Continuous Glucose Monitors (CGM) for Non-Diabetics
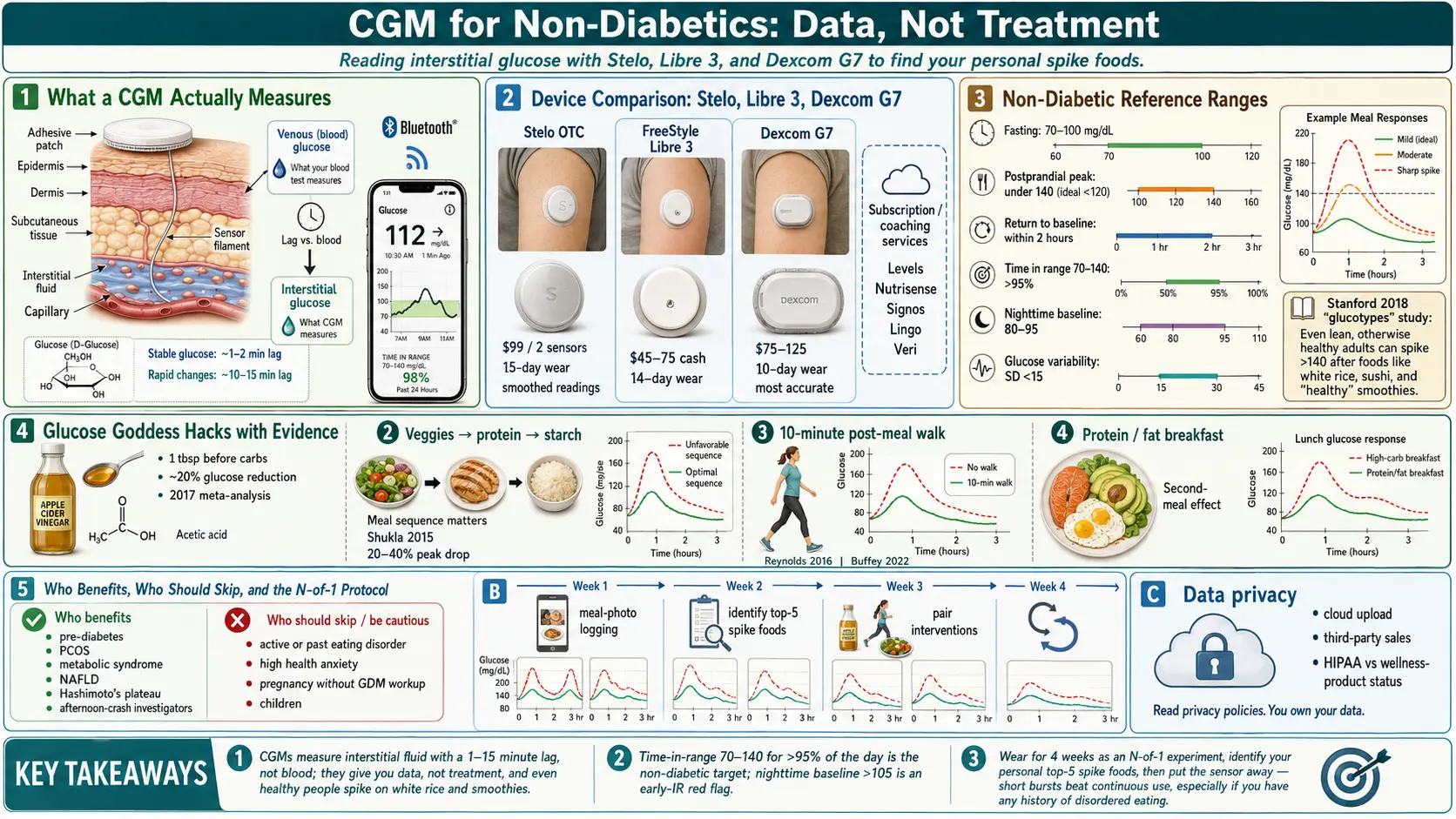
Table of Contents
- What a CGM Actually Measures
- Device Options — Dexcom, Libre, Medtronic, Stelo
- Non-Diabetic Subscription Services
- Getting a CGM Without Diabetes
- Interpretation Basics — What the Numbers Mean
- Realistic Expectations — Data, Not Treatment
- The N-of-1 Protocol — How to Actually Learn Something
- Glucose Goddess Hacks — What the Evidence Shows
- Who Benefits Most
- When NOT to Use a CGM
- Practical Troubleshooting — Skin, Sleep, Sensors
- Data Privacy Considerations
- Key Research Papers
- Connections
- Featured Videos
What a CGM Actually Measures
A continuous glucose monitor is a small disc that sticks to the back of your upper arm (or abdomen). A hair-thin filament sits in the fatty layer just under the skin and measures interstitial glucose — the sugar floating in the fluid between your cells — every one to five minutes. A Bluetooth chip sends the reading to your phone, where an app graphs it in near real time.
