Alpha Lipoic Acid (ALA / Thioctic Acid)
Alpha Lipoic Acid (ALA) is a sulfur-containing antioxidant cofactor synthesized in mitochondria from octanoic acid and cysteine. It is the only known antioxidant active in both lipid and aqueous compartments, the only one that crosses the blood-brain barrier readily, and the only one that can regenerate every other major antioxidant in the body — vitamin C, vitamin E, glutathione, and CoQ10. It has been a prescription drug in Germany for diabetic neuropathy since 1966 and remains the most clinically validated nutraceutical for nerve pain.
Interactive Visualization Mitochondria & ATP — watch your cells make energy Follow electrons through the transport chain and watch the ATP-synthase motor spin — then block Complex IV and see the chain stall. Launch → Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- Biochemistry & Endogenous Synthesis
- Mitochondrial Function & Bioenergetics
- Diabetic Peripheral Neuropathy (Headline Indication)
- Antioxidant Recycling Network
- Insulin Sensitivity & Blood Sugar Control
- Heavy Metal Chelation & Liver Protection
- Neuroprotection & Cognitive Function
- Cardiovascular Protection
- Skin Health & Anti-Glycation
- Forms: R-ALA vs Racemic, IV vs Oral
- Recommended Dosage
- Cautions and Contraindications
- Research Papers and References
- Connections
- Featured Videos
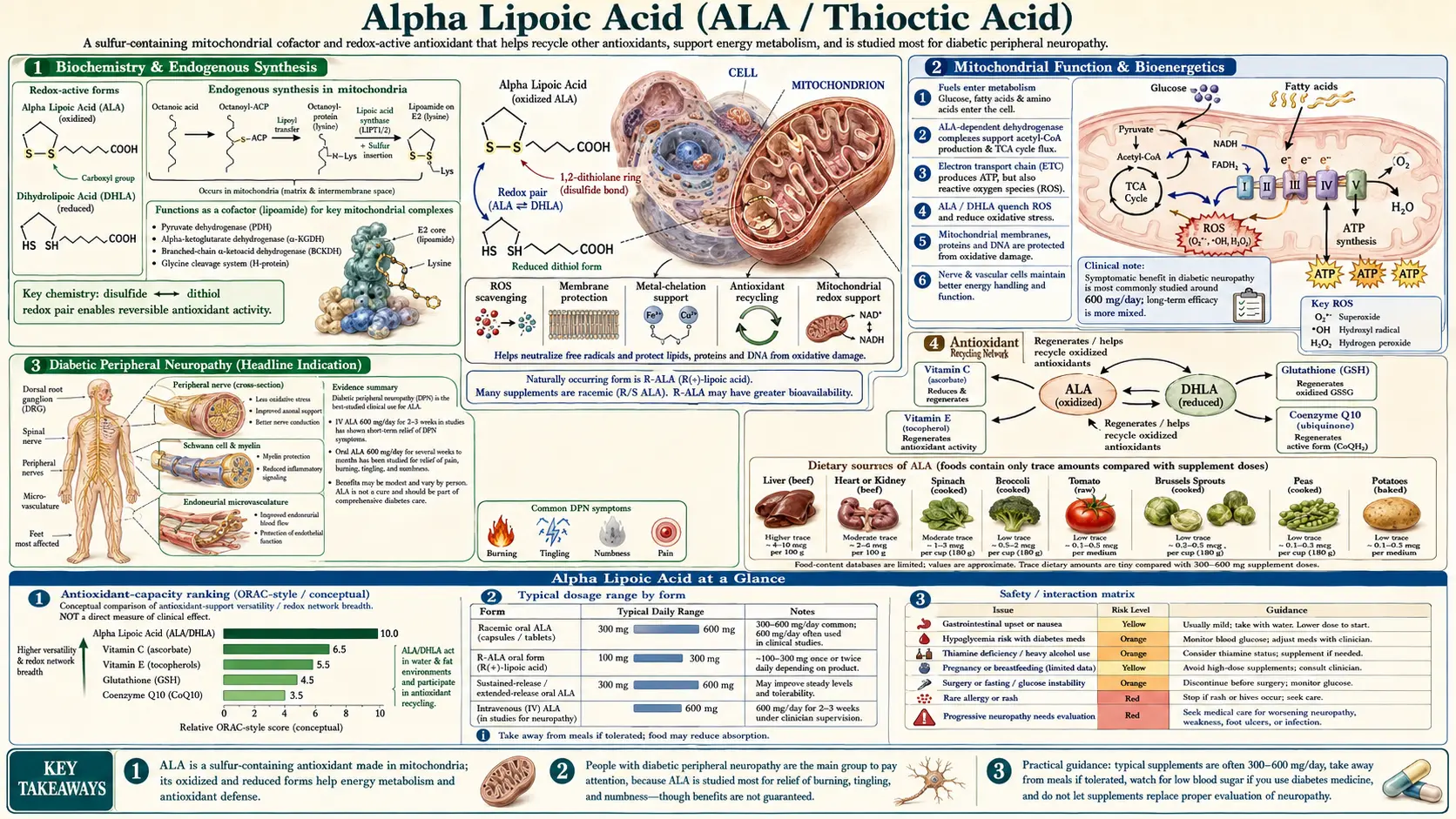
Biochemistry & Endogenous Synthesis
Alpha lipoic acid is a short-chain fatty acid (1,2-dithiolane-3-pentanoic acid) with a unique five-membered ring containing two sulfur atoms in a disulfide bond. This ring is the redox-active center: it cycles between the oxidized form (alpha lipoic acid, or ALA) and the reduced form (dihydrolipoic acid, or DHLA), donating two electrons each time it converts.
The body synthesizes small amounts of ALA in mitochondria from octanoic acid (a medium-chain fatty acid) and the sulfur from cysteine. Lipoic acid synthase (LIAS) attaches the lipoyl group directly onto the lysine residues of four mitochondrial enzyme complexes — a post-translational modification called lipoylation. Endogenously synthesized ALA is therefore not free; it is covalently bound to enzyme proteins where it serves as a swinging arm that shuttles intermediates between active sites.
