Reversing Insulin Resistance: Diet and Fasting Protocols
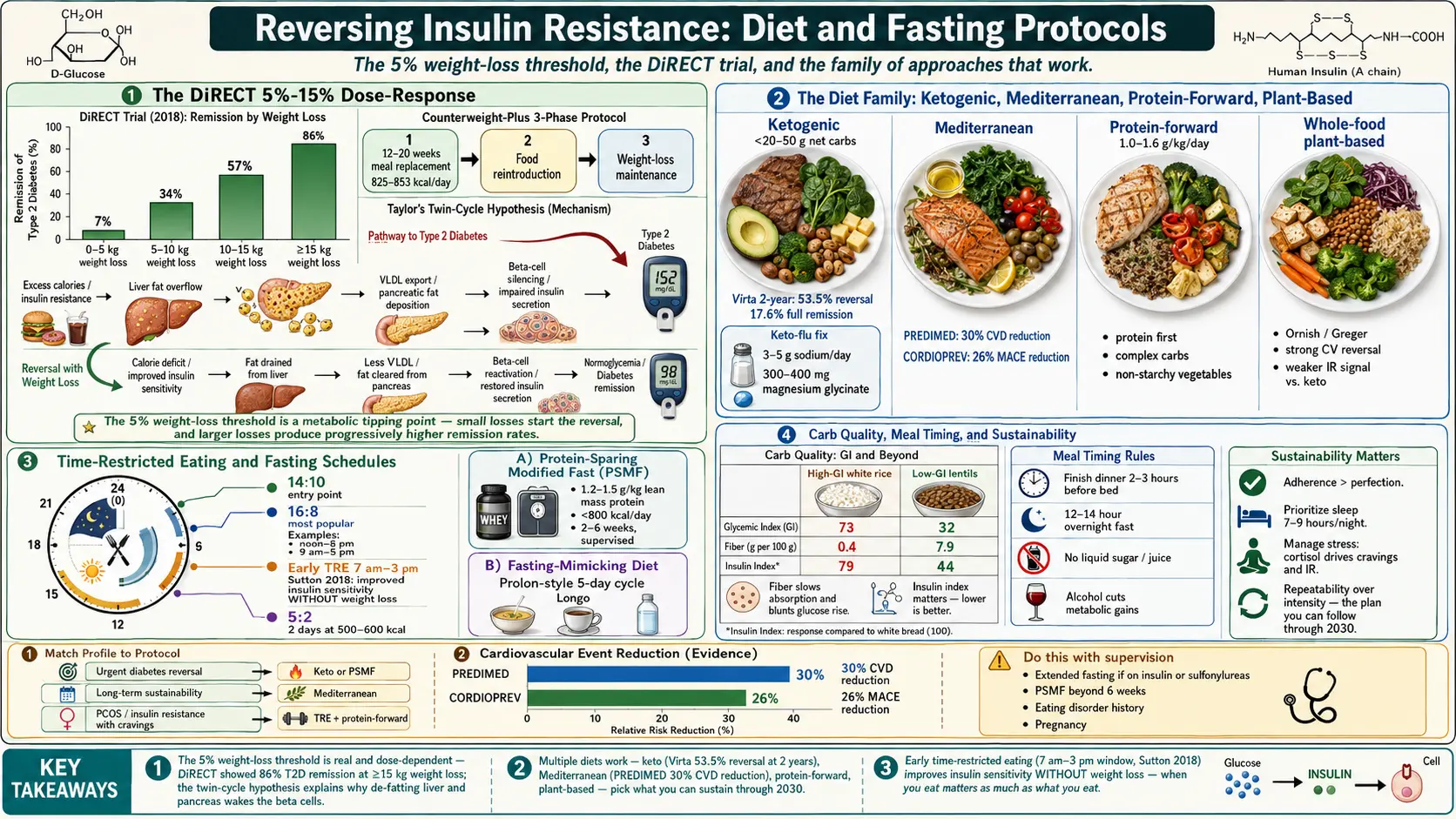
Table of Contents
- Why Food Comes First
- The 5% Weight-Loss Threshold — DiRECT and Newcastle
- Low-Carb and Ketogenic Diets
- The Mediterranean Diet
- Protein-Forward, Lower-Glycemic-Load Eating
- Low-Fat and Whole-Food Plant-Based
- Time-Restricted Eating and Intermittent Fasting
- The Protein-Sparing Modified Fast
- Extended Fasts and Fasting-Mimicking Diets
- Carbohydrate Quality Over Quantity
- Meal Timing, Sleep, and Alcohol
- How to Pick a Protocol You Will Actually Keep
- Cautions and Who Should Not Do This Alone
- Key Research Papers
- Connections
- Featured Videos
Why Food Comes First
Insulin resistance is, at its core, a problem of too much insulin circulating too often. Your muscles and liver stop responding to the hormone because they are flooded with it, day after day. The medications we have — metformin, berberine, GLP-1 agonists like semaglutide — help. But nothing lowers insulin as powerfully, as cheaply, or as durably as changing what and when you eat.
