Exercise and Muscle Insulin Sensitivity
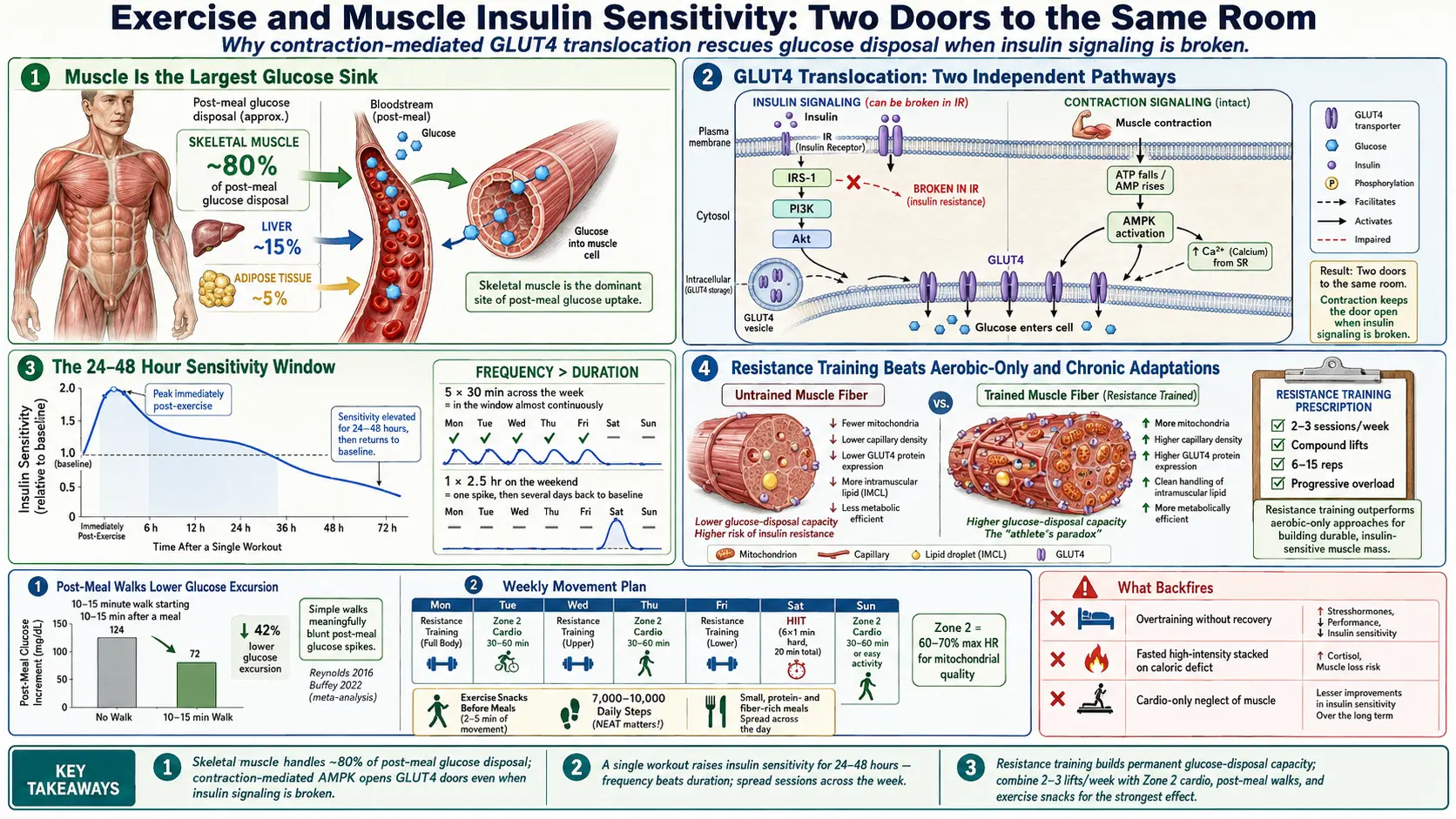
Table of Contents
- Why Muscle Is the Center of the Story
- GLUT4 Translocation — Two Doors to the Same Room
- The 24–48 Hour Window After a Single Workout
- Chronic Training Adaptations
- Resistance Training Beats Aerobic-Only for IR
- Post-Meal Walks — The Cheapest Intervention in Medicine
- Zone 2 Aerobic Work
- HIIT — Potent and Time-Efficient
- Exercise Snacks, NEAT, and the Sitting Problem
- Timing Relative to Meals
- What Doesn't Work — And What Backfires
- Special Populations
- A 12-Week Starter Plan by Fitness Level
- Key Research Papers
- Connections
- Featured Videos
Why Muscle Is the Center of the Story
If you want to understand why exercise is so powerful for insulin resistance, start with one number: roughly 80% of the glucose that enters your bloodstream after a meal is pulled out of circulation by skeletal muscle. Liver and fat tissue handle the rest. Muscle is, by a wide margin, the largest glucose sink in the human body.