Free, unbound ALA — the form available from supplements and the small amount in food — behaves very differently. It enters cells freely, crosses the blood-brain barrier, distributes into both watery and fatty compartments, and exerts antioxidant and signaling effects that the protein-bound form cannot. Dietary sources are minor (organ meats, spinach, broccoli, yeast) and provide nowhere near the amounts used therapeutically.
ALA exists as two mirror-image forms: the natural R-isomer (R-LA), made by the body and found in food, and the synthetic S-isomer (S-LA), which arises only from chemical synthesis. Most supplements sold as "alpha lipoic acid" are a racemic 50/50 mixture of R and S. The R-form is substantially more bioactive — it has higher cellular uptake, is the form recognized by the lipoyl-binding domains, and produces stronger metabolic effects per milligram.
Mitochondrial Function & Bioenergetics
Protein-bound lipoic acid is essential to four mitochondrial enzyme complexes that together control the entry of carbon into the citric acid cycle and the catabolism of branched-chain amino acids:
- Pyruvate dehydrogenase complex (PDH) — converts pyruvate (from glycolysis) to acetyl-CoA, the gateway molecule of the TCA cycle. PDH is the rate-limiting step for carbohydrate oxidation. ALA serves as the dithiolane cofactor on the E2 subunit (dihydrolipoyl transacetylase).
- Alpha-ketoglutarate dehydrogenase complex (α-KGDH) — the rate-limiting enzyme of the TCA cycle itself, converting α-ketoglutarate to succinyl-CoA. ALA again serves as the swinging cofactor.
- Branched-chain α-keto acid dehydrogenase (BCKDH) — catabolizes leucine, isoleucine, and valine; defects cause maple syrup urine disease.
- Glycine cleavage system (GCS) — degrades glycine for one-carbon metabolism and methylation.
When mitochondrial ALA supply is adequate, these enzymes run efficiently and ATP production proceeds with minimal electron leak. When lipoylation is impaired — as occurs in aging, oxidative stress, and metabolic disease — PDH and α-KGDH slow down, pyruvate is shunted toward lactate, and the TCA cycle stalls. The result is reduced ATP yield, elevated lactate, and increased reactive oxygen species (ROS) production from the dysfunctional electron transport chain.