The encouraging news, and the point of this article, is that insulin resistance is one of the most reversible metabolic conditions in medicine. Not just managed. Reversed. We have high-quality randomized trials showing that the majority of people with type 2 diabetes can come off insulin and hit normal HbA1c — sometimes within weeks — using nothing but a structured eating plan. Prediabetes and the milder insulin resistance that shows up on a HOMA-IR score are even easier targets.
No single diet is "the" answer. Several work. What they share is a consistent reduction in the metabolic load your pancreas has to handle. Your job is to pick the version you can live with for the rest of your life.
The 5% Weight-Loss Threshold — DiRECT and Newcastle
If you remember one number from this page, make it 5%. That is the weight-loss threshold at which insulin resistance and type 2 diabetes begin to reverse in a meaningful way for most people who carry extra visceral fat.
The evidence comes primarily from the DiRECT trial (Diabetes Remission Clinical Trial), run across UK primary care clinics by Roy Taylor at Newcastle University and Mike Lean at Glasgow, published in The Lancet in 2018. DiRECT randomized 306 adults with type 2 diabetes (diagnosed within the last six years, not on insulin) to either standard care or a structured weight-management program called Counterweight-Plus. The intervention had three phases:
- Total diet replacement. Four meal-replacement shakes and soups per day, totaling 825–853 kcal, for 12 to 20 weeks. All other diabetes and antihypertensive drugs were stopped on day one under physician supervision.
- Structured food reintroduction. Two to eight weeks of stepped reintroduction of ordinary food, starting at around 1,500 kcal per day.
- Long-term weight maintenance with monthly primary-care check-ins.
The results redefined what primary care can do:
- 46% of the intervention group achieved diabetes remission at 12 months (HbA1c under 6.5% with no diabetes medications), versus 4% of controls.
- Remission was strongly dose-dependent on weight loss. Participants losing 0–5 kg had a 7% remission rate. Those losing 5–10 kg hit 34%. Those losing 10–15 kg hit 57%. And those losing 15 kg or more reached 86%.
- Framed as percent body weight, roughly 5% loss started producing remission, and 15% loss made it the most likely outcome (around 64%).
- At the two-year follow-up, 36% of the original intervention group remained in remission, compared to 3% of controls.
Taylor's twin-cycle hypothesis explains the mechanism. Excess calories pile up as fat in the liver, which oozes that fat into the pancreas, which strangles the insulin-producing beta cells. Take the fat out of the liver and pancreas — which happens quickly on a calorie-deficit diet — and the beta cells wake up. The 5% threshold is roughly the point at which the organs begin to de-fat.
You do not need to do Counterweight-Plus exactly. The how of losing 5–15% matters less than the whether. The diets below are all delivery vehicles for the same underlying trick: sustained energy deficit plus lower insulin exposure.
