the brain regulates blood flow, energy, and chemistry. Most concussions occur without loss of consciousness; in fact, fewer than 10% of patients black out.
Concussions are remarkably common. In the United States, an estimated 3.8 million sports- and recreation-related concussions occur each year, and that figure understates the true total because many cases never reach a doctor. The three biggest sources are falls (the leading cause across all ages, especially in children under 5 and adults over 65), motor vehicle accidents, and contact sports such as football, hockey, soccer, rugby, lacrosse, and boxing/MMA. Military service members — particularly those exposed to blast injuries — also carry an elevated risk.
The hallmark of a concussion is that standard CT and MRI scans usually look normal. The injury is functional rather than structural — the wiring is intact, but it isn't firing the way it should. That's why concussions have historically been called "invisible injuries," and why diagnosis depends on careful symptom assessment rather than imaging alone.
Mechanism of Injury
The image at the top of this page summarizes what happens inside the skull during a concussion. Three overlapping processes drive the injury:
1. Coup-Contrecoup Injury
When the head is struck or rapidly decelerated, the brain — which floats in cerebrospinal fluid — slams into the inside of the skull at the point of impact (the coup) and then rebounds and hits the opposite side (the contrecoup). The frontal lobes (judgment, executive function) and temporal lobes (memory, mood) are especially vulnerable because they sit against bony ridges inside the skull. This is why concussion symptoms so often involve thinking, mood, and memory rather than obvious motor weakness.
2. Diffuse Axonal Shearing
The brain is not uniformly dense — gray matter and white matter accelerate and decelerate at slightly different rates during sudden rotational forces. That difference stretches and twists the long signal-carrying fibers of nerve cells (axons), particularly in the corpus callosum and brainstem. Axons may not snap outright, but the stretching disrupts ion channels and triggers a cascade of microscopic damage. This diffuse axonal injury is a major reason concussions can cause widespread symptoms even when no single brain region looks injured on a scan.
3. Neuroinflammation, Glutamate Excitotoxicity, and the Metabolic Crisis
In the first seconds after impact, stretched neurons dump glutamate, the brain's main excitatory neurotransmitter, into the surrounding tissue. This forces neighboring cells to fire uncontrollably, which in turn forces sodium-potassium pumps into overdrive to restore their resting state. Restoring balance burns enormous amounts of ATP (cellular energy) at exactly the moment when blood flow to the brain has dropped. The result is a metabolic mismatch: energy demand spikes while energy supply falls.
This mismatch curve typically lasts 7 to 10 days in adults and longer in adolescents. During that window, neurons are functional but fragile — this is the vulnerability period, and it is the single most important reason that a second hit during recovery is so dangerous. Microglia, the brain's resident immune cells, are also activated; their inflammatory signaling helps clear damage but also drives many of the symptoms (headache, fatigue, brain fog) and, if it persists, contributes to post-concussion syndrome.
Symptoms
Concussion symptoms fall into four overlapping clusters. Many symptoms are delayed by hours or even days — a person can walk away from a hit feeling fine, then feel terrible the next morning. That's not a sign the original assessment was wrong; it's how the metabolic cascade unfolds.
Physical (Somatic) Symptoms
- Headache — the most common symptom, present in roughly 90% of cases
- Dizziness and balance problems
- Nausea or vomiting (especially in the first 24 hours)
- Visual disturbances: blurred vision, double vision, sensitivity to light (photophobia)
- Sensitivity to noise (phonophobia)
- Fatigue — out of proportion to activity
- Neck pain (concussion and whiplash often happen together)
Cognitive Symptoms
- Confusion, "feeling in a fog"
- Difficulty concentrating — reading and screen use feel exhausting
- Memory problems — trouble forming new memories or recalling the event itself (post-traumatic amnesia)
- Slowed thinking and reaction time
Emotional Symptoms
- Irritability, short fuse
- Anxiety or feeling on edge
- Sadness or low mood
- Emotional lability — tearful or angry over small things
Sleep Symptoms
- Sleeping more than usual in the first few days
- Insomnia — trouble falling or staying asleep, often emerging after the first week
- Drowsiness during the day
- Disrupted sleep architecture (less restorative deep and REM sleep)
Red-flag symptoms that require emergency evaluation include repeated vomiting, worsening headache, seizures, weakness or numbness on one side, slurred speech, unequal pupils, loss of consciousness lasting more than a minute, or progressive confusion. These can signal a more serious bleed (subdural or epidural hematoma) rather than an uncomplicated concussion.
Diagnosis
Concussion is fundamentally a clinical diagnosis — meaning it is made by a clinician interviewing and examining the patient, not by a single test. Because routine imaging is usually normal, the diagnostic toolkit relies on structured symptom inventories, cognitive screens, and physical exams of balance and eye movement.
Clinical Assessment Tools
- SCAT5 (Sport Concussion Assessment Tool, 5th edition): the international standard sideline and clinic tool. It combines symptom checklists, orientation questions, immediate and delayed memory, concentration tasks (digits backward, months in reverse), and a balance error scoring system. A child version (Child SCAT5) exists for ages 5–12.
