Alpha Lipoic Acid for Diabetic Peripheral Neuropathy
Diabetic peripheral neuropathy is the indication for which alpha lipoic acid has the strongest evidence base of any nutraceutical for any condition. It has been a licensed prescription drug for this indication in Germany under the names Thioctsäure and Tioctan since 1966. The pivotal ALADIN, SYDNEY, NATHAN, DEKAN, and ORPIL trial series — collectively the largest and longest randomized investigation of a nutritional compound for any condition — established 600 mg/day IV induction and 600 mg/day oral maintenance as the evidence-based protocol. This deep-dive walks through every pivotal trial, both intravenous and oral protocols, the five mechanisms by which ALA addresses diabetic nerve damage, and the practical patient timeline for clinical response.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- What Diabetic Peripheral Neuropathy Is
- The Five Pathways of Hyperglycemic Nerve Damage
- How ALA Addresses Each Damage Pathway
- The ALADIN Trial Series (I, II, III)
- The SYDNEY Trial Series (1 and 2)
- NATHAN 1 — The 4-Year Landmark Trial
- DEKAN and ORPIL Trials
- Meta-Analyses (Mijnhout, Han)
- IV vs Oral Protocols Compared
- Practical Patient Protocol & Timeline
- Combinations With Conventional Medications
- Patient FAQ
- Cautions Specific to Neuropathy Patients
- Key Research Papers
- Connections
- Featured Videos
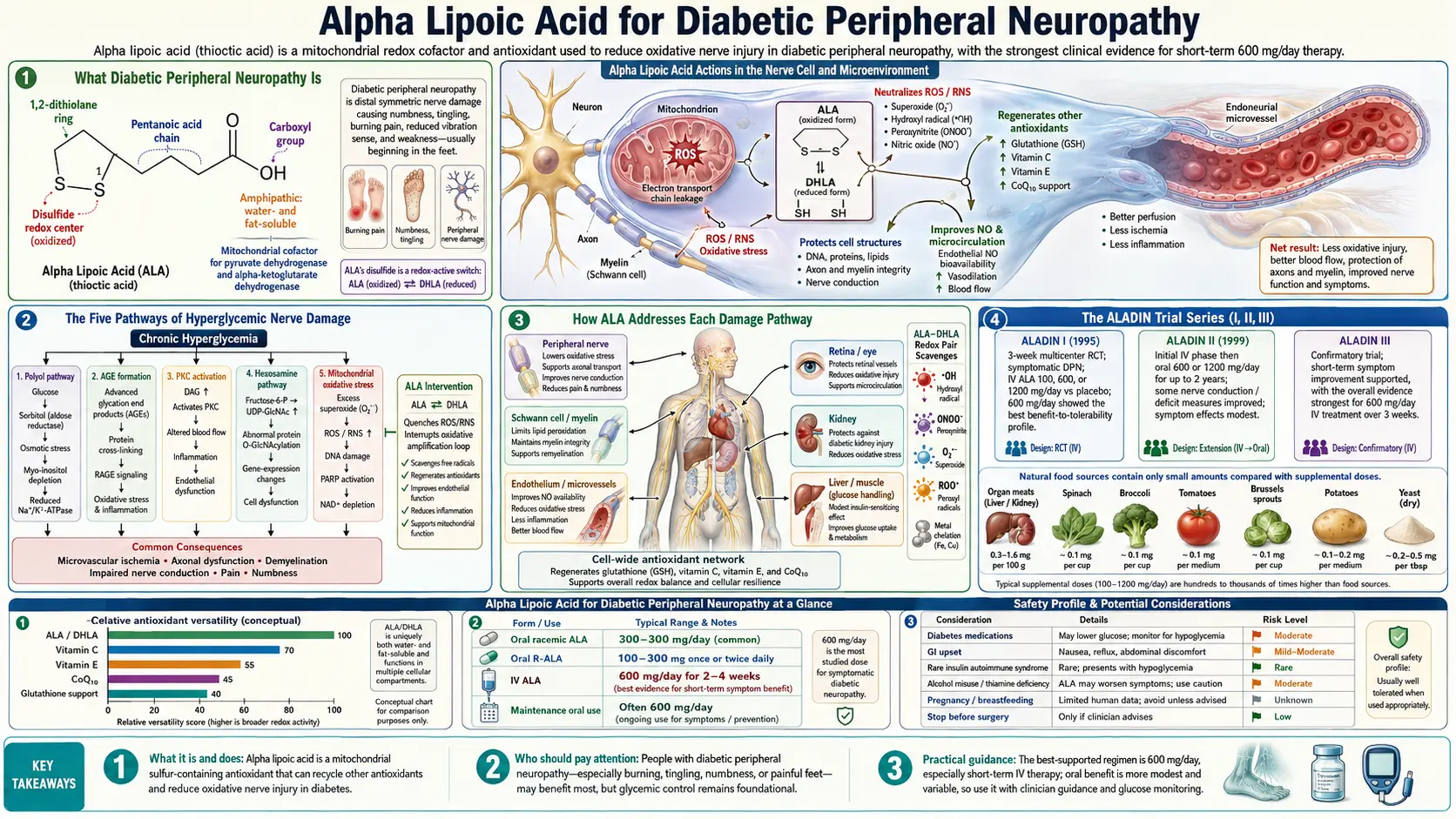
What Diabetic Peripheral Neuropathy Is
Diabetic peripheral neuropathy (DPN) is progressive damage to the sensory and motor nerves that occurs in people with long-standing diabetes — primarily type 2 but also long-duration type 1. It affects approximately 50% of patients with diabetes of 10+ years duration and is the most common cause of peripheral neuropathy worldwide.
The classic presentation is a "stocking-glove" distribution: burning, tingling, electric-shock pain, pins-and-needles, and progressive numbness, starting in the toes and feet and gradually ascending. Pain is typically worse at night and disturbs sleep. As nerve damage progresses, sensation is lost — which paradoxically becomes more dangerous than the pain because it leads to unnoticed foot injuries, ulcers, and amputations.