Low-Carb and Ketogenic Diets
Because carbohydrates are the single biggest drivers of post-meal insulin spikes, cutting them hard and fast is the most mechanically direct way to lower insulin. A ketogenic diet restricts net carbohydrates to under 20–50 grams per day, keeps protein moderate, and fills the rest of the plate with fats. After four to seven days, the liver switches to making ketones from fat, and blood glucose stabilizes in a narrow range.
The strongest insulin-resistance evidence comes from the Virta Health trial, a two-year open-label study led by Sarah Hallberg and published by Athinarayanan and colleagues in 2018. Virta used an individualized ketogenic intervention with continuous remote physician and coach support. At two years:
- 53.5% of the intervention group met criteria for type 2 diabetes reversal.
- 17.6% achieved full remission (normal HbA1c off all medications).
- Most participants came off sulfonylureas and reduced or eliminated insulin.
- HbA1c dropped by about 0.9 points; HOMA-IR dropped sharply in parallel.
Practical rules of thumb for a keto approach:
- Carbs: Under 20 g net for strict keto, under 50 g for "low-carb." Track for the first month; most people can freestyle after that.
- Protein: 1.2–1.6 g per kg of ideal body weight. Protein does raise insulin modestly but far less than carbs, and it protects muscle during weight loss.
- Fat: Fills the rest. Olive oil, avocado, nuts, fatty fish, eggs, full-fat dairy if tolerated.
- Ketone monitoring: Optional but motivating. A blood ketone meter reading 0.5–3.0 mmol/L confirms nutritional ketosis. Urine strips work in week one but become unreliable thereafter.
Keto flu is the headache, fatigue, and brain fog many people hit in days 2–5. It is sodium, potassium, and magnesium loss, not a sign you are doing it wrong. Mitigate with 3–5 g of sodium per day (broth, salt on food, electrolyte powders), 300–400 mg of magnesium glycinate at night, and normal potassium intake from avocado, leafy greens, and salmon.
Two honest caveats. First, a minority of people — particularly lean, athletic hyper-responders — see their LDL cholesterol rise steeply on keto. If your LDL jumps over 190 mg/dL or apoB over 120, swap some saturated fat for olive oil and nuts, and discuss with your doctor. Second, keto is chemically effective but socially and culinarily narrow. Long-term adherence rates at five years are mediocre. If you cannot see yourself eating this way in 2030, use keto as a tool for a 3–12 month reversal phase, then transition to a Mediterranean or protein-forward pattern for maintenance.
The Mediterranean Diet
If keto is a scalpel, the Mediterranean diet is a steady hand. It is the only eating pattern with decades of randomized-trial data on cardiovascular and metabolic endpoints, and it wins on long-term adherence almost every time it is tested.
The PREDIMED trial (Estruch et al., NEJM 2013, reanalyzed 2018) randomized 7,447 high-cardiovascular-risk Spanish adults to either a Mediterranean diet supplemented with extra-virgin olive oil, the same diet supplemented with mixed nuts, or a low-fat control. The two Mediterranean arms cut major cardiovascular events by about 30% over five years. Subsequent substudies showed significant drops in fasting insulin, HOMA-IR, and progression to type 2 diabetes.
The CORDIOPREV study (Delgado-Lista et al., 2022) compared the Mediterranean diet head-to-head with a low-fat diet in 1,002 coronary-heart-disease patients over seven years. Mediterranean produced a 26% reduction in major adverse cardiac events and better long-term insulin sensitivity.
What the actual plate looks like:
- Extra-virgin olive oil as the primary fat (4+ tablespoons per day).
- Vegetables at every meal, fruit daily (lower-glycemic — berries, apples, citrus — if IR is active).
- Legumes several times per week.
- Fish 3+ times per week, especially oily fish (sardines, salmon, anchovies).
- Poultry and eggs in moderation; red meat rarely.
- Nuts daily (a handful).
- Whole grains in portions appropriate to your insulin status — start lower if HOMA-IR is high.
- Red wine only if you already drink, with meals, and modestly. Not required.