That single fact reframes insulin resistance. It is not primarily a pancreas problem or a willpower problem — it is, in large part, a muscle problem. When the doorways that let glucose into muscle cells start to rust shut, blood sugar lingers in circulation, the pancreas compensates with more insulin, and the whole metabolic system tilts toward trouble. More muscle, and more insulin-sensitive muscle, means more glucose disposal capacity. Less muscle, or more insulin-resistant muscle, means less.
This is why you can often out-exercise a bad meal in a way you cannot out-exercise a bad diet in the long run: a single session of exercise directly opens a second pathway for glucose to enter muscle — one that does not need insulin at all.
GLUT4 Translocation — Two Doors to the Same Room
Glucose cannot diffuse into muscle cells on its own. It needs a transporter protein called GLUT4 to carry it across the cell membrane. In a resting muscle cell, most GLUT4 sits idle inside tiny storage vesicles in the cytoplasm. For glucose to get in, those vesicles have to travel to the cell surface and fuse with the membrane, planting GLUT4 like a doorway. That process is called GLUT4 translocation.
There are two independent ways to trigger it:
- Insulin-dependent pathway (resting state). After you eat, insulin binds its receptor on the muscle cell, kicks off a signaling cascade (IRS-1, PI3K, Akt), and GLUT4 vesicles move to the membrane. This is the pathway that breaks in insulin resistance — the receptor signals weakly, fewer GLUT4 doors open, and glucose piles up outside the cell.
- Contraction-mediated pathway (exercise). When a muscle contracts, it burns ATP. Falling ATP and rising AMP activate an energy sensor called AMPK (AMP-activated protein kinase). AMPK triggers GLUT4 translocation by an entirely separate route that does not require insulin. Calcium release during contraction also contributes.
This is the single most important sentence on this page: contraction opens GLUT4 doors even when insulin cannot. In a person whose insulin signaling is broken, walking, lifting, or cycling still drops blood glucose because the muscle is prying its own doors open with a second key. That is why a diabetic person who cannot get blood sugar under control with medication alone will often see glucose fall 30–60 mg/dL after a brisk 15-minute walk.
The two pathways are additive. After exercise, the insulin-dependent door also works better for many hours. You get a temporary repair of the broken pathway layered on top of a second pathway that was never broken.
The 24–48 Hour Window After a Single Workout
A single bout of moderate or vigorous exercise increases muscle insulin sensitivity for roughly 24 to 48 hours. During that window, a given amount of insulin moves more glucose than it did before the workout. HOMA-IR scores drop. Post-meal glucose spikes are smaller. Fasting insulin the next morning is lower.
The practical implication is enormous: frequency matters more than duration. Five 30-minute sessions spread across the week keep you inside that sensitivity window almost continuously. One 2.5-hour session on Saturday leaves you outside the window from roughly Monday onward. Spread the dose.
This is also why "weekend warrior" cardio produces weaker metabolic results than daily activity, even at identical weekly minutes. The muscle forgets.
Chronic Training Adaptations
Stay with regular training for weeks and months, and deeper changes stack on top of the acute effect:
- Increased mitochondrial density. Muscle cells grow more mitochondria and enlarge the ones they have. More mitochondria means more capacity to burn fat and glucose, and less overflow into lipid droplets that disrupt insulin signaling.
- Capillarization. New capillaries grow into trained muscle. More capillaries means more surface area for insulin and glucose to reach muscle cells in the first place — a delivery problem solved at the plumbing level.
- Higher baseline GLUT4 protein expression. Trained muscle simply has more GLUT4 transporters stored and ready to translocate. The doors are more numerous before a single one opens.
- Improved intramuscular lipid handling. Endurance-trained muscle paradoxically stores more intramuscular triglyceride (the "athlete's paradox") yet remains insulin sensitive, because those lipids are cleanly packaged and actively burned rather than leaking toxic intermediates like diacylglycerol and ceramide that jam insulin signaling.
Resistance Training Beats Aerobic-Only for IR
For decades, "exercise for diabetes" meant walking. The research has caught up: in sedentary and insulin-resistant people, resistance training produces larger insulin-sensitivity gains than equivalent time spent doing aerobic work alone. The argument is structural. Every pound of skeletal muscle you add is a permanent increase in glucose disposal capacity. That capacity sits on your frame twenty-four hours a day, whether you exercise that day or not.