- Glasgow Coma Scale (GCS): a 3- to 15-point scale measuring eye opening, verbal response, and motor response. Most concussions score 13–15 (the "mild" range). Lower scores indicate a more serious brain injury.
- Vestibular/Ocular Motor Screening (VOMS): a brief exam that provokes symptoms with smooth pursuit, saccades, near-point convergence, and vestibulo-ocular reflex tasks. VOMS is highly sensitive — many concussion patients with normal SCAT5 scores still show abnormalities here.
Neuroimaging
CT scan is reserved for patients with red-flag symptoms or a meaningful risk of intracranial bleeding (older age, anticoagulant use, focal neurologic findings, persistent vomiting, GCS <15). The Canadian CT Head Rule and New Orleans Criteria help triage who actually needs imaging — the goal is to avoid unnecessary radiation, especially in children.
MRI is generally not needed in uncomplicated concussion, but advanced sequences such as diffusion tensor imaging (DTI) can detect white-matter changes invisible on standard imaging and are increasingly used in research and persistent cases.
Neurocognitive Testing
Computerized neurocognitive tests — ImPACT, CNS Vital Signs, ANAM — measure reaction time, working memory, attention, and processing speed. These are most useful when a baseline was performed before injury (common in collegiate and professional athletes), giving a personal benchmark to recover toward. Without a baseline, the tests still help track progress over time.
Emerging Blood Biomarkers
The FDA has cleared blood tests measuring GFAP (glial fibrillary acidic protein) and UCH-L1 (ubiquitin C-terminal hydrolase L1) — the Banyan Brain Trauma Indicator — to help decide which adult patients with mTBI can safely skip a CT scan. They are not a stand-alone concussion diagnosis but are reshaping how emergency departments triage head injury.
Management and Recovery
Concussion management has changed substantially in the past decade. The old advice of "rest in a dark room until you're 100%" is now considered counterproductive; prolonged inactivity worsens mood, sleep, and recovery. The current evidence-based approach is built on a brief rest period followed by a graded return to activity.
Initial 24–48 Hours: Relative Rest
- Cognitive rest: limit (don't necessarily eliminate) screens, schoolwork, and demanding mental tasks
- Physical rest: avoid exercise, sports, and anything with a meaningful risk of a second hit
- Sleep: sleep is fine and helpful — the old advice to wake someone up every hour is no longer recommended for routine concussions
- Hydration and nutrition: dehydration worsens headaches and fatigue
- Avoid alcohol and recreational drugs during recovery
Days 2–3 Onward: Sub-Symptom-Threshold Activity
After the first 24–48 hours, the goal becomes "do as much as you can without making symptoms worse." Light walking, gentle stretching, short bouts of reading, and limited screen time are encouraged. If any activity provokes a noticeable spike in symptoms, scale back — but don't retreat to bed-rest. Studies show patients who begin light aerobic activity within the first week recover faster than those who wait.
Sleep Hygiene
Sleep quality drives recovery. Useful steps include keeping a consistent sleep schedule, avoiding screens for 60 minutes before bed, eliminating caffeine after noon, and treating any emergent insomnia early. See the Sleep Hygiene remedy page for detailed protocols.
Graduated Return-to-Play / Return-to-Learn
Athletes follow a six-stage return-to-play protocol developed by the Concussion in Sport Group:
- Symptom-limited daily activities (e.g., walking around the house)
- Light aerobic exercise (stationary bike, easy jog — heart rate <70% max)
- Sport-specific exercise (running drills, no contact)
- Non-contact training drills (passing, more complex movements)
- Full-contact practice (after medical clearance)
- Return to play
Each stage takes a minimum of 24 hours; if symptoms reappear at any stage, the athlete drops back a level and waits 24 hours before retrying. The total minimum is roughly one week, but adolescents often take longer.
A parallel return-to-learn protocol applies in the classroom: shortened school days, breaks between classes, reduced homework, extended deadlines, and a quiet space for testing — phased back to normal as tolerated.
Avoiding Second-Impact Syndrome
The most important rule of concussion management is "when in doubt, sit them out." A second concussion sustained while still recovering from the first can produce second-impact syndrome — rapid, often catastrophic brain swelling. It is rare but disproportionately strikes adolescents and is sometimes fatal. This single risk justifies the entire return-to-play framework.
Medications and Adjuncts
- Acetaminophen for headache (avoid NSAIDs in the first 24–48 hours per some protocols, due to theoretical bleeding risk)
- Anti-nausea medication short-term if needed
- Vestibular rehabilitation (specialized physical therapy) for persistent dizziness or balance problems
- Vision therapy for convergence insufficiency or oculomotor dysfunction
- Cervical physical therapy for whiplash-associated neck pain
Post-Concussion Syndrome and CTE Concerns
Post-Concussion Syndrome (PCS)
Most concussions resolve within 7–14 days in adults and 2–4 weeks in adolescents. When symptoms persist beyond 4 weeks, the condition is called persistent post-concussion symptoms (often still abbreviated PCS). Estimates vary, but roughly 10–30% of concussion patients develop persistent symptoms. The most common are headaches, fatigue, brain fog, sleep disturbance, anxiety, and depression.