Mediterranean does not produce the sharp drops in fasting insulin that keto delivers in eight weeks. It produces durable drops over years, with strong cardiovascular protection baked in. For most patients with mild to moderate insulin resistance and no urgent diabetes to reverse, this is the pattern to start with and stay on.
Protein-Forward, Lower-Glycemic-Load Eating
A middle path for people who do not want to count carbs strictly but want better metabolic results than a standard Western diet offers. The formula:
- Protein first at every meal. Target 1.0–1.6 g per kg of body weight per day, distributed across 3–4 meals. 30–40 g at breakfast changes the rest of the day.
- Non-starchy vegetables. Half the plate, most meals.
- Complex carbohydrates — lentils, beans, intact whole grains, berries, root vegetables — as the carb portion, instead of bread, rice, and flour-based foods.
- Healthy fats — olive oil, nuts, avocado, fatty fish — to round out meals and drive satiety.
This approach leans on protein's two advantages for insulin resistance. First, protein is the most satiating macronutrient, which quietly cuts total calorie intake without conscious restriction. Second, adequate protein during any weight-loss phase protects skeletal muscle, and muscle is the largest glucose disposal organ in your body. Losing weight while losing muscle makes your insulin resistance worse, not better. Keeping protein high keeps muscle on.
Low-Fat and Whole-Food Plant-Based
The opposite end of the macronutrient map. Approaches like Dean Ornish's reversal program and the whole-food plant-based approach popularized by Michael Greger restrict fat to 10–15% of calories, eliminate animal products, and rely on legumes, whole grains, fruit, and vegetables.
The evidence is a mixed bag for IR specifically. Ornish's program has the best cardiovascular-reversal data (Lifestyle Heart Trial, 1990) of any diet ever tested, with documented regression of coronary plaques. On fasting insulin and HOMA-IR, plant-based diets perform well, but the signal is weaker than for keto or DiRECT-style caloric restriction in head-to-head studies. Where whole-food plant-based shines is cardiovascular risk reduction, gut microbiome diversity, and sustainability for people who dislike meat.
If you choose this route, pay attention to:
- Protein adequacy — legumes, tofu, tempeh, seitan. Aim for the same 1.0–1.4 g/kg target.
- B12 supplementation — mandatory on any vegan plan.
- Omega-3 from algae oil if no fish.
- Refined carbohydrate traps. "Plant-based" pasta, bread, and dessert are still high-glycemic. IR reversal on plant-based requires whole foods, not just meatless foods.
Time-Restricted Eating and Intermittent Fasting
Time-restricted eating (TRE) narrows your daily food intake to a window — typically 8, 10, or 12 hours — and leaves the rest of the 24 as water, black coffee, or plain tea. No counting, no forbidden foods, just a clock.
The mechanistic breakthrough study is Sutton et al., Cell Metabolism 2018. Eight men with prediabetes were randomized to early time-restricted feeding (eating between roughly 7 a.m. and 3 p.m.) versus a 12-hour schedule, with calorie intake matched. After five weeks, the early-TRE arm had substantially improved insulin sensitivity, lower fasting insulin, lower blood pressure, and reduced oxidative stress — without any weight change. This trial is the cleanest demonstration that when you eat affects insulin signaling independent of how much.
Practical TRE schedules:
- 14:10 — 10-hour eating window. The easiest entry point; most people do this naturally by skipping bedtime snacks.
- 16:8 — 8-hour window. The most popular format. Typical: eat noon to 8 p.m., or better, 9 a.m. to 5 p.m.
- Early vs late window. Finishing dinner by 6–7 p.m. outperforms a late window in head-to-head data. Your circadian insulin sensitivity is higher in the morning.
- OMAD (one meal a day) — popular online but no evidence it beats 16:8 on insulin metrics, and harder to hit protein targets.
- 5:2 — five normal days, two days at 500–600 kcal. Works for some. Equivalent results to standard caloric restriction in most randomized comparisons.
TRE pairs naturally with any of the food-quality approaches above. It is the single easiest behavioral intervention to add.