The practical prescription is modest and achievable:
- 2–3 sessions per week, non-consecutive days.
- Compound lifts that recruit large muscle groups — squat, deadlift (or hip hinge), chest press, row, overhead press, loaded carry. Machines are fine for beginners.
- Progressive overload — add weight, reps, or sets over time. The stimulus has to keep increasing or adaptation stops.
- Rep range 6–15 for hypertrophy plus strength. You do not need to train like a powerlifter to build metabolic muscle.
The combined approach — resistance training plus aerobic work — beats either one alone. But if you only have time for one, and you are sedentary and insulin-resistant, resistance training is the higher-yield investment.
Post-Meal Walks — The Cheapest Intervention in Medicine
A 10–15 minute walk immediately after a meal flattens the post-meal glucose spike by a clinically meaningful amount. Reynolds and colleagues showed in 2016 that post-meal walks lowered post-prandial glucose more than a single longer daily walk. The 2022 meta-analysis by Buffey and colleagues pooled seven trials and confirmed that even 2–5 minute "light-intensity" walking breaks after eating significantly reduced post-meal glucose compared with prolonged sitting.
The mechanism is exactly what you would predict. Food is pouring glucose into your bloodstream. Contracting leg muscles open AMPK-driven GLUT4 doors. Glucose goes into the muscle instead of marinating the rest of your organs. The effect is largest after the carb-heaviest meal of the day — typically dinner.
Practical rules:
- Walk within 15 minutes of finishing a meal, not an hour later.
- Any pace beats sitting. Brisk beats strolling, but strolling beats the couch by a wide margin.
- 10–15 minutes is the sweet spot. Longer is better but not required.
- If walking outside is not an option, pace the house, walk a hallway, or march in place while watching TV.
This single habit, done after the two largest meals of the day, can shift an early-stage insulin-resistant person's CGM trace noticeably within a week.
Zone 2 Aerobic Work
Zone 2 is the intensity at which you are breathing harder than at rest but can still hold a conversation in full sentences. In heart-rate terms it is roughly 60–70% of your maximum heart rate. Physiologically it is the highest intensity at which fat remains the dominant fuel and lactate stays low.
Zone 2 is the best tool in exercise physiology for building mitochondrial quality — the cellular machinery that ultimately determines how cleanly your muscle handles fat and glucose. Healthy, dense mitochondria burn fatty acids all the way to CO2 and water. Damaged or sparse mitochondria stall halfway, accumulate toxic lipid intermediates, and jam insulin signaling from the inside.
The target dose is 150+ minutes per week, aligning with the American Diabetes Association and WHO physical-activity guidelines. Split it however fits your life — three 50-minute sessions, five 30-minute sessions, or daily 20-minute bike commutes. Walking briskly uphill, easy cycling, swimming, rowing, and elliptical all qualify.
HIIT — Potent and Time-Efficient
High-intensity interval training alternates short hard efforts (30 seconds to 4 minutes) with recovery periods. Well-designed HIIT produces insulin-sensitivity improvements comparable to or greater than longer moderate-intensity sessions, in a fraction of the total time — often just 3 sessions per week of 10–20 minutes each.
A simple starter HIIT session on a bike or rower:
- 5 minutes easy warm-up.
- 6 rounds: 1 minute hard (RPE 8–9 out of 10), 1 minute easy.
- 3 minutes easy cool-down.
Total time: 20 minutes. Total hard work: 6 minutes. Metabolic effect: large.
The caveat: HIIT alone does not build the muscle mass you need for long-term glucose disposal. It gives you cardiovascular benefits and acute insulin-sensitivity gains, but it does not replace resistance training. The strongest protocol combines HIIT, Zone 2, and resistance work across a week.
Exercise Snacks, NEAT, and the Sitting Problem
Structured workouts are only part of the story. The research on sedentary behavior is unambiguous: prolonged sitting impairs insulin sensitivity even in people who exercise regularly. Healy and colleagues showed in 2008 that independent of total moderate-to-vigorous activity, time spent sedentary was associated with worse metabolic markers. You can run for an hour at 6 a.m. and still have a metabolically compromised day if you sit motionless from 9 to 5.
The counter-moves are small and frequent:
- Exercise snacks. One minute of stair climbing or bodyweight squats 3 times a day. Francois and colleagues (2014) showed that brief intense exercise "snacks" before meals improved 24-hour glucose control.
- Break up sitting. Stand, walk, or stretch for 2–5 minutes every 30–60 minutes.