Here is the important technical detail most marketing glosses over: CGMs do not read blood sugar directly. They read interstitial fluid, which trails venous blood glucose by roughly one to two minutes when glucose is stable and up to ten to fifteen minutes when it is moving fast. That means if you check your CGM two minutes after chugging a soda, the spike you see on screen is already old news; the actual peak in your blood has already crested. And if you compare a CGM reading to a fingerstick meter taken at the same moment, they will almost never match exactly. A 10–15% discrepancy is normal, not a malfunction.
For someone without diabetes, this lag and accuracy range is fine. You are not dosing insulin. You are looking for patterns — does this meal spike me, does that walk flatten my curve — and patterns emerge clearly even with imperfect readings.
Device Options — Dexcom, Libre, Medtronic, Stelo
Four brands dominate the U.S. market, each with its own trade-offs.
Dexcom G7. Widely regarded as the most accurate consumer CGM. Wear time is 10 days. Cash price runs $75–$125 per sensor without insurance. Readings update every minute; no fingerstick calibration required. The app supports customizable alerts and integrates with the Apple Watch and Garmin.
FreeStyle Libre 3. The value pick. 14-day wear per sensor, $45–$75 cash. The newest generation is small (about the size of two stacked pennies), pushes readings to your phone every minute, and has meaningfully improved accuracy over earlier Libres. The app ecosystem is less polished than Dexcom's but works fine for non-diabetic pattern-finding.
Medtronic Guardian 4 / Simplera. The legacy clinical option, mostly used inside insulin-pump systems. Rarely what a non-diabetic picks; mentioned here only so you are not surprised if your endocrinologist offers it.
Stelo by Dexcom. In August 2024 the FDA approved Stelo as the first over-the-counter CGM for non-insulin-using adults. No prescription required. You buy it directly from dexcom.com or Amazon, roughly $99 for two sensors (about a month of wear) or a subscription near $89/month. Stelo is built on the same hardware platform as the G7 but has longer smoothing of readings and slightly different alert behavior, because Dexcom does not want non-diabetics panicking over every noisy spike. For most people reading this page, Stelo is now the simplest on-ramp.
Non-Diabetic Subscription Services
A parallel industry has grown up around the CGM — companies that ship you the sensor, an app, and a coaching layer so you do not have to interpret the data alone. They typically route you through a tele-prescribing doctor who writes a cash-pay Rx (this was the only legal path before Stelo existed).
- Levels. Pioneer of the category. App focuses on per-meal “zone scores” and a metabolic dashboard. Roughly $199 for your first month, then a subscription for sensors. Runs on Libre or Dexcom hardware.
- Nutrisense. Pairs the sensor with a registered dietitian who reviews your logs weekly. $299–$399 for a four-week starter; ongoing plans drop to around $250/month.
- Signos. Targets weight loss and exercise. Uses an algorithm to suggest workouts when glucose is rising. $143–$199/month on an annual plan.
- January AI. Uses only one or two weeks of CGM data, then predicts your glucose response to foods you have never eaten. After the initial wear, the sensor comes off and the AI takes over.
- Veri. European-built app with a clean interface; popular with Hashimoto's and PCOS users.
- Lingo. Abbott's own direct-to-consumer product (built on Libre hardware), priced around $89/month. Competes head-on with Stelo.
What are you actually paying for with a subscription? The hardware itself costs the company $30–$60. The premium goes to the app, the coaching, and the tele-prescribing middleman that Stelo has now made obsolete. If you are comfortable reading your own data, buying Stelo or a cash-pay Libre is half the price.
Getting a CGM Without Diabetes
Three legitimate paths in the U.S.:
1. Buy Stelo over the counter. No doctor required. Check out on dexcom.com, receive in 3–5 days. This is now the default.