Conventional pharmaceutical treatment focuses on pain management rather than reversing the underlying nerve damage: gabapentin and pregabalin (calcium channel modulators), duloxetine (SNRI), tricyclic antidepressants, and topical capsaicin. These reduce pain perception but do not stop or reverse the nerve-fiber damage. Alpha lipoic acid is the only nutraceutical with substantial randomized trial evidence for actually improving nerve function and symptoms rather than just suppressing pain perception.
For the broader clinical picture of peripheral neuropathy, see our Peripheral Neuropathy page. For the place of neuropathy within the broader diabetic complication landscape (alongside retinopathy and nephropathy), see Diabetic Complications.
The Five Pathways of Hyperglycemic Nerve Damage
Chronic hyperglycemia damages peripheral nerves through five overlapping biochemical pathways. Understanding them clarifies why ALA — a single molecule — can address damage that conventional drugs (each targeting only one pathway) cannot.
- The polyol (aldose reductase) pathway — excess intracellular glucose is converted by aldose reductase to sorbitol, which accumulates in nerve cells because they lack sorbitol dehydrogenase. Sorbitol creates osmotic stress, depletes NADPH (needed for glutathione regeneration), and reduces nerve myo-inositol content critical for membrane signaling.
- Advanced glycation end-product (AGE) formation — glucose non-enzymatically attaches to proteins (including myelin and nerve cytoskeletal proteins), forming cross-linked AGE structures that disrupt nerve function and trigger inflammatory signaling through the RAGE receptor.
- Protein kinase C (PKC) activation — hyperglycemia increases diacylglycerol synthesis, activating PKC isoforms that drive vascular dysfunction, reduced nerve blood flow, and pro-inflammatory cytokine release.
- Hexosamine pathway flux — excess fructose-6-phosphate enters the hexosamine biosynthesis pathway, producing UDP-N-acetylglucosamine that modifies transcription factors and contributes to insulin resistance and inflammatory gene expression.
- Mitochondrial superoxide overproduction — hyperglycemia drives excess electron entry into the mitochondrial electron transport chain in dorsal root ganglion neurons, generating superoxide (O&sub2;−) that damages mitochondrial DNA, depolarizes the membrane potential, and triggers neuronal apoptosis. This is the proposed unifying mechanism — the superoxide surge upregulates the first four pathways.
