Alpha Lipoic Acid for Blood Sugar & Insulin Sensitivity
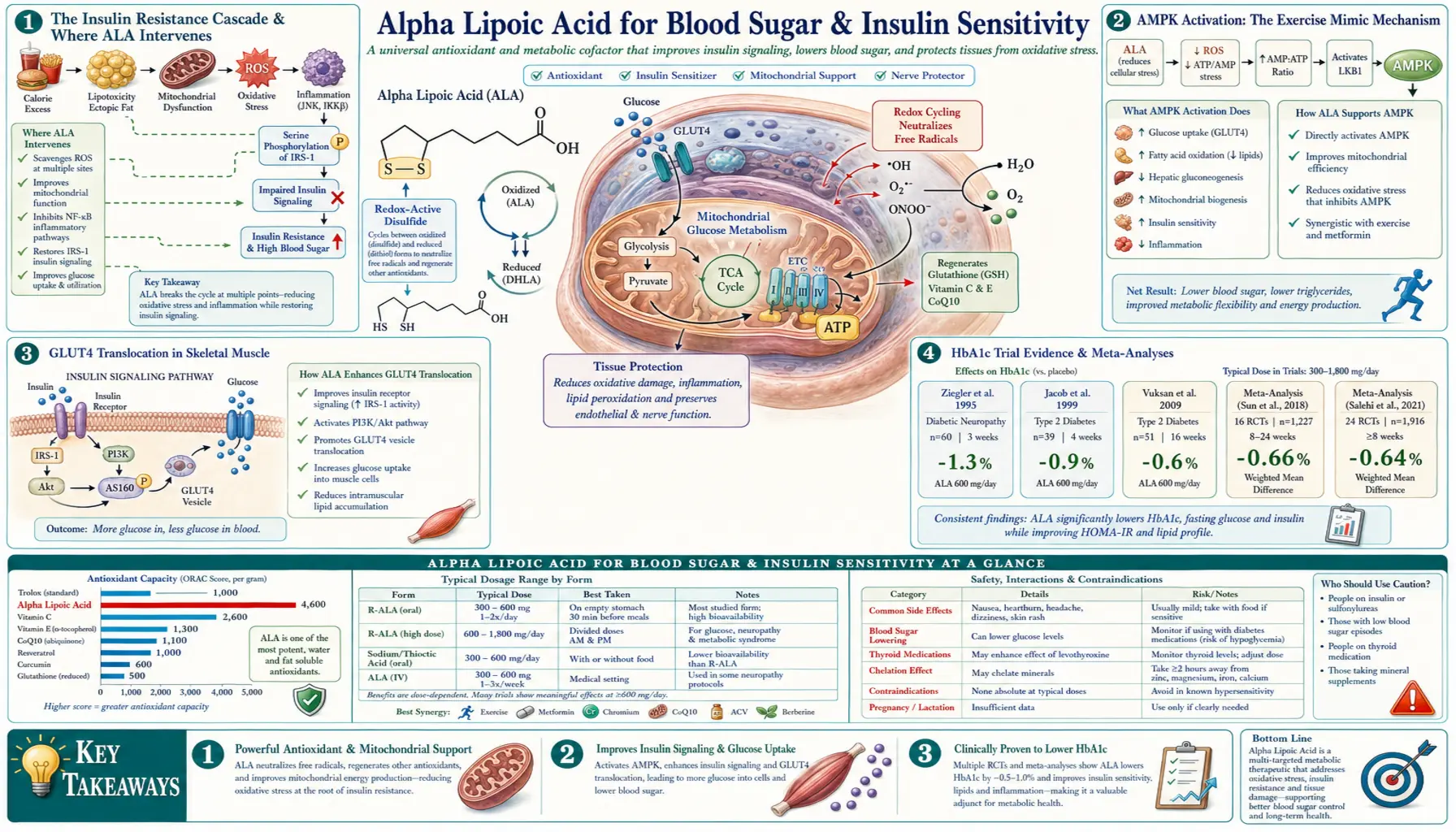
Alpha lipoic acid improves whole-body insulin sensitivity through AMP-activated protein kinase (AMPK) activation in skeletal muscle — the same metabolic signal exercise produces. The downstream effects include GLUT4 glucose transporter translocation to the muscle cell membrane, reduced inflammatory oxidative stress that drives insulin receptor desensitization, and reduced hepatic glucose output. Meta-analyses of oral ALA trials in type 2 diabetes show consistent HbA1c reductions of 0.3-0.5 percentage points at 300-600 mg/day, with larger effects in patients with worse baseline control. ALA paired with berberine and chromium forms the most evidence-supported nutraceutical stack for insulin resistance and metabolic syndrome.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- The Insulin Resistance Cascade & Where ALA Intervenes
- AMPK Activation: The Exercise Mimic Mechanism
- GLUT4 Translocation in Skeletal Muscle
- HbA1c Trial Evidence & Meta-Analyses
- Trials in Prediabetes & Metabolic Syndrome
- Stacking with Berberine, Chromium, Metformin
- Dosing Strategy for Different Glycemic States
- The Hypoglycemia Caution (Insulin, Sulfonylureas)
- Insulin Autoimmune Syndrome (Hirata's Disease)
- CGM Monitoring When Starting ALA
- Key Research Papers
- Connections
- Featured Videos
The Insulin Resistance Cascade & Where ALA Intervenes
Insulin resistance is the foundation of type 2 diabetes, metabolic syndrome, NAFLD, PCOS, and many features of cardiovascular disease. It develops gradually through a cascade of cellular changes:
- Adipose tissue inflammation — excess caloric intake expands adipocytes, eventually triggering macrophage infiltration and chronic low-grade inflammation that releases TNFα, IL-6, and other inflammatory cytokines into circulation
- Hepatic insulin resistance — inflammatory cytokines impair hepatic insulin signaling, leading to excess gluconeogenesis and elevated fasting glucose
- Skeletal muscle insulin resistance — inflammatory cytokines impair muscle insulin signaling, reducing post-meal glucose uptake; intramyocellular lipid accumulation further impairs insulin sensitivity
- Pancreatic compensation, then failure — the pancreas initially produces more insulin to overcome the resistance; eventually beta-cell function declines and frank diabetes develops