Supplemental ALA, even though most of it does not become protein-bound, supports mitochondrial function in three ways: it directly quenches ROS leaking from the electron transport chain; it regenerates oxidized CoQ10 (ubiquinol) in the mitochondrial inner membrane; and it preserves the activity of mitochondrial antioxidant enzymes by maintaining cellular glutathione status. The landmark mitochondrial-aging research by Bruce Ames and Tory Hagen at UC Berkeley demonstrated that combining ALA with acetyl-L-carnitine reverses age-related mitochondrial decline in old rats, restoring memory, ambulation, and mitochondrial membrane potential to youthful levels.
Diabetic Peripheral Neuropathy (Headline Indication)
Diabetic peripheral neuropathy — the burning, tingling, electric-shock pain that affects more than half of long-term diabetics — is the indication for which ALA has the strongest evidence base of any nutraceutical for any condition. ALA has been a licensed prescription drug for this indication in Germany (under the name Thioctsäure or Tioctan) since 1966, and the major clinical trials — the ALADIN, SYDNEY, ORPIL, DEKAN, and NATHAN series — were funded specifically to satisfy European drug regulators.
The mechanistic case is strong. Hyperglycemia damages peripheral nerves through five overlapping pathways: increased polyol flux through aldose reductase (sorbitol accumulation), advanced glycation end-product (AGE) formation, protein kinase C activation, hexosamine pathway flux, and most importantly, mitochondrial superoxide overproduction in the small dorsal-root ganglion neurons. ALA addresses every one of these — it inhibits aldose reductase, scavenges the ROS that drive the other four pathways, and restores intraneural blood flow that is reduced in diabetic microvascular disease.
Key trial results
- ALADIN I (1995, Ziegler et al., Diabetologia) — 328 patients with type 2 diabetes and symptomatic neuropathy. Intravenous ALA 600 mg/day for 3 weeks produced significant reductions in pain, paresthesia, and numbness on the Total Symptom Score (TSS) versus placebo. Established the 600 mg/day IV dose as standard.
- ALADIN II (1999, Reljanovic et al.) — 2-year oral follow-up. Sustained improvement in nerve conduction velocity, particularly in the sural nerve.
- ALADIN III (1999, Ziegler et al., Diabetes Care) — 509 patients. 3-week IV induction followed by 6 months of oral 1800 mg/day. Improvement in neuropathic deficit (NIS) score versus placebo.
- SYDNEY 1 (2003, Ametov et al., Diabetes Care) — IV ALA 600 mg/day for 14 daily infusions reduced TSS by 5.7 points versus 1.8 for placebo; 52% of ALA patients achieved >50% pain reduction.
- SYDNEY 2 (2006, Ziegler et al., Diabetes Care) — Oral ALA 600, 1200, or 1800 mg/day for 5 weeks. All three doses significantly reduced TSS versus placebo, with no additional benefit above 600 mg/day. Established 600 mg/day as the optimal oral dose.
- NATHAN 1 (2011, Ziegler et al., Diabetes Care) — The 4-year landmark trial. 460 patients on oral ALA 600 mg/day or placebo. Significant improvement in the Neuropathy Impairment Score - Lower Limbs (NIS-LL). Established long-term oral safety and continued efficacy.
- DEKAN trial (Ziegler et al., Diabetes Care 1997) — Cardiac autonomic neuropathy. Oral ALA 800 mg/day for 4 months improved heart-rate variability indices.
The 2012 Cochrane-style meta-analysis by Mijnhout et al. pooled 1,160 patients from 4 trials and concluded that IV ALA 600 mg/day for 3 weeks produces a clinically meaningful reduction in pain, paresthesia, and numbness. The pooled odds ratio for >50% pain reduction was 2.96 (95% CI 1.97-4.45).
In clinical practice the typical protocol is 600 mg IV daily for 2-4 weeks followed by 600 mg/day oral for indefinite maintenance. Oral-only protocols at 600 mg/day are also effective but the time to clinical response is longer (4-8 weeks vs 2-3 weeks for IV).
