Continuous Glucose Monitor (CGM): Real-Time Metabolic Insight Through a Sensor on Your Arm
A continuous glucose monitor (CGM) is a small adhesive sensor — about the size of a large coin — worn on the upper arm or abdomen for 10 to 14 days, which measures interstitial glucose every few minutes and transmits results to a smartphone in real time. Originally developed for people with type 1 diabetes, CGMs are now widely used by people with type 2 diabetes, by metabolic-health enthusiasts without diabetes, and by athletes and shift workers interested in personalized glycemic patterns. In the United States, the FDA approved the first over-the-counter CGM (Dexcom Stelo) in 2024, and Abbott launched Lingo and Libre Rio; European users have had direct-to-consumer access for longer.
This article explains how a CGM works, what useful information it actually provides for non-diabetic adults, how to interpret the data, common pitfalls, and whether the price is justified for your situation.
Interactive Visualization Glycation & HbA1c — sugar-coat a red cell and watch the number lag Coat red blood cells in glucose for 120 days and watch HbA1c emerge as their average — then normalize the sugar today and see why the number takes months to follow. Launch →Table of Contents
- How a CGM Works
- Devices and Brands
- What You Actually Learn
- Key Metrics to Track
- Is a CGM Useful for Non-Diabetics?
- Pitfalls and Misinterpretation
- Cost and Insurance
- Connections
- Featured Videos
How a CGM Works
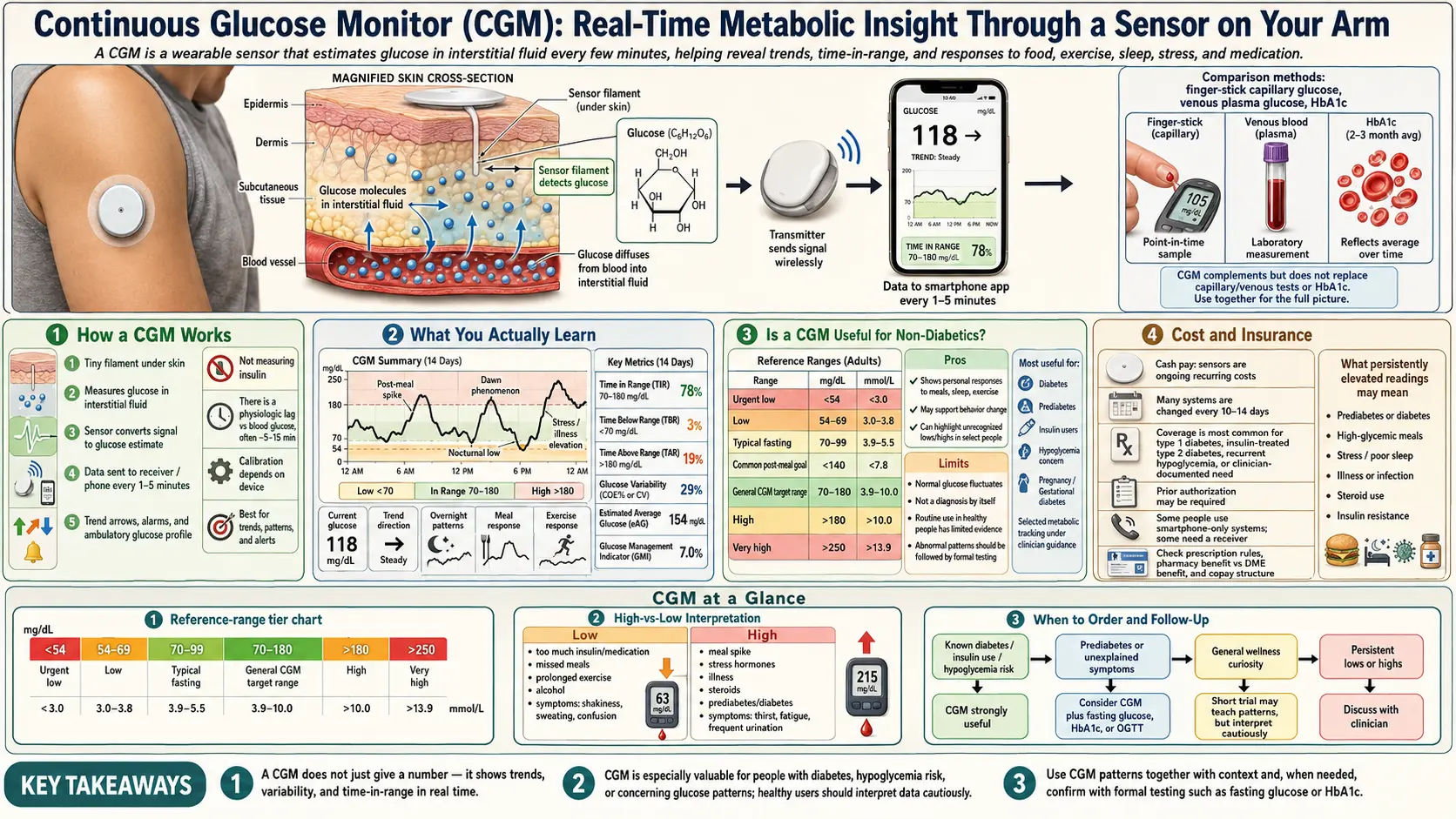
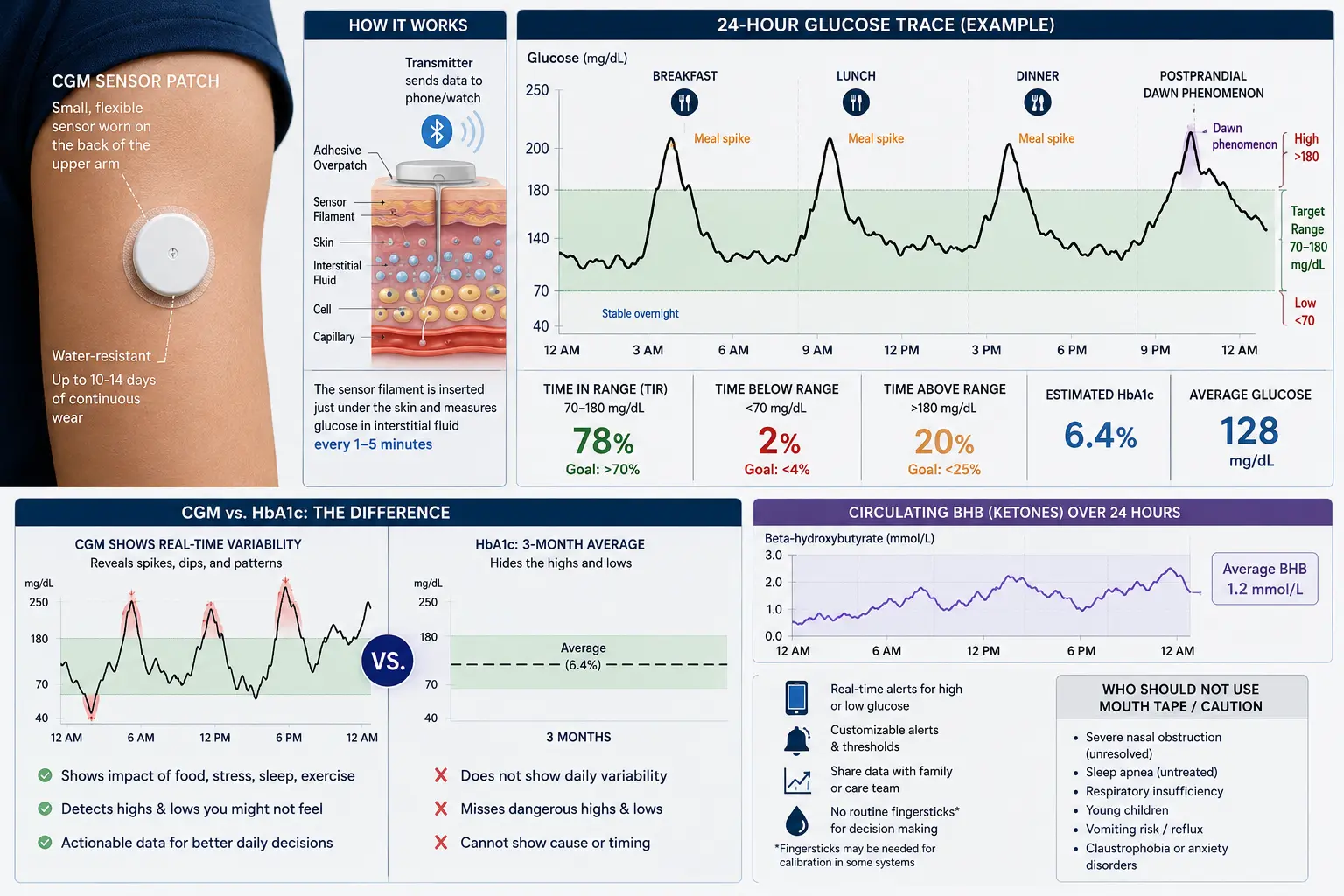
A small filament extends from the sensor through the skin into subcutaneous tissue, where it measures glucose in interstitial fluid. Because interstitial glucose lags plasma glucose by roughly 5 to 15 minutes, real-time values trail fingerstick blood glucose slightly but closely track trends. The sensor transmits via Bluetooth to a smartphone app that displays current glucose, direction of change, hours in target range, and historical patterns.