Most conventional pharmaceutical interventions target only one of these pathways: aldose reductase inhibitors (which have failed in repeated trials due to liver toxicity), AGE breakers (the prototype alagebrium was discontinued), and PKC inhibitors (the ruboxistaurin trials were disappointing). ALA addresses all five through a combination of direct antioxidant activity (the unifying mitochondrial superoxide mechanism), aldose reductase inhibition, and reduced AGE formation.
How ALA Addresses Each Damage Pathway
- vs. polyol pathway — ALA directly inhibits aldose reductase at clinical doses, reducing sorbitol accumulation in nerve tissue. The effect is modest compared to pharmaceutical aldose reductase inhibitors but does not produce the liver toxicity that ended their clinical development.
- vs. AGE formation — ALA reduces non-enzymatic glycation through its reducing thiol structure and protects against AGE-induced inflammatory signaling. The downstream effect is reduced cross-linked protein damage in nerve tissue.
- vs. PKC activation — ALA reduces PKC activation indirectly by improving cellular redox state. The fall in oxidative signaling that normally drives PKC isoform activation is the mechanism.
- vs. hexosamine pathway — indirect; primarily through reduced flux into the pathway when ALA improves insulin sensitivity and reduces fasting hyperglycemia.
- vs. mitochondrial superoxide — the primary effect. ALA directly scavenges mitochondrial superoxide, regenerates oxidized glutathione (the principal mitochondrial antioxidant), supports glutathione peroxidase activity, and reduces electron leak through restoration of normal mitochondrial function.
Beyond the five pathways, ALA also improves intraneural blood flow. Diabetic nerve damage involves microvascular dysfunction — the small blood vessels supplying nerves develop endothelial damage, reducing nerve perfusion. ALA improves endothelial nitric oxide bioavailability and reduces oxidative damage to the nerve microvasculature, restoring blood flow to nerve fibers. This mechanism contributes to the clinical observation that ALA produces sensory and motor improvement even in long-standing neuropathy where some structural damage is presumed irreversible — the surviving fibers function better with better blood supply.
The ALADIN Trial Series (I, II, III)
ALADIN stands for "Alpha-Lipoic Acid in Diabetic Neuropathy" — a series of three pivotal trials conducted in Germany in the 1990s to satisfy European drug regulators for the prescription approval of ALA for this indication.
ALADIN I (Ziegler et al., 1995, Diabetologia)
The first trial. 328 patients with type 2 diabetes and symptomatic distal sensorimotor polyneuropathy were randomized to four arms: intravenous ALA at 100, 600, or 1200 mg/day, or placebo, given as daily infusions for 3 weeks. The primary outcome was the Total Symptom Score (TSS), a validated measure of pain, paresthesia, numbness, and burning.
Results:
- The 600 mg/day group showed a TSS reduction of 3.5 points versus 1.6 for placebo — a statistically significant and clinically meaningful difference
- The 1200 mg/day group did NOT show additional benefit over 600 mg/day, establishing the upper limit of clinical efficacy
- The 100 mg/day group showed minimal effect, establishing the lower limit
- Hamburg Pain Adjective List and Neuropathic Symptom Score also improved significantly at 600 mg/day
ALADIN I established the 600 mg/day IV dose as the standard, with the dose-response showing a clear plateau above that level. This dose has remained the IV protocol ever since.
ALADIN II (Reljanovic et al., 1999)
The 2-year oral extension trial in patients who had completed acute IV therapy. Patients received either 600 mg or 1200 mg of oral ALA daily, or placebo, for 24 months. Outcomes focused on nerve conduction velocity (NCV) measurements in the sural nerve (a sensitive marker of nerve fiber function).
Results showed sustained improvement in nerve conduction velocity in the ALA groups compared to placebo, with the 600 mg group performing equivalently to the 1200 mg group — further reinforcing the dose-plateau finding from ALADIN I. The trial established that oral maintenance therapy after IV induction produces continued nerve-function improvement over years, not just short-term symptom reduction.
ALADIN III (Ziegler et al., 1999, Diabetes Care)
509 type 2 diabetic patients with neuropathy randomized to 3 weeks of IV ALA 600 mg/day followed by 6 months of oral 1800 mg/day, versus placebo. The trial measured both the Total Symptom Score (subjective) and the Neuropathy Impairment Score (NIS — objective examination findings).