ALA intervenes at multiple points in this cascade:
- At the adipose inflammation level — reduces oxidative stress and inflammatory cytokine production
- At the skeletal muscle level — directly activates AMPK and triggers GLUT4 translocation, increasing glucose uptake independently of insulin signaling (more on this below)
- At the hepatic level — reduces oxidative stress in hepatocytes; some evidence for reduced hepatic gluconeogenesis
- At the pancreatic level — protects beta cells from oxidative damage (less directly studied)
The most important and best-characterized mechanism is the AMPK / GLUT4 pathway in skeletal muscle — the same pathway through which exercise and metformin work.
AMPK Activation: The Exercise Mimic Mechanism
AMP-activated protein kinase (AMPK) is a cellular energy sensor. When ATP is consumed faster than it can be regenerated (during exercise, fasting, or cellular stress), the AMP:ATP ratio rises and activates AMPK. AMPK then signals the cell to switch from anabolic (energy-storing) to catabolic (energy-producing) metabolism:
- Increased glucose uptake — AMPK triggers translocation of GLUT4 glucose transporters from intracellular vesicles to the plasma membrane, allowing more glucose entry from the bloodstream
- Increased fatty acid oxidation — AMPK phosphorylates acetyl-CoA carboxylase, reducing malonyl-CoA levels, which removes the brake on carnitine palmitoyltransferase 1 (CPT1) and allows fatty acid entry into mitochondria
- Decreased gluconeogenesis — AMPK reduces hepatic glucose output
- Decreased lipogenesis — AMPK shuts down fatty acid synthesis
- Increased mitochondrial biogenesis — AMPK activates PGC-1α over longer time scales
Exercise, fasting, metformin, berberine, and resveratrol all activate AMPK through different upstream signals. Alpha lipoic acid joins this list — it activates AMPK in skeletal muscle and adipose tissue, mimicking the metabolic effects of moderate exercise on a cellular level. This is why ALA improves insulin sensitivity even in sedentary individuals: the cell receives an exercise-like signal regardless of whether the body is actually moving.
The mechanism by which ALA activates AMPK is incompletely characterized but appears to involve reduction of cellular oxidative stress (which itself can inhibit AMPK) combined with direct effects on the upstream kinases LKB1 and CaMKK2 that normally activate AMPK.