The Protein-Sparing Modified Fast
The PSMF is an aggressive short-term tool, not a lifestyle. The format:
- Protein: 1.2–1.5 g per kg of lean body mass, from lean meat, fish, poultry, egg whites, or low-fat dairy.
- Fat: minimal (incidental to the protein source).
- Carbs: minimal, usually only from non-starchy vegetables.
- Total calories: typically under 800.
- Duration: two to six weeks, with multivitamin, sodium, potassium, and magnesium supplementation, and — for longer runs — physician supervision.
Lyle McDonald documented the protocol in book form in the 1990s; Benjamin Bikman and others have updated it for modern metabolic-health use. It is effectively a medically-supervised very-low-calorie diet that spares muscle via high protein. Expect 1–2 kg of fat loss per week and rapid drops in fasting insulin and liver fat.
PSMF is not for everyone. It is intense, flavorless by design, and must not be done for more than six weeks without medical oversight. Use it to break through a plateau or initiate a reversal phase, then transition to a sustainable pattern.
Extended Fasts and Fasting-Mimicking Diets
Beyond daily TRE lie extended water fasts — 24 to 72 hours of water, black coffee, tea, and electrolytes only. Done under medical supervision, they produce deep autophagy, rapid liver-fat clearance, and sharp insulin drops. Risks include refeeding syndrome (especially after 72+ hours), electrolyte disturbance, and hypoglycemia in people on sulfonylureas or insulin. Do not attempt extended fasts if you are underweight, pregnant, on diabetes medication, or have a history of disordered eating.
A gentler alternative is the fasting-mimicking diet (FMD), developed by Valter Longo at USC and sold commercially as Prolon. FMD is a five-day cycle of plant-based, low-protein, low-calorie meal kits (roughly 1,100 kcal on day 1 and 800 kcal on days 2–5) that produces most of the metabolic signatures of water fasting while still letting you eat. Small trials show improvements in fasting glucose, insulin, IGF-1, and markers of biological aging when repeated monthly for three cycles. FMD is expensive but forgiving. Many clinicians use it as a quarterly reset in patients who are otherwise eating a Mediterranean pattern.
Carbohydrate Quality Over Quantity
Not all carbs behave the same in your blood. Fifty grams of lentils and fifty grams of white-bread carbohydrate produce very different glucose and insulin curves, even though they are the same quantity. The quality dimensions that matter:
- Glycemic index (GI) — how fast 50 g of the carb raises blood glucose. White rice is 73; lentils are 32.
- Glycemic load (GL) — GI scaled to a realistic portion. A better real-world number.
- Insulin index — the insulin response specifically. Some foods (dairy, some protein-carb mixes) provoke more insulin than their glucose curve predicts.
- Fiber content. Soluble fiber slows carbohydrate absorption and feeds beneficial gut bacteria that produce butyrate, which improves insulin signaling.
The practical rule: build meals around carbs that come packaged with fiber, water, and a little protein or fat. Berries instead of juice. Whole intact oats instead of instant. Lentils and beans instead of refined flour. Sweet potato instead of potato chips. Even if your net carb count stays the same, your insulin exposure drops.
Meal Timing, Sleep, and Alcohol
Front-load your calories. Jakubowicz et al., Diabetes Care 2020, randomized women with obesity and type 2 diabetes to a high-energy breakfast, moderate lunch, and small dinner (B-diet) versus six small meals spread through the day (6M-diet), with matched calories. After twelve weeks, the B-diet group lost more weight, saw greater drops in glucose and HbA1c, and reduced their total daily insulin dose by an average of 26 units. The meta-message: human metabolism handles carbohydrates better in the morning than at night.
In practical terms: eat dinner before 7 p.m. when you can, and make it the smallest meal of the day rather than the biggest. This also pairs with early-window time-restricted eating.