Devices and Brands
- Dexcom Stelo, G7, G6 — real-time readings, trend arrows, alerts.
- Abbott FreeStyle Libre 3, Libre Rio, Lingo — scan-or-continuous options.
- Medtronic Guardian — typically paired with insulin pumps.
- Levels and Nutrisense — software and coaching layer on top of hardware sensors, packaged for non-diabetic users.
What You Actually Learn
For a non-diabetic adult, two weeks of CGM data typically reveal:
- Post-meal glucose excursions from specific foods in your body — individual responses vary more than textbook glycemic indices suggest.
- Effect of exercise timing on glucose — a 10-minute post-meal walk often flattens spikes dramatically.
- Effect of sleep quality on morning fasting glucose and dawn-phenomenon patterns.
- Effect of stress and illness — cortisol spikes during stressful meetings often show on the CGM.
- Nocturnal patterns — unexplained overnight rises (dawn phenomenon) or drops.
- Hidden hypoglycemia — rare, but sometimes identifies reactive hypoglycemia after high-glycemic meals.
Key Metrics to Track
- Time in range (70–140 mg/dL for non-diabetics): Aim for >85% of each day.
- Post-meal peak: Aim for <140 mg/dL at 60–90 min post-meal.
- Return to baseline: Aim for return to <120 mg/dL within 2 hours.
- Fasting/morning glucose: Aim for 70–95 mg/dL.
- Glucose variability: Lower coefficient of variation = more stable metabolism.
Is a CGM Useful for Non-Diabetics?
The evidence is mixed but meaningful. CGM use often motivates real dietary behavior change — particularly reducing refined carbohydrate at specific meals — and provides feedback loops that static tests like A1C cannot. A 2–4 week trial is often sufficient to identify personal patterns; after that, benefit plateaus unless used episodically. A small but growing literature suggests early identification of pre-diabetes patterns that A1C misses. Skeptics argue CGMs over-medicalize normal glucose variability; this is a legitimate concern for anxiety-prone users.
Pitfalls and Misinterpretation
- Mild post-meal spikes are normal. Healthy adults can reach 140–160 after a high-carb meal; this does not indicate disease.
- Exercise temporarily raises glucose — the liver releases glucose for fuel. This is not alarming.
- Vitamin C, acetaminophen, and hydroxyurea can interfere with some sensor chemistries.
- First 24 hours of a new sensor are often less accurate.
- Dehydration can exaggerate readings.
Cost and Insurance
Over-the-counter CGMs cost roughly $50–90 per 14-day sensor in the U.S. Coaching-bundled services cost more monthly. Insurance coverage is standard for diagnosed diabetes and increasingly available for insulin-using type-2 diabetes and for some prediabetic patients. For short experimental self-monitoring by non-diabetic adults, a single 2-sensor trial (~4 weeks, $100-180) is typically enough to capture the insights worth acting on.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for continuous glucose monitor testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Continuous glucose monitor type 2 diabetes — PubMed literature search
- CGM time in range outcomes — PubMed literature search
- CGM non-diabetic use — PubMed literature search
- Glycemic variability cardiovascular risk — PubMed literature search
- Dexcom CGM accuracy — PubMed literature search
- FreeStyle Libre accuracy — PubMed literature search
- Postprandial glucose spikes — PubMed literature search
- CGM lifestyle intervention metabolic — PubMed literature search
- Personalized nutrition CGM Zoe — PubMed literature search
- CGM pregnancy gestational diabetes — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- Glycation & HbA1c: What That Number Actually Measures — interactive animation
- Hemoglobin A1C
- Fasting Insulin
- Insulin Resistance
- Type 2 Diabetes
- Diabetes
- Gestational Diabetes
- Fasting
- Blood Sugar
- Anxiety
- Metabolic Syndrome
- Weight Loss
- Vitamin C
- Exercise and Muscle Insulin Sensitivity
- Fasting Insulin and HOMA IR Testing
- Hypoglycemia Awareness and Prevention
- Insulin Types and Dosing Strategies
- CGM and Time in Range for Diabetes
- CGM for Non Diabetics