Antioxidant Recycling Network
ALA's most striking property is its position at the center of the body's antioxidant network. Most antioxidants work in one compartment only — vitamin C in the watery cytosol and plasma, vitamin E in lipid membranes, glutathione in the cytosol. ALA crosses freely between them and, in its reduced DHLA form, can donate electrons to regenerate every other major antioxidant after they have been oxidized:
- Regenerates oxidized vitamin C (dehydroascorbate) back to active ascorbate
- Regenerates oxidized vitamin E (tocopheryl radical) in cell membranes, allowing it to quench another lipid radical
- Regenerates oxidized glutathione (GSSG) back to reduced glutathione (GSH), bypassing the normal glutathione-reductase pathway when NADPH is limiting
- Regenerates oxidized CoQ10 (ubiquinone) back to ubiquinol in mitochondrial membranes
- Directly scavenges hydroxyl radicals, hypochlorous acid, peroxyl radicals, peroxynitrite, and singlet oxygen
Because the body itself converts most ingested ALA to DHLA inside cells (via the lipoamide dehydrogenase enzyme), supplemental ALA effectively becomes a slow-release reservoir of reducing power that keeps the network charged. This is the mechanistic basis for the broad clinical effects: when ALA is supplied, every downstream antioxidant operates at higher capacity, and oxidative stress markers (8-OHdG, F2-isoprostanes, oxidized LDL) consistently fall in human trials.
ALA also activates the Nrf2 pathway — the master transcription factor that upregulates more than 200 endogenous cytoprotective genes, including glutathione synthesis enzymes (GCLC, GCLM), NADPH-quinone oxidoreductase (NQO1), heme oxygenase-1 (HO-1), and glutathione-S-transferases. This means ALA does not just provide antioxidant activity directly; it also induces the body to make more of its own antioxidant machinery.
Insulin Sensitivity & Blood Sugar Control
Independent of its neuropathy effects, ALA improves whole-body insulin sensitivity and glucose disposal. The mechanisms are multiple: ALA activates AMP-activated protein kinase (AMPK) in skeletal muscle, mimicking the metabolic signal of exercise; it stimulates GLUT4 glucose transporter translocation to the muscle cell membrane; and it reduces the inflammatory oxidative stress that drives insulin receptor desensitization in adipose tissue.
The clinical effect on HbA1c is modest but real. Meta-analyses of oral ALA trials in type 2 diabetes show average HbA1c reductions of 0.3-0.5 percentage points at doses of 300-600 mg/day, with greater effects in patients with worse baseline control. Fasting glucose typically falls 5-20 mg/dL. These are not metformin-magnitude effects, but ALA is a useful adjunct, particularly in patients who also have neuropathy and would be taking it anyway.
In metabolic syndrome and prediabetes, several small trials have shown improvements in fasting insulin and HOMA-IR after 8-12 weeks of 600 mg/day oral ALA. The combination of ALA + berberine + chromium is used by many functional medicine practitioners for insulin resistance, exploiting three different AMPK-related mechanisms.
Heavy Metal Chelation & Liver Protection
The dithiol structure of DHLA forms stable complexes with toxic heavy metals, including mercury, arsenic, lead, cadmium, and excess copper or iron. Because both ALA and DHLA cross cell membranes (and the blood-brain barrier), this chelation activity reaches tissue compartments that hydrophilic chelators like DMSA, DMPS, and EDTA cannot access.
ALA is the central agent in the Andy Cutler protocol — a frequent low-dose oral chelation method developed for individuals with chronic mercury toxicity from amalgam fillings or seafood exposure. The protocol uses doses as small as 12.5-50 mg every 3-4 hours (matching ALA's short plasma half-life) to mobilize and excrete mercury without redistributing it to the brain. This approach remains controversial in mainstream toxicology but is widely used in integrative medicine for documented cases of body-burden heavy metal accumulation.
Independently of chelation, ALA strongly protects the liver. It raises hepatic glutathione, reduces lipid peroxidation in hepatocyte membranes, and has been used clinically since the 1970s in cases of Amanita phalloides (death-cap mushroom) poisoning — one of the few interventions shown to prevent fulminant liver failure when given within 24-48 hours of ingestion. It is also studied in non-alcoholic fatty liver disease (NAFLD), where it modestly reduces transaminases and hepatic steatosis on imaging.
For routine detox and liver support, ALA pairs naturally with NAC (glutathione precursor), milk thistle (silymarin), and selenium — a quartet that supports phase I and phase II hepatic biotransformation and glutathione synthesis simultaneously.