Results showed continued NIS improvement during the 6-month oral phase, particularly in lower-limb measurements. The 1800 mg/day oral dose was tolerable but did not show additional benefit over what subsequent trials would establish with 600 mg/day oral.
The SYDNEY Trial Series (1 and 2)
SYDNEY 1 (Ametov et al., 2003, Diabetes Care)
The SYDNEY trials (Symptomatic Diabetic Neuropathy) were conducted at a Moscow clinical center under international protocols. SYDNEY 1 randomized 120 patients to IV ALA 600 mg/day for 14 consecutive daily infusions versus placebo. The primary outcome was the Total Symptom Score.
Results were striking:
- TSS reduction of 5.7 points in the ALA group versus 1.8 in placebo
- 52% of ALA patients achieved >50% pain reduction (a clinically meaningful threshold) versus 18% for placebo
- Improvement was apparent within the first week of IV therapy
- Side effect profile was minimal — nausea and headache occurred in <5%, no serious adverse events
SYDNEY 1 produced the largest clear effect size in the IV ALA literature and reinforced the 14-day daily infusion as the standard induction protocol.
SYDNEY 2 (Ziegler et al., 2006, Diabetes Care)
The critical oral dose-response trial. 181 type 2 diabetic patients randomized to oral ALA 600 mg, 1200 mg, or 1800 mg/day, or placebo, for 5 weeks. The trial answered the question: what is the optimal oral dose?
Results:
- All three ALA doses produced statistically significant TSS reductions versus placebo (51%, 48%, and 52% reduction respectively, versus 32% for placebo)
- No additional benefit was seen above 600 mg/day — the three doses performed equivalently
- Higher doses were associated with somewhat more frequent gastrointestinal side effects (nausea, indigestion) but no serious adverse events
- Improvement was visible by week 2-3 and continued through week 5
SYDNEY 2 is the trial that established 600 mg/day as the optimal oral dose — the dose used in essentially all subsequent clinical practice and integrative medicine protocols. Higher doses provide no additional clinical benefit but do increase cost and GI side effects.
NATHAN 1 — The 4-Year Landmark Trial
The NATHAN 1 trial (Ziegler et al., 2011, Diabetes Care) is the longest randomized controlled trial of any nutraceutical for any condition. 460 patients with mild-to-moderate diabetic distal symmetric polyneuropathy were randomized to oral ALA 600 mg/day or placebo, and followed for 4 years. The primary outcome was the Neuropathy Impairment Score - Lower Limbs (NIS-LL), an objective neurological examination measure.
Results:
- Statistically significant improvement in NIS-LL in the ALA group versus placebo at 4 years
- The clinical effect size was modest (typical of long-term placebo-controlled trials in chronic disease) but the direction was consistent — ALA improved nerve function over 4 years while placebo patients showed gradual deterioration
- Subgroup analyses showed larger benefit in patients with better baseline glycemic control, suggesting ALA works best when added to good diabetes management rather than as a substitute for it
- Safety profile was excellent — 4 years of daily 600 mg ALA produced no significant adverse events beyond those seen with placebo
NATHAN 1 established three critical clinical points:
- Long-term oral ALA at 600 mg/day is safe and well-tolerated
- The benefit persists over years, not just weeks
- ALA is best understood as a long-term adjunct to good diabetes management, not a standalone treatment
For patients with established diabetic neuropathy, the NATHAN 1 finding means that ALA supplementation is a multi-year commitment — benefits accumulate slowly and reverse if treatment is discontinued. The clinical framing should be similar to statins or ACE inhibitors: a chronic medication taken indefinitely for ongoing protection.
DEKAN and ORPIL Trials
DEKAN (Ziegler et al., 1997)
The "Deutsche Kardiale Autonome Neuropathie" trial focused on cardiac autonomic neuropathy — a less common but more dangerous form of diabetic neuropathy that affects the heart and produces resting tachycardia, orthostatic hypotension, and silent myocardial ischemia. Cardiac autonomic neuropathy increases mortality risk substantially.
73 type 2 diabetics with documented cardiac autonomic neuropathy received oral ALA 800 mg/day or placebo for 4 months. The ALA group showed significant improvement in heart rate variability indices (the standard measure of cardiac autonomic function): reduced resting tachycardia, improved respiratory sinus arrhythmia, and improved 24-hour heart rate variability. Standard deviation of normal-to-normal R-R intervals (SDNN) improved measurably.