- Standing desk. Not a cardiovascular intervention, but it raises NEAT (non-exercise activity thermogenesis) and reduces uninterrupted sitting.
- Daily step target. Roughly 7,000–10,000 steps. The benefit curve is steepest between 4,000 and 8,000; past 10,000 the returns flatten.
NEAT — all the movement that is not formal exercise — can differ by 1,500–2,000 calories per day between two people of the same size. That gap is larger than almost any workout prescription. Cultivate restlessness.
Timing Relative to Meals
Three patterns work; which one fits depends on your life and your stomach:
- Post-meal walk (10–15 min). Best for blunting glucose excursions. Use after the largest meal.
- Pre-meal exercise snack (1–6 min vigorous). Primes GLUT4 so the meal lands on an already-opened door. Effective and time-efficient.
- Fasted morning session. A moderate workout before breakfast uses fat as fuel and depletes muscle glycogen, increasing sensitivity to the first post-workout meal. Works well for Zone 2 and light resistance work.
What to avoid: fasted, high-intensity, long-duration training done regularly — especially when stacked onto aggressive caloric restriction. That combination can spike cortisol, raise morning fasting glucose via gluconeogenesis, and in the long run worsen the picture rather than improve it. If you want to fast and train hard, keep one of the two variables dialed down.
What Doesn't Work — And What Backfires
- Spot reduction. Crunches, planks, and ab wheels do not preferentially burn visceral fat. Visceral fat responds to overall caloric deficit, insulin-lowering nutrition, and full-body resistance plus aerobic training. The belly is not a muscle you can target for fat loss.
- Overtraining without recovery. More is not always better. Chronically under-recovered lifters and runners can show worse insulin sensitivity, elevated cortisol, poor sleep, and rising fasting glucose. Program deload weeks every 4–8 weeks. Sleep is a training variable.
- Cardio-only in a sedentary, aging adult. Hours of elliptical without any resistance work neglects the muscle-building half of the equation. You stay aerobically fit and metabolically mediocre.
- Starvation plus hard training. Aggressive caloric deficits combined with high-volume training drive cortisol up, sex hormones down, and often plateau weight loss while worsening mood and sleep. Eat enough protein and carbohydrate to support the work.
Special Populations
Polycystic Ovary Syndrome (PCOS)
Insulin resistance is central to PCOS, and resistance training is particularly valuable here: it improves insulin sensitivity and favorably shifts the androgen-to-estrogen balance many women with PCOS struggle with. Two to three sessions per week of compound lifts, combined with post-meal walks and at least 150 minutes of Zone 2, is a powerful baseline. See IR and PCOS for the full protocol.
Post-Menopausal Women
Estrogen loss accelerates muscle mass decline and reduces insulin sensitivity. Protecting muscle becomes a medical priority, not a cosmetic one. Resistance training at meaningful loads — not just pink dumbbells — is the single best intervention for preserving bone density, muscle mass, and glucose control simultaneously. See Osteoporosis for the bone-loading side of the same prescription.
Sarcopenic Obesity in Older Adults
"Skinny fat" at 70 is common and dangerous: low muscle mass, high fat mass, poor insulin sensitivity, high fall risk. The treatment is protein-forward nutrition (roughly 1.2–1.6 g/kg body weight per day, distributed across meals) plus progressive resistance training. Frailty is not inevitable with age; it is mostly a training status.
Pregnancy
Pregnancy-safe options include walking, stationary cycling, swimming, prenatal yoga, and light-to-moderate resistance training with modified positions (no supine lifts after the first trimester). High-intensity intervals and heavy lifting should be scaled or paused after the first trimester unless supervised. Gestational diabetes prevention is a legitimate goal for insulin-resistant women entering pregnancy — discuss exercise dose with your obstetrician.
Arthritis and Joint Limitations
Aquatic exercise, recumbent cycling, elliptical, and rowing deliver meaningful insulin-sensitivity benefits without pounding the joints. Resistance training adapted to tolerated ranges of motion still builds muscle and still moves glucose. Pain is a reason to modify, not to quit.
A 12-Week Starter Plan by Fitness Level
Deconditioned (currently mostly sedentary)
- Weeks 1–4: 10-minute walk after dinner daily. Two sessions per week of 20 minutes of bodyweight resistance (sit-to-stand, wall push-up, assisted row, glute bridge). Build to 5,000 steps per day.
- Weeks 5–8: Add a 10-minute walk after lunch. Resistance sessions move to dumbbells or machines; 30 minutes, 2×/week. Steps to 7,000.
- Weeks 9–12: Add one 20-minute Zone 2 cardio session. Resistance to 3×/week. Steps to 8,000–10,000.