Neuroprotection & Cognitive Function
The brain is uniquely vulnerable to oxidative damage — it consumes 20% of the body's oxygen, is rich in polyunsaturated fatty acids, and has limited antioxidant reserves. ALA is one of the few antioxidants that readily crosses the blood-brain barrier in both oxidized and reduced forms, making it valuable for central nervous system protection.
In Alzheimer's disease, small open-label trials (Hager et al., 2007) found that 600 mg/day oral ALA for 12 months stabilized cognitive decline in patients with mild-to-moderate AD, compared to expected progression. The proposed mechanism is reduction of beta-amyloid-induced oxidative stress in hippocampal neurons.
In multiple sclerosis, the LAPMS pilot trial (Yadav et al., 2010) and a larger 2-year Oregon Health & Science University study (2017) found that 1,200 mg/day oral ALA significantly reduced annualized brain atrophy on MRI compared to placebo in secondary-progressive MS, with effect sizes comparable to natalizumab. The mechanism likely involves reduced oxidative damage to oligodendrocytes and improved mitochondrial function in axons under chronic inflammatory stress.
In stroke recovery, animal models consistently show that ALA pretreatment or early post-stroke administration reduces infarct size by 30-50%, attributed to reduced excitotoxic glutamate release and improved mitochondrial calcium handling. Human trials are limited.
ALA also shows promise in chemotherapy-induced peripheral neuropathy, where the mechanisms overlap with diabetic neuropathy, and in age-related cognitive decline, where the Ames-Hagen rodent work translated into improvements in subjective memory and processing speed in pilot human trials of ALA + acetyl-L-carnitine.
Cardiovascular Protection
ALA improves endothelial function — the ability of arterial linings to dilate in response to nitric oxide. In patients with metabolic syndrome and impaired glucose tolerance, 600 mg/day oral ALA for 4 weeks improved flow-mediated dilation in the brachial artery by 44-72%, a magnitude similar to statin therapy. The mechanism is reduced oxidative destruction of nitric oxide and increased availability of the NO substrate arginine.
Additional cardiovascular effects include modest blood pressure reduction (typically 3-5 mmHg systolic in hypertensive patients), reduced LDL oxidation, improved triglyceride profiles, and reduced inflammatory markers like high-sensitivity C-reactive protein. In diabetic patients, ALA reduces albumin excretion — an early marker of vascular and renal damage.
Because ALA improves both microvascular blood flow and endothelial responsiveness, it is studied as adjunctive therapy in conditions characterized by impaired vascular function: cardiovascular disease, peripheral arterial disease, erectile dysfunction, and Raynaud's phenomenon.
Skin Health & Anti-Glycation
Topical ALA at 3-5% concentration has been studied for fine lines, photoaging, and skin roughness. A 2003 double-blind split-face study by Beitner found that 12 weeks of topical 5% ALA significantly reduced facial fine lines, particularly around the eyes and upper lip, and improved skin smoothness and color.
The mechanism is anti-glycation — ALA blocks the formation of advanced glycation end-products (AGEs), the cross-linked sugar-protein structures that stiffen collagen and elastin and produce the characteristic appearance of glycated, aged skin. ALA also reduces inflammation in skin and supports the regeneration of intracellular glutathione in keratinocytes exposed to UV damage.
Oral ALA contributes to skin health through the same mechanisms applied systemically: reduced glycation throughout the dermis, improved microcirculation, and protection of skin lipids from peroxidation. Pairing with topical vitamin C and vitamin E creates synergistic dermal antioxidant defense.
Forms: R-ALA vs Racemic, IV vs Oral
- Racemic alpha lipoic acid — a 50/50 mixture of R-ALA (natural, bioactive) and S-ALA (synthetic mirror image). The standard, low-cost form found in most supplements. Effective but requires roughly double the dose of R-ALA to achieve the same plasma R-ALA levels.
- R-Alpha Lipoic Acid (R-ALA, R-LA) — the natural enantiomer alone, manufactured by enzymatic resolution or asymmetric synthesis. Approximately twice as bioavailable as racemic ALA on a per-milligram basis. More expensive.