This established ALA as relevant for the autonomic as well as the somatic forms of diabetic neuropathy.
ORPIL Trial
The Oral Pilot Trial (smaller, ~24 patients) tested oral ALA 1800 mg/day for 3 weeks in symptomatic diabetic neuropathy. Results showed improvement on Total Symptom Score versus baseline. ORPIL was a forerunner to the larger SYDNEY 2 trial and helped establish that oral-only protocols could produce clinical benefit, not just IV induction.
Meta-Analyses (Mijnhout, Han)
Two pivotal meta-analyses pulled together the evidence base:
Mijnhout et al. (2012)
Pooled 1,160 patients from 4 of the major IV trials (ALADIN I, ALADIN III, SYDNEY 1, and one supporting trial). For IV ALA 600 mg/day for 3 weeks:
- Pooled odds ratio for >50% pain reduction: 2.96 (95% CI 1.97-4.45)
- Number needed to treat (NNT): approximately 5
- The treatment effect was robust across the included studies
The conclusion: "Treatment with alpha lipoic acid (600 mg/day intravenously) over 3 weeks is safe and significantly improves both positive neuropathic symptoms and neuropathic deficits to a clinically meaningful degree in diabetic patients with symptomatic polyneuropathy."
Han et al. (2012)
Independent meta-analysis with somewhat broader inclusion criteria, reaching similar conclusions: IV ALA produces clinically meaningful pain reduction with a favorable safety profile, and oral ALA at 600 mg/day produces similar but slower-onset benefit suitable for maintenance therapy.
Together, the two meta-analyses provide Class I evidence for ALA in diabetic peripheral neuropathy — the same evidence level required for FDA drug approval, though ALA is regulated as a dietary supplement in the US rather than as a prescription drug.
IV vs Oral Protocols Compared
| Aspect | IV (600 mg/day) | Oral (600 mg/day) |
|---|---|---|
| Time to clinical response | 1-2 weeks | 4-8 weeks |
| Magnitude of pain reduction | Larger (TSS −5.7 in SYDNEY 1) | Moderate (TSS −3.5 in SYDNEY 2) |
| Typical duration | 2-4 week induction course | Indefinite maintenance |
| Availability | Prescription in Germany; IV nutrient clinics elsewhere | Over-the-counter dietary supplement |
| Cost | $50-150 per infusion | $15-40 per month |
| Best for | Severe symptoms; rapid relief needed; treatment-refractory cases | Mild-moderate symptoms; long-term maintenance; cost-sensitive patients |
The optimal clinical strategy in expert practice is IV induction followed by indefinite oral maintenance: 600 mg IV daily for 14-21 days produces rapid symptom relief, then 600 mg/day oral indefinitely maintains the benefit and continues to address the underlying nerve damage over years (as established by NATHAN 1).
For patients without access to IV ALA, oral-only protocols also work but require more patience — expect 4-8 weeks to assess response, and 3-6 months of consistent use to reach maximum effect.
Practical Patient Protocol & Timeline
For patients with established diabetic peripheral neuropathy:
Initial trial (8 weeks)
- Dose: Racemic alpha lipoic acid 600 mg/day OR R-ALA 300 mg/day (R-form is more bioactive per milligram)
- Timing: On an empty stomach — 30 minutes before breakfast or 2 hours after the last meal of the day. Food reduces absorption by 30-50%.