Risk factors for PCS include female sex, prior concussions, prior migraines, prior anxiety or depression, adolescence, and a high initial symptom burden. The condition is real and biological — not "just psychological" — though psychological factors can amplify or maintain symptoms once the original injury has healed. Treatment is multidisciplinary: graded aerobic exercise (often guided by the Buffalo Concussion Treadmill Test), vestibular and vision therapy, cognitive behavioral therapy, sleep optimization, and targeted treatment of headaches.
Chronic Traumatic Encephalopathy (CTE)
Chronic traumatic encephalopathy is a progressive neurodegenerative disease linked to repetitive head impacts — not to a single concussion. It has been documented in football players, boxers, ice hockey players, soccer players, rugby players, military veterans exposed to blast injuries, and others with long histories of repeated head trauma. The hallmark pathological finding is the abnormal accumulation of tau protein in a distinctive perivascular pattern at the depths of cortical sulci — a signature distinct from Alzheimer's disease.
Symptoms typically emerge years to decades after exposure ends and include progressive memory loss, executive dysfunction, mood changes (depression, irritability, suicidality), impulsivity, and ultimately dementia. CTE can currently only be definitively diagnosed at autopsy, though clinical criteria called Traumatic Encephalopathy Syndrome (TES) are now used in living patients. Tau-PET imaging, blood biomarkers (phospho-tau, neurofilament light chain), and advanced MRI are active research targets.
Two important caveats: (1) the cumulative burden of subconcussive impacts — hits that don't cause symptoms but still stretch axons — appears to matter as much as or more than the number of diagnosed concussions, especially for athletes who started playing contact sports very young; and (2) not everyone with repetitive head trauma develops CTE, which suggests genetic susceptibility (such as APOE4 status) plays a role. Research is ongoing and rapidly evolving.
Prevention
You cannot prevent every concussion, but the rate is highly modifiable. The most effective interventions target the three biggest causes — falls, motor vehicle crashes, and contact sports.
Helmets and Protective Gear
Helmets reduce the risk of skull fractures and severe brain injury substantially, but it is important to be honest about their limits: no helmet fully prevents concussion, because concussion is driven by rotational forces inside the skull rather than direct skull impact. Helmets reduce concussion risk by perhaps 20–30% in cycling and skiing, less in football. Mouthguards, eye protection, and properly fitted equipment add incremental benefit.
Technique and Rule Changes
In sports, the largest gains come from technique training (e.g., heads-up tackling in football) and rule changes (banning checking from behind in hockey, prohibiting head-first tackles, limiting full-contact practice). USA Hockey's elimination of body checking at the youngest age levels cut concussion rates by roughly half. Soccer headers in young players are now restricted in many leagues.
Fall Prevention in Older Adults
Falls are the leading cause of TBI-related ED visits in adults over 65. The most effective fall-prevention measures are:
- Strength and balance training (tai chi, Otago Exercise Program)
- Vision correction — up-to-date glasses, cataract surgery
- Medication review — reducing sedatives, blood pressure drugs that cause orthostasis, anticholinergics
- Home modifications — remove throw rugs, install grab bars, improve lighting, eliminate clutter
- Vitamin D and adequate calcium for bone strength and muscle function
Motor Vehicle Safety
Seat belts, properly installed child car seats, airbags, anti-lock brakes, and rigorous policies against impaired and distracted driving prevent concussions before they happen. Modern vehicle safety design has cut TBI rates from crashes substantially.
Age-Appropriate Sports and Baseline Testing
Younger brains recover more slowly and may be more vulnerable to long-term effects of repetitive head impacts. Many pediatric organizations now recommend delaying tackle football and full-contact hockey to age 14 or older, and limiting heading in youth soccer. Baseline neurocognitive testing in athletes (preseason ImPACT or similar) gives clinicians a personal benchmark for return-to-play decisions and is now standard at most colleges and high schools that field contact-sport teams.
Research Papers
The following PubMed topic searches return current peer-reviewed literature relevant to this condition. Each link opens a live PubMed query.
- Concussion sport related
- Mild traumatic brain injury
- Diffuse axonal injury
- Post-concussion syndrome
- Chronic traumatic encephalopathy
- CTE tau pathology
- Second impact syndrome
- Return to play protocol
- SCAT5 sport concussion assessment
- Neurocognitive testing concussion
- Concussion biomarkers GFAP
- Vestibular rehabilitation concussion
Connections
- Neurology
- Traumatic Brain Injury (TBI)
- Migraine
- Alzheimer's Disease
- Parkinson's Disease
- Multiple Sclerosis
- Sleep Hygiene
- PTSD
- Anxiety
- Insomnia
- Magnesium
- Omega-3 Fatty Acids
- Methylene Blue
- Anti-Inflammatory Diet
- Depression
- Headache
- Fatigue
- Brain Fog
- Dizziness
- Epilepsy