- Sodium R-Lipoate (Na-R-ALA, Bio-Enhanced R-Lipoic Acid) — a stabilized sodium salt of R-ALA. The most chemically stable oral form — pure R-ALA degrades at temperatures above 40°C, but Na-R-ALA tolerates handling, transport, and shelf life better. Higher plasma concentrations than equivalent doses of free R-ALA.
- Intravenous ALA — pharmaceutical-grade racemic ALA 600 mg in saline, infused over 30-60 minutes. Achieves plasma concentrations 10-20× higher than equivalent oral doses. Used clinically for diabetic neuropathy induction therapy, severe oxidative stress, mushroom poisoning, and heavy metal mobilization. Available by prescription in Germany and some European countries; off-label use in IV nutrient therapy clinics elsewhere.
- Slow-release oral formulations — address ALA's very short plasma half-life (30-60 minutes) by extending absorption over 4-6 hours. Trials are limited but plasma kinetics are improved.
- Topical creams and serums — 1-5% ALA in dermatological formulations for anti-aging, particularly around the eyes and on photodamaged skin.
Practical guidance: For most antioxidant and general-health purposes, racemic ALA at 300-600 mg/day is the cost-effective choice. For mitochondrial-targeted longevity protocols (Bruce Ames-style) and patients responding poorly to racemic, R-ALA or Na-R-ALA at 150-300 mg/day is preferred. For diabetic neuropathy, follow the trial protocols (600 mg/day IV induction then oral maintenance).
Recommended Dosage
- General antioxidant support — 100-300 mg/day racemic ALA, taken with breakfast on an empty stomach or 30 minutes before
- Metabolic syndrome & insulin sensitivity — 300-600 mg/day racemic, or 150-300 mg/day R-ALA, divided into 2-3 doses
- Diabetic peripheral neuropathy (oral protocol) — 600 mg/day racemic, taken as one 600 mg dose or 300 mg twice daily, on an empty stomach. Expect 4-8 weeks to assess response. Sustained use is required — symptoms typically return on discontinuation.
- Diabetic peripheral neuropathy (IV protocol) — 600 mg/day IV in 250 mL saline, infused over 30-60 minutes, 5 days per week for 2-4 weeks, followed by indefinite oral 600 mg/day maintenance
- Cognitive support / mitochondrial longevity — 300-600 mg/day ALA combined with 500-1000 mg/day acetyl-L-carnitine (the Ames-Hagen protocol)
- Heavy metal mobilization (Cutler protocol) — 12.5-50 mg every 3-4 hours during waking hours, only initiated after dental amalgam removal; protocol detail and timing matter and clinical supervision is recommended
- Multiple sclerosis (Yadav protocol) — 1,200 mg/day oral racemic, divided into 2 doses; off-label investigational use
- Topical anti-aging — 3-5% cream or serum applied once or twice daily to clean skin; expect 8-12 weeks for visible effects
Timing matters. ALA absorption is reduced 30-50% when taken with food (especially carbohydrate-rich meals), so it should be taken on an empty stomach — either 30 minutes before a meal or 2 hours after. Plasma half-life is short (about 30 minutes for racemic ALA, 60 minutes for R-ALA), but cellular effects persist much longer because ALA enters the redox-cycling pool inside cells.
Cautions and Contraindications
ALA is generally well tolerated. The most important considerations:
- Hypoglycemia risk in diabetics — ALA enhances insulin sensitivity and glucose uptake. Patients on insulin, sulfonylureas (glipizide, glyburide), or other glucose-lowering medications should monitor blood sugar closely when starting ALA, as dose adjustments are often required to avoid hypoglycemia.
- Insulin Autoimmune Syndrome (IAS / Hirata's disease) — a rare but serious adverse effect, reported almost exclusively in Japanese, Korean, and Chinese populations carrying the HLA-DRB1*04:06 allele (which has very high prevalence in East Asian genetic backgrounds and rare in European/African descent). IAS presents as severe spontaneous hypoglycemia from autoantibodies against endogenous insulin. ALA use should be approached cautiously in patients of East Asian descent.
- Biotin depletion — long-term high-dose ALA can deplete biotin (vitamin B7) by competing for cellular uptake. A modest biotin supplement (300-500 mcg/day) is reasonable for anyone taking >600 mg ALA/day for more than a few months.