Sleep is sugar. Eve Van Cauter and Karine Spiegel's classic sleep-restriction studies in young healthy men showed that four days of 4-hour sleep reduced insulin sensitivity by roughly 30% — the metabolic profile of someone decades older. You can ruin a perfect diet with chronic poor sleep. Seven to nine hours is not a luxury; it is part of the protocol.
Alcohol. Ethanol is processed by the liver ahead of anything else. While alcohol is in the bloodstream, fat metabolism pauses and de-novo lipogenesis rises. Heavy or daily drinking drives fatty liver, which drives insulin resistance, which drives more fatty liver. If you are trying to reverse IR or NAFLD, reduce alcohol to a few drinks per week or eliminate it for the reversal phase.
How to Pick a Protocol You Will Actually Keep
Here is the honest summary no diet book will tell you: the best diet for insulin resistance is the one you will still be doing in three years. The trials are full of crossover and dropout. The winners, statistically, are the people who found a pattern they could live with.
Some matchmaking:
- Urgent diabetes with HbA1c over 8, on multiple drugs? Consider a DiRECT-style 12-week total diet replacement or a medically supervised ketogenic reset. Call in your doctor before starting; medication adjustments are mandatory on day one.
- Clear diagnosis of type 2 diabetes, motivated, food-focused? Virta-style ketogenic for 6–12 months, then transition to Mediterranean or protein-forward for maintenance.
- Prediabetes or HOMA-IR of 2.5–4.5, no urgent emergency? Mediterranean or protein-forward plus 14:10 or 16:8 time-restricted eating. Retest in 3 and 6 months.
- PCOS with IR? Lower-carb Mediterranean, protein-forward, or moderate keto all have good data. See IR and PCOS.
- NAFLD/MASLD as the driver? Any approach that produces 5–10% weight loss works; Mediterranean has the most liver-specific data. See the NAFLD/MASLD article.
- Plateau or need a reset? A 2–4 week PSMF or a single cycle of fasting-mimicking diet.
Measure to believe. Check fasting insulin and HOMA-IR at baseline, 3 months, and 6 months. HbA1c and fasting glucose are slower to move and can miss improvements. Triglycerides, HDL, and the triglyceride-to-HDL ratio are cheap surrogates that often track HOMA-IR well. See the fasting insulin and HOMA-IR testing guide.
Cautions and Who Should Not Do This Alone
Most of the tools on this page are safe for motivated adults with standard insulin resistance or mild type 2 diabetes. A few groups need extra caution or explicit medical supervision:
- Type 1 diabetes. Keto, TRE, and fasting can be used with T1D, but only under the close care of an endocrinologist who understands both the diet and insulin dosing. Sliding-scale insulin must be adjusted or dangerous hypoglycemia will follow. This is not a DIY project.
- T2D on insulin or sulfonylureas. Any reduction in carb intake or introduction of fasting requires medication adjustment on day one. Hypoglycemia from unadjusted glipizide is the most common preventable harm in this space.
- Pregnancy or breastfeeding. Do not do extended fasting or strict ketogenic diets during pregnancy. A Mediterranean or lower-glycemic pattern is appropriate; consult your obstetrician for gestational diabetes management.
- History of eating disorders. Rigid food rules, prolonged fasting, and intense counting are contraindicated. Work with a therapist or dietitian experienced in eating-disorder recovery. A gentle Mediterranean pattern is usually the safe floor.
- Elderly adults with sarcopenia. Aggressive caloric restriction can cost irreplaceable muscle. Protein-forward approaches with resistance training are the priority; PSMFs and extended fasts are usually wrong at this age.
- Low body weight or underweight. You cannot — and should not try to — reverse IR through further weight loss. Look instead at muscle-building resistance training, sleep, and reducing refined-carb exposure. See exercise and muscle insulin sensitivity.
- Chronic kidney disease stage 3 or beyond. The 1.6 g/kg protein target may be too high. Work with a renal dietitian.
If you are on any diabetes or blood-pressure medication, have a conversation with your prescriber before you change your diet, not after. Dietary reversal is powerful enough to require the same dose changes as starting a new drug.