2. Ask your primary care doctor for a prescription. If you have pre-diabetes (A1c 5.7–6.4), elevated fasting insulin (see HOMA-IR testing), PCOS, metabolic syndrome, or NAFLD, most physicians will write a cash-pay Rx for a Libre 3 or Dexcom G7 without much friction. Insurance usually will not cover it without a Type 1 or Type 2 diagnosis, but HSA and FSA funds are eligible for CGM sensors with a prescription — that is worth a 25–35% tax discount on the total cost.
3. Use a subscription service. Pay the premium for the concierge tele-prescribing + app. Convenient if your doctor refuses, or if you want the coaching layer.
Pharmacies like CVS, Walgreens, and many independents stock Libre and Dexcom sensors behind the counter. Bring a prescription and ask for the cash price — it is often lower than the list price if you decline insurance runs.
Interpretation Basics — What the Numbers Mean
Before you read your data, memorize the non-diabetic reference ranges. These are different from the ranges diabetics target because a healthy metabolism is considerably tighter than most CGM apps' default “in range” bands.
- Fasting glucose (morning, before eating): 70–100 mg/dL is normal. 100–125 is pre-diabetic. Over 125 on two separate tests is diabetic.
- Postprandial peak (1–2 hours after a meal): under 140 mg/dL is the goal for a healthy non-diabetic. Under 120 is ideal.
- Return to baseline: you should be back under 120 within two hours of eating, and within roughly 20 mg/dL of your fasting value by three hours.
- Time in range (70–140): a metabolically healthy adult spends more than 95% of the day inside this band.
- Nighttime baseline: most healthy adults cruise at 80–95 mg/dL overnight. A chronic overnight value over 105 is a red flag for early insulin resistance, even with a normal fasting morning number.
- Glucose variability (standard deviation): under 15 mg/dL over 24 hours indicates a smooth curve. Over 25 signals a roller-coaster pattern worth investigating.
Realistic Expectations — Data, Not Treatment
Here is the blunt version most influencers skip. A CGM gives you data. It does not give you treatment. If you have insulin resistance, the CGM cannot fix it; it can only show you which meals make it worse. And the difference between data and treatment is the difference between a bathroom scale and weight loss — one measures, the other requires work.
More importantly: healthy non-diabetic people spike, too. The 2018 Stanford “glucotypes” study by Michael Snyder's group put CGMs on 57 non-diabetic volunteers and found that standardized meals produced wildly different responses — and that even lean, fit, metabolically pristine subjects regularly peaked over 140, sometimes over 160, after foods you would consider blameless. Examples of foods that commonly spike non-diabetics:
- White rice, white bread, any refined grain. Glycemic index over 70 hits the bloodstream fast.
- Grapes, bananas, dates, mango. Fructose plus glucose, little fiber, easy to over-eat.
- “Healthy” smoothies. A Jamba-style cup can contain 70–90 g of sugar in liquid form — more than a can of soda.
- Breakfast cereal, even “fiber” brands.
- Sushi. The rice is usually doctored with sugar.
- Wine or beer on an empty stomach (biphasic: initial bump, then a reactive low 3–4 hours later).
Seeing your glucose hit 150 after a bowl of jasmine rice is not evidence you are pre-diabetic. It is evidence that you ate jasmine rice. Judge the metric by the pattern over days and weeks, not by a single alarm.
The N-of-1 Protocol — How to Actually Learn Something
The most useful framework for a non-diabetic CGM wearer is an N-of-1 experiment: you are the only subject, and the goal is to learn your specific responses, not general truths.
- Wear two sensors back to back (4 weeks total). One week is noise. Four weeks lets you see patterns across workdays, weekends, menstrual cycles, travel, and the stress curve of real life.
- Log every meal with a photo and a time-stamp. Most apps do this in two taps. Include the walk after, the wine, the coffee, the stressful meeting.
- Pair each meal photo with its 3-hour glucose curve. Look at three numbers: the peak, the time-to-peak, and the time-to-return-to-baseline. A tight curve peaking under 120 and back down by two hours is a “green” meal for you.
- Identify your personal top 5 spike foods. They will surprise you. For one person it is oats. For another it is grapes. For another it is a specific brand of protein bar sweetened with maltitol.