- Thiamine (vitamin B1) dependency — PDH and α-KGDH (the enzymes ALA activates) require thiamine pyrophosphate as a co-substrate. In thiamine-deficient individuals — particularly chronic alcoholics — high-dose ALA could theoretically worsen thiamine demand and precipitate Wernicke encephalopathy. Co-supplement thiamine in any at-risk population.
- Thyroid hormone — ALA may slightly inhibit peripheral T4-to-T3 conversion in some patients; monitor TSH and free T3 in hypothyroid individuals who add ALA.
- Drug interactions — theoretically enhances the effects of insulin, sulfonylureas, metformin, GLP-1 agonists, and any glucose-lowering medication; can chelate certain mineral supplements taken at the same time (separate by 2 hours)
- GI side effects — nausea, indigestion, and rare allergic skin reactions at higher oral doses; usually resolves with food (at the cost of absorption) or dose reduction
- Pregnancy and breastfeeding — limited human safety data; avoid in the absence of clinical guidance
- Children — safety data limited; not recommended outside of supervised clinical use for specific indications
Research Papers and References
The following PubMed search links provide curated entry points into the published clinical and mechanistic literature on alpha lipoic acid. Each link opens directly in PubMed at the National Library of Medicine.
- ALA and diabetic peripheral neuropathy (the ALADIN/SYDNEY/NATHAN evidence base) — PubMed: alpha lipoic acid diabetic neuropathy
- NATHAN 1 trial (4-year oral ALA for neuropathy) — PubMed: NATHAN 1 alpha lipoic acid Ziegler
- SYDNEY 2 trial (oral dose-response) — PubMed: SYDNEY 2 alpha lipoic acid
- ALA mitochondrial function and aging (Ames / Hagen) — PubMed: alpha lipoic acid acetyl carnitine aging mitochondria
- ALA and insulin sensitivity, HbA1c, type 2 diabetes — PubMed: alpha lipoic acid insulin sensitivity HbA1c
- ALA in multiple sclerosis (LAPMS / Yadav) — PubMed: alpha lipoic acid multiple sclerosis brain atrophy
- ALA and Alzheimer's disease cognition — PubMed: alpha lipoic acid Alzheimer cognition
- ALA antioxidant recycling: regenerating vitamin C, vitamin E, glutathione — PubMed: alpha lipoic acid antioxidant recycling
- ALA and Nrf2 pathway activation — PubMed: alpha lipoic acid Nrf2
- ALA and heavy metal chelation (mercury, arsenic, lead) — PubMed: alpha lipoic acid mercury chelation
- ALA hepatoprotection and non-alcoholic fatty liver disease (NAFLD) — PubMed: alpha lipoic acid NAFLD liver
- ALA endothelial function and cardiovascular — PubMed: alpha lipoic acid endothelial function
- Topical ALA for photoaging and skin (Beitner) — PubMed: alpha lipoic acid topical photoaging
- Insulin Autoimmune Syndrome (Hirata's disease) and ALA — PubMed: alpha lipoic acid insulin autoimmune syndrome
- R-alpha lipoic acid versus racemic bioavailability — PubMed: R alpha lipoic acid bioavailability
External Authoritative Resources
- Linus Pauling Institute — Lipoic Acid Micronutrient Information Center
- NCCIH — Herbs and Supplements at a Glance
- MedlinePlus — Alpha Lipoic Acid
- PubMed — All research on alpha lipoic acid
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- Mitochondria & ATP — interactive animation
- All Antioxidants
- Diabetes
- Diabetic Complications
- Peripheral Neuropathy
- Oxidative Stress
- NAC (N-Acetylcysteine)
- NAD+ & NMN
- Methylene Blue
- Detox Protocols
- Liver Cleansing
- Longevity Protocols
- Blood Sugar
- Vitamin C
- Vitamin E
- Vitamin B7 (Biotin)
- Vitamin B1 (Thiamine)
- Selenium
- Sulfur
- Cysteine
- Glycine
- Methionine
- Taurine
- Arginine
- Berberine
- Milk Thistle
- Turmeric (Curcumin)
- Astragalus
- Quercetin
- Hemoglobin A1c
- Fasting Insulin
- Continuous Glucose Monitor
- Mercury
- Lead
- Arsenic
- Neurology
- Cardiovascular Disease