Key Research Papers
Foundational publications demonstrating that type 2 diabetes is reversible — from the DiRECT trial's primary-care weight-loss remission, to the Virta ketogenic 2-year results, to the time-restricted-eating and meal-timing studies that work without calorie restriction. Each citation links to the full text via DOI.
- Lean MEJ, Leslie WS, Barnes AC, et al. Primary Care-Led Weight Management for Remission of Type 2 Diabetes (DiRECT): An Open-Label, Cluster-Randomised Trial. Lancet. 2018;391(10120):541–551.
- Lean MEJ, Leslie WS, Barnes AC, et al. Durability of a Primary Care-Led Weight-Management Intervention for Remission of Type 2 Diabetes: 2-Year Results of the DiRECT Open-Label, Cluster-Randomised Trial. Lancet Diabetes & Endocrinology. 2019;7(5):344–355.
- Hallberg SJ, McKenzie AL, Williams PT, et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. Diabetes Therapy. 2018;9(2):583–612.
- Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes: A 2-Year Non-Randomized Clinical Trial. Frontiers in Endocrinology. 2019;10:348.
- Sutton EF, Beyl R, Early KS, Cefalu WT, Ravussin E, Peterson CM. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even Without Weight Loss in Men with Prediabetes. Cell Metabolism. 2018;27(6):1212–1221.
- Jakubowicz D, Landau Z, Tsameret S, et al. Reduction in Glycated Hemoglobin and Daily Insulin Dose Alongside Circadian Clock Upregulation in Patients with Type 2 Diabetes Consuming a Three-Meal Diet: A Randomized Clinical Trial. Diabetes Care. 2019;42(12):2171–2180.
- de Cabo R, Mattson MP. Effects of Intermittent Fasting on Health, Aging, and Disease. New England Journal of Medicine. 2019;381(26):2541–2551.
- Volek JS, Phinney SD, Forsythe CE, et al. Carbohydrate Restriction Has a More Favorable Impact on the Metabolic Syndrome Than a Low Fat Diet. Lipids. 2009;44(4):297–309.
- Estéruelas-Cabrera M, Salas-Salvadó J, Babio N, et al. Mediterranean Diet and Type 2 Diabetes Incidence: The PREDIMED Trial. Annals of Internal Medicine. 2014;160(1):1–10.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin (Diabetes Prevention Program). New England Journal of Medicine. 2002;346(6):393–403.
- Reaven GM. Banting Lecture 1988. Role of Insulin Resistance in Human Disease. Diabetes. 1988;37(12):1595–1607.
- Petersen MC, Shulman GI. Mechanisms of Insulin Action and Insulin Resistance. Physiological Reviews. 2018;98(4):2133–2223.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: DiRECT trial and remission
- PubMed: ketogenic diet and T2D
- PubMed: Mediterranean diet and HOMA-IR
- PubMed: time-restricted eating and IR
- PubMed: fasting-mimicking diet (Longo)
- PubMed: protein-sparing modified fast
- PubMed: glycemic load and IR
- PubMed: sleep deprivation and IR
- PubMed: PREDIMED and diabetes
- PubMed: Virta Health 2-year ketogenic
Connections
- Blood Sugar & Insulin — interactive animation
- Fasting Insulin and HOMA-IR Testing
- Exercise and Muscle Insulin Sensitivity
- NAFLD & MASLD Connection
- Insulin Resistance and PCOS
- Insulin Resistance
- Diabetes
- Obesity
- CGM for Non-Diabetics
- Metformin, Berberine and GLP-1s
- Metabolic Syndrome Cardiovascular Risk
- Elimination Diet
- Fasting
- Fasting Insulin
- Magnesium
- Olive Oil
- Lentils
- Metabolic Syndrome
- Visceral Fat
- Blood Sugar Deep Dive: Insulin Resistance — the Reaven Syndrome X framework, HOMA-IR ranges, and the ectopic-lipid mechanism these diet and fasting protocols are working against.