- Form preference: R-ALA or Na-R-ALA (sodium R-lipoate) for better bioavailability; racemic is acceptable and substantially cheaper
- Concurrent supplementation: Add biotin 300 mcg/day (to prevent biotin depletion from chronic ALA), thiamine 50-100 mg/day (cofactor for the enzymes ALA activates)
Week-by-week timeline (oral-only protocol)
- Week 1-2: Usually no perceptible change; some patients report increased awareness of symptoms as nerve function begins to return
- Week 3-4: First subjective improvements often noticed — reduced burning, less night pain, modest improvement in sleep quality
- Week 5-8: Steady improvement; quantifiable reduction in Total Symptom Score
- Month 3-6: Plateau of clinical effect; some patients report continued slow improvement; foot sensation and balance may improve measurably
- Year 1+: Maintenance phase; benefits sustained as long as daily dosing continues
IV induction protocol (if available)
- 600 mg IV ALA in 250 mL normal saline, infused over 30-60 minutes, 5 days per week for 2-3 weeks (typically 10-15 total infusions)
- Clinical response typically apparent by infusion 5-7
- Transition to 600 mg/day oral immediately after IV course ends
- Periodic IV "boosts" (1-week courses every 6-12 months) sometimes used in patients with severe baseline disease
When to consider discontinuing
Most patients should continue ALA indefinitely once benefit is established — the NATHAN 1 trial showed that benefits accumulate over years and likely reverse on discontinuation. Reasons to consider stopping include: complete symptom resolution that persists for >6 months (uncommon), intolerable side effects, hypoglycemia issues that cannot be managed by adjusting diabetes medications, or development of new contraindications.
Combinations With Conventional Medications
- Gabapentin / pregabalin — complementary mechanisms (gabapentinoids block pain perception; ALA improves underlying nerve function). Combination is safe and synergistic. Many patients can taper gabapentinoid dose over months as ALA-driven nerve improvement reduces pain.
- Duloxetine (Cymbalta) — complementary; duloxetine's SNRI mechanism doesn't overlap with ALA. Combination is well-tolerated.
- Tricyclic antidepressants (amitriptyline, nortriptyline) — combination is safe; the chronic sedative effect of TCAs can be reduced as nerve symptoms improve with ALA, allowing dose taper.
- Capsaicin topical — complementary; topical and oral interventions don't interfere.
- Metformin — works synergistically — both activate AMPK and improve insulin sensitivity. Standard combination in integrative diabetes care.
- Insulin and sulfonylureas — caution: ALA enhances insulin sensitivity and can cause hypoglycemia. Start with lower-dose ALA (300 mg), monitor blood glucose closely for 2-4 weeks, and be prepared to reduce insulin or sulfonylurea dose.
- SGLT2 inhibitors (empagliflozin, dapagliflozin) and GLP-1 agonists (semaglutide, liraglutide) — complementary; no significant interactions.
- Benfotiamine — the fat-soluble form of thiamine (B1); pairs excellently with ALA for diabetic neuropathy. Combination is the most-studied non-pharmaceutical nerve-support stack. Typical dose: benfotiamine 300 mg + ALA 600 mg daily.
Patient FAQ
Q: How quickly will I notice improvement?
With oral ALA, expect 4-8 weeks before noticeable change. IV protocols produce faster response (1-2 weeks). Be patient — this is a long-term intervention.
Q: Does it work if my neuropathy is severe and long-standing?
Even patients with 10+ year neuropathy histories show measurable improvement on ALA. Some structural nerve damage is irreversible, but improved function of surviving fibers and improved nerve blood flow can produce real symptom relief. The Yu Ping Feng San and ALADIN trials included patients with established disease, not just early disease.
Q: Can I stop ALA once my symptoms improve?
Generally no — benefits typically reverse over weeks to months after discontinuation. ALA is a long-term commitment similar to taking statins for cholesterol or ACE inhibitors for blood pressure.
Q: Will ALA replace my gabapentin or duloxetine?
Sometimes, eventually. Many patients are able to taper or discontinue gabapentinoids and antidepressants after 6-12 months of ALA therapy with sustained symptom control. Always taper under physician supervision rather than stopping abruptly.
Q: What if my insurance doesn't cover IV ALA?
Oral-only protocols (600 mg/day racemic, or 300 mg/day R-ALA) work well, just with a slower response time. The cost difference is dramatic — IV courses cost $500-2000 total; a year of oral ALA costs $180-480.
Q: Are there any side effects?
Most patients tolerate ALA well. Common minor effects: nausea or indigestion (usually resolves with food), mild headache during first 1-2 weeks, hypoglycemia (if on insulin or sulfonylureas — monitor closely). Rare effects: skin rash, sulfurous breath odor.
Q: Can I take it forever?
Yes — the NATHAN 1 trial established 4 years of daily 600 mg ALA as safe and effective with no cumulative toxicity. Add a biotin supplement (300-500 mcg/day) to prevent biotin depletion during chronic ALA use.