- Retest — the rematch round. In week three or four, repeat each spike meal with one variable changed: add fat, add fiber, add a 10-minute post-meal walk, eat it later in the day, pair it with protein. Learn the lowest-effort swap that flattens the curve.
- Stop wearing it. After a month you will know most of what the device can teach you. Put the sensor box away, apply the lessons, and re-wear for a week once or twice a year to recalibrate.
Glucose Goddess Hacks — What the Evidence Shows
Jessie Inchauspe's popular “Glucose Goddess” book codified a set of tricks that CGM-wearers consistently see working. Most have at least modest trial evidence behind them:
- One tablespoon of vinegar in water before a carb-heavy meal. A 2017 meta-analysis found a roughly 20% reduction in postprandial glucose across 11 small trials. The mechanism is slowed gastric emptying and inhibition of intestinal alpha-amylase.
- Eat veggies first, protein and fat second, starch and sugar last. Multiple small crossover trials show this sequence lowers the glucose peak by 20–40% compared with the same foods eaten in reverse.
- A 10-minute walk after eating. Even light walking activates muscle glucose uptake independent of insulin (GLUT4 translocation via contraction). Postprandial peaks drop 20–30%.
- Protein and fat at breakfast instead of sweet carbs. Eggs or Greek yogurt set a flatter curve for the whole day, in part because of next-meal glucose priming (the “second-meal effect”).
- Strength training 2–3x/week. The single biggest lever. See Exercise and Muscle Insulin Sensitivity.
What the hacks will not do is compensate for chronic overeating or a diet built on ultra-processed food. They are polish, not foundation.
Who Benefits Most
CGM as a short-term diagnostic tool is especially useful in:
- PCOS. Glucose variability often drives the weight, acne, and cycle irregularity. See PCOS.
- Pre-diabetes (A1c 5.7–6.4, HOMA-IR > 2). A single month of CGM-guided eating often drops A1c by 0.3–0.5 points at the next lab draw.
- Metabolic syndrome. Three of the five criteria (waist, triglycerides, glucose, HDL, blood pressure) can shift within weeks of CGM-driven changes.
- Hashimoto's with a weight plateau. People on stable thyroid medication who cannot lose weight often uncover hidden carbohydrate intolerance via CGM.
- Unexplained fatigue or “afternoon crashes.” Many are reactive hypoglycemia following a high-glycemic meal — visible instantly on a CGM trace.
- Athletes dialing fueling strategy. Training zones, fasted work, and carbohydrate tolerance are all legible on a CGM.
When NOT to Use a CGM
This is the section most CGM marketing pretends does not exist. A CGM is a powerful tool and, like any powerful tool, it is contraindicated in some people.
- Active or recent eating disorder. Anorexia, bulimia, orthorexia, and ARFID are absolute contraindications. A CGM gives a restrictive mindset more to restrict. If you have ever been treated for an eating disorder, talk to your clinician before ordering one — and probably don't.
- High baseline health anxiety. If you already catastrophize lab numbers, watching your glucose bounce around all day will not calm you down. It will create new fears about foods that were never a problem.
- Pregnancy (unless gestational diabetes is being worked up). Non-diabetic pregnant women generally do not benefit from CGM and may worsen food anxiety during an already stressful period.
- Children and adolescents without a medical indication. CGM in kids needs clinical supervision; it is not a quantified-self toy.
- People who will not act on the data. If you know you will read the data, feel guilty, and not change anything, skip the device. It becomes an expensive source of shame.
Practical Troubleshooting — Skin, Sleep, Sensors
Skin reactions. About 10–20% of wearers develop itching or a rash at the adhesive site within a few wears. Fixes, in order of escalation:
- Rotate sites — alternate arms, try the upper abdomen with a prescription Rx.
- Wipe the site with an alcohol swab and let it dry fully before applying.
- Apply a thin hydrocolloid or IV-prep barrier patch (Skin Tac, SKINtac, Tegaderm, or a dedicated CGM patch like Simpatch) before the sensor.
- If a persistent rash develops, stop and consult your doctor — isobornyl acrylate (IBOA) allergy is well-documented with older Libre generations.
Sleep-disturbing alerts. Default low-glucose alarms are calibrated for Type 1 diabetics and will go off at 70 mg/dL — a number that is perfectly normal for a non-diabetic overnight. Turn the low alert off, or set it at 55 mg/dL. Stelo disables it by default for exactly this reason.