Moderately Active
- Weeks 1–4: 2×/week resistance (compound lifts, 4 exercises, 3 sets of 8–12). 2×/week Zone 2 cardio, 30 minutes. Post-dinner walks daily.
- Weeks 5–8: Add a third resistance session. Replace one Zone 2 with a 20-minute HIIT session (6×1-minute hard).
- Weeks 9–12: Progressive overload — add weight every 1–2 weeks. Add an exercise snack (1 minute of squats or stairs) before each meal.
Experienced
- Maintain 3–4 resistance sessions, 2 Zone 2 sessions of 45–60 minutes, 1 HIIT session per week.
- Deload every 6–8 weeks.
- Keep post-meal walks and exercise snacks regardless of training volume — they are additive, not redundant.
Retest fasting insulin and HOMA-IR at week 12. If you wear a CGM, expect narrower glucose excursions and a lower overnight baseline within the first 2–4 weeks.
Key Research Papers
Foundational publications on exercise physiology, GLUT4 translocation, and the dose-response relationship between physical activity and insulin sensitivity. Each citation links to the full text via DOI.
- Richter EA, Hargreaves M. Exercise, GLUT4, and Skeletal Muscle Glucose Uptake. Physiological Reviews. 2013;93(3):993–1017.
- Colberg SR, Sigal RJ, Yardley JE, et al. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care. 2016;39(11):2065–2079.
- Buffey AJ, Herring MP, Langley CK, Donnelly AE, Carson BP. The Acute Effects of Interrupting Prolonged Sitting Time in Adults with Standing and Light-Intensity Walking on Biomarkers of Cardiometabolic Health: A Systematic Review and Meta-Analysis. Sports Medicine. 2022;52(8):1765–1787.
- Healy GN, Dunstan DW, Salmon J, et al. Breaks in Sedentary Time: Beneficial Associations with Metabolic Risk. Diabetes Care. 2008;31(4):661–666.
- Holloszy JO. Exercise-Induced Increase in Muscle Insulin Sensitivity. Journal of Applied Physiology. 2005;99(1):338–343.
- DeFronzo RA, Jacot E, Jequier E, Maeder E, Wahren J, Felber JP. The Effect of Insulin on the Disposal of Intravenous Glucose: Results from Indirect Calorimetry and Hepatic and Femoral Venous Catheterization. Diabetes. 1981;30(12):1000–1007.
- Boulé NG, Haddad E, Kenny GP, Wells GA, Sigal RJ. Effects of Exercise on Glycemic Control and Body Mass in Type 2 Diabetes Mellitus: A Meta-Analysis of Controlled Clinical Trials. JAMA. 2001;286(10):1218–1227.
- Roberts CK, Hevener AL, Barnard RJ. Metabolic Syndrome and Insulin Resistance: Underlying Causes and Modification by Exercise Training. Comprehensive Physiology. 2013;3(1):1–58.
- Reaven GM. Banting Lecture 1988. Role of Insulin Resistance in Human Disease. Diabetes. 1988;37(12):1595–1607.
- Petersen MC, Shulman GI. Mechanisms of Insulin Action and Insulin Resistance. Physiological Reviews. 2018;98(4):2133–2223.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin (Diabetes Prevention Program). New England Journal of Medicine. 2002;346(6):393–403.
- Reynolds AN, Mann JI, Williams S, Venn BJ. Advice to Walk After Meals Is More Effective for Lowering Postprandial Glycaemia in Type 2 Diabetes Mellitus Than Advice That Does Not Specify Timing. Diabetologia. 2016;59(12):2572–2578.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: GLUT4 translocation and AMPK
- PubMed: resistance training and insulin sensitivity
- PubMed: post-meal walking and glucose
- PubMed: HIIT and insulin sensitivity
- PubMed: Zone 2 training and mitochondria
- PubMed: sedentary behavior and IR
- PubMed: exercise snacks and glycemic control
- PubMed: PCOS and resistance training
- PubMed: sarcopenic obesity and resistance training
Connections
- Blood Sugar & Insulin — interactive animation
- Fasting Insulin and HOMA-IR Testing
- Osteoporosis
- CGM for Non-Diabetics
- Insulin Resistance and PCOS
- Insulin Resistance
- Diabetes
- Obesity
- Metabolic Syndrome
- Reversal Protocol: Diet and Fasting
- NAFLD & MASLD Connection
- Metformin, Berberine and GLP-1s
- Metabolic Syndrome Cardiovascular Risk
- Sleep, Stress and Cortisol
- Fasting
- Blood Sugar
- CGM
- Visceral Fat