Cautions Specific to Neuropathy Patients
- Hypoglycemia is the most important risk — diabetic neuropathy patients are typically on glucose-lowering medications. Adding ALA enhances insulin sensitivity and can drop blood glucose. Monitor closely for 2-4 weeks after starting; be prepared to reduce insulin or sulfonylurea dose by 10-25%.
- Foot care still required — even with ALA-driven sensory improvement, diabetic foot care remains essential. Sensation may not fully return, and the foot remains at risk for unnoticed injuries, ulcers, and infections. Daily foot inspection, proper footwear, and regular podiatry visits are not optional.
- Glycemic control remains primary — ALA is an adjunct, not a substitute for good diabetes management. NATHAN 1 showed that ALA worked best in patients with HbA1c under 8%. Optimize your HbA1c through diet, exercise, and medication adherence first; add ALA on top of that foundation.
- Insulin Autoimmune Syndrome (IAS / Hirata's disease) — rare but documented in patients of East Asian descent carrying HLA-DRB1*04:06. Presents as severe spontaneous hypoglycemia from autoantibodies against insulin. Discontinue ALA if unexplained hypoglycemia develops.
- Biotin co-supplementation — long-term ALA (>6 months at 600 mg+) can deplete biotin through competitive cellular uptake. Add 300-500 mcg biotin daily.
- Thiamine adequacy — the mitochondrial enzymes ALA activates require thiamine pyrophosphate. Chronic alcoholics and patients with malabsorption should ensure adequate thiamine status before high-dose ALA.
Key Research Papers
- Ziegler D et al. (1995). Treatment of symptomatic diabetic peripheral neuropathy with the antioxidant alpha-lipoic acid: a 3-week multicentre randomized controlled trial (ALADIN Study). Diabetologia. — PubMed
- Reljanovic M et al. (1999). Treatment of diabetic polyneuropathy with the antioxidant thioctic acid (alpha-lipoic acid): a two year multicenter randomized double-blind placebo-controlled trial (ALADIN II). Free Radical Research. — PubMed
- Ziegler D et al. (1999). Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a 7-month multicenter randomized controlled trial (ALADIN III Study). Diabetes Care. — PubMed
- Ametov AS et al. (2003). The sensory symptoms of diabetic polyneuropathy are improved with alpha-lipoic acid: the SYDNEY trial. Diabetes Care. — PubMed
- Ziegler D et al. (2006). Oral treatment with alpha-lipoic acid improves symptomatic diabetic polyneuropathy: the SYDNEY 2 trial. Diabetes Care. — PubMed
- Ziegler D et al. (2011). Efficacy and safety of antioxidant treatment with alpha-lipoic acid over 4 years in diabetic polyneuropathy: the NATHAN 1 trial. Diabetes Care. — PubMed
- Ziegler D et al. (1997). Effects of treatment with the antioxidant alpha-lipoic acid on cardiac autonomic neuropathy in NIDDM patients: the DEKAN study. Diabetes Care. — PubMed
- Mijnhout GS et al. (2012). Alpha lipoic acid for symptomatic peripheral neuropathy in patients with diabetes: a meta-analysis of randomized controlled trials. International Journal of Endocrinology. — PubMed
- Han T et al. (2012). A systematic review and meta-analysis of alpha-lipoic acid in the treatment of diabetic peripheral neuropathy. European Journal of Endocrinology. — PubMed
- Vallianou N et al. (2009). Alpha-lipoic acid and diabetic neuropathy. Review in Diabetic Studies. — PubMed
PubMed Topic Searches
- PubMed: alpha lipoic acid diabetic neuropathy
- PubMed: ALA aldose reductase polyol pathway
- PubMed: ALA nerve conduction velocity
- PubMed: ALA + benfotiamine combination
- PubMed: ALA intraneural blood flow
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- Alpha Lipoic Acid Overview
- ALA Benefits Hub
- ALA for Mitochondria
- ALA for Blood Sugar
- ALA for Neuroprotection
- Peripheral Neuropathy
- Diabetic Complications
- Diabetes
- Hemoglobin A1c
- Fasting Insulin
- Vitamin B1 (Thiamine / Benfotiamine)
- Vitamin B7 (Biotin)
- Vitamin B12
- Numbness & Tingling
- Chronic Pain
- All Antioxidants
- Oxidative Stress