Sensor failures. Expect one in every 5–10 sensors to fail early — signal loss, premature shutdown, bad adhesive. All three manufacturers replace failed sensors for free if you call the support line within the warranty window (usually 14 days).
Compression lows. Sleeping on top of the sensor squeezes interstitial fluid out of the area and produces a fake low reading. Real number; artifact reading. If you see a low that appears only at night and resolves the moment you roll over, this is why.
Acetaminophen and high-dose vitamin C can briefly skew readings upward on older Dexcom sensors; the G7 and Stelo are much less affected.
Data Privacy Considerations
Every CGM subscription service uploads your glucose data to the cloud. Read the privacy policy before you agree. Questions to ask:
- Is the data de-identified and sold to third parties (food brands, pharma, insurers)?
- Can you export and delete your complete dataset on request?
- Is the data covered by HIPAA (usually yes if prescribed) or only by the company's privacy policy (usually the case for OTC wellness products like Stelo)?
- If the company is acquired, where does the dataset go?
These are not paranoid questions. Glucose curves, paired with meal photos and timestamps, are among the most behaviorally revealing datasets that exist. Treat them accordingly.
Key Research Papers
Foundational publications on continuous glucose monitoring in non-diabetic populations, glucose variability, and the behavioral interventions revealed by CGM data. Each citation links to the full text via DOI.
- Hall H, Perelman D, Breschi A, et al. Glucotypes Reveal New Patterns of Glucose Dysregulation. PLoS Biology. 2018;16(7):e2005143.
- Shah VN, DuBose SN, Li Z, et al. Continuous Glucose Monitoring Profiles in Healthy Nondiabetic Participants: A Multicenter Prospective Study. Journal of Clinical Endocrinology & Metabolism. 2019;104(10):4356–4364.
- Zeevi D, Korem T, Zmora N, et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell. 2015;163(5):1079–1094.
- Klonoff DC, Nguyen KT, Xu NY, et al. The Need for Accuracy in Over-the-Counter Continuous Glucose Monitors. Journal of Diabetes Science and Technology. 2023;17(3):599–601.
- Battelino T, Danne T, Bergenstal RM, et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care. 2019;42(8):1593–1603.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin (Diabetes Prevention Program). New England Journal of Medicine. 2002;346(6):393–403.
- Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man (HOMA). Diabetologia. 1985;28(7):412–419.
- Reaven GM. Banting Lecture 1988. Role of Insulin Resistance in Human Disease. Diabetes. 1988;37(12):1595–1607.
- Petersen MC, Shulman GI. Mechanisms of Insulin Action and Insulin Resistance. Physiological Reviews. 2018;98(4):2133–2223.
- Saltiel AR, Olefsky JM. Inflammatory Mechanisms Linking Obesity and Metabolic Disease. Journal of Clinical Investigation. 2017;127(1):1–4.
- Reynolds AN, Mann JI, Williams S, Venn BJ. Advice to Walk After Meals Is More Effective for Lowering Postprandial Glycaemia in Type 2 Diabetes Mellitus Than Advice That Does Not Specify Timing. Diabetologia. 2016;59(12):2572–2578.
- Shukla AP, Iliescu RG, Thomas CE, Aronne LJ. Food Order Has a Significant Impact on Postprandial Glucose and Insulin Levels. Diabetes Care. 2015;38(7):e98–e99.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: CGM in non-diabetic adults
- PubMed: CGM and pre-diabetes
- PubMed: CGM in PCOS
- PubMed: post-meal walking and glucose
- PubMed: vinegar and postprandial glucose
- PubMed: meal sequence and glucose
- PubMed: glucose variability and metabolic syndrome
- PubMed: CGM and orthorexia risk
Connections
- Endocrinology
- Blood Sugar & Insulin — interactive animation
- Exercise and Muscle Insulin Sensitivity
- Fasting Insulin and HOMA-IR Testing
- Polycystic Ovary Syndrome
- Diabetes
- Insulin Resistance
- Metabolic Syndrome
- Reversal Protocol: Diet and Fasting
- Insulin Resistance and PCOS
- NAFLD & MASLD Connection
- Metformin, Berberine and GLP-1s
- Metabolic Syndrome Cardiovascular Risk
- CGM
- Fasting
- Blood Sugar
- Obesity
- Fasting Insulin
- Ultra-Processed Foods
- Sleep, Stress & Cortisol in Insulin Resistance