GLUT4 Translocation in Skeletal Muscle
Skeletal muscle is responsible for approximately 80% of insulin-mediated whole-body glucose disposal after meals. Glucose enters muscle cells through the GLUT4 transporter, which is normally stored in intracellular vesicles and translocated to the cell membrane in response to insulin or exercise. In insulin-resistant individuals, this translocation is impaired — insulin signaling fails to mobilize GLUT4 efficiently, leaving cells "hungry" for glucose despite high blood levels.
ALA stimulates GLUT4 translocation through two mechanisms:
- Insulin-dependent pathway — ALA improves insulin signaling by reducing the oxidative damage to insulin receptor substrate (IRS-1) and PI3-kinase that contributes to insulin resistance
- Insulin-independent pathway — ALA-activated AMPK triggers GLUT4 translocation directly, bypassing the insulin signaling cascade entirely. This is why ALA improves glucose disposal even in patients with severe insulin resistance where insulin signaling is profoundly impaired.
The insulin-independent mechanism is particularly clinically valuable because it parallels how exercise works — exercise-induced glucose uptake is independent of insulin status and can occur normally even in advanced diabetes. ALA effectively gives the cell some of this exercise-like glucose uptake capacity at rest.
Quantitatively, the effect is meaningful but modest — published trials show ALA improves muscle glucose disposal by approximately 15-25% on hyperinsulinemic-euglycemic clamp testing in type 2 diabetics. For comparison, metformin produces 20-30% improvement; exercise produces 50-100% improvement during the active session.
HbA1c Trial Evidence & Meta-Analyses
Multiple randomized trials and meta-analyses have evaluated ALA's effect on glycemic control in type 2 diabetes:
The Akbari et al. (2018) meta-analysis
Pooled 25 trials with over 1,200 patients. Findings:
- Average HbA1c reduction: 0.35 percentage points on 300-1800 mg/day ALA over 8-26 weeks
- Fasting blood glucose reduction: ~13 mg/dL on average
- Effects were dose-related but plateaued above 600 mg/day
- Larger effects in patients with worse baseline HbA1c (above 8%)
- Smaller effects in well-controlled diabetics (HbA1c under 7%)
- No effect in non-diabetic patients on fasting glucose
The Mohammadi et al. (2022) meta-analysis
More recent pooling of trials specifically in type 2 diabetes, confirming the Akbari findings and adding analyses of HOMA-IR (insulin resistance index): significant HOMA-IR improvement of ~1.5 points in patients with baseline HOMA-IR > 3.
Clinical interpretation
A 0.35 percentage point HbA1c reduction is modest in absolute terms — metformin produces ~1.0 point reduction, GLP-1 agonists produce ~1.0-1.5 points. ALA is therefore appropriately positioned as an adjunct to pharmacological therapy rather than as a substitute. The clinical use cases where ALA contributes meaningful value:
- Adding to metformin in patients who need a small additional HbA1c reduction (e.g., 7.5 to 7.0)
- Pre-diabetes prevention protocols where lifestyle change alone is insufficient
- Patients with both insulin resistance AND another ALA-responsive indication (diabetic neuropathy, oxidative stress, fatigue) — getting multiple benefits from one supplement
- Patients who cannot tolerate or refuse metformin and want a nutraceutical alternative (though metformin is the better choice when tolerated)
ALA should NOT be presented as a substitute for proven diabetes medications. It is a useful adjunct, particularly when paired with other AMPK-activating interventions.
Trials in Prediabetes & Metabolic Syndrome
Several small trials have tested ALA in prediabetes and metabolic syndrome — conditions where insulin resistance is established but frank diabetes has not yet developed:
- Insulin sensitivity (Manning trials) — 8 weeks of 600 mg/day ALA improved insulin-mediated glucose disposal by ~17% in obese patients with impaired glucose tolerance
- HOMA-IR reduction — multiple small trials show 1-2 point HOMA-IR improvement after 8-12 weeks of 600 mg/day in metabolic syndrome patients
- Weight loss adjunct — modest weight loss (~2 kg over 12 weeks) has been reported in some trials when ALA is added to caloric restriction, possibly through AMPK-driven fatty acid oxidation
- Triglyceride reduction — ALA modestly reduces fasting triglycerides in metabolic syndrome (typically 15-25 mg/dL reduction)
The trial evidence in metabolic syndrome is less robust than in established type 2 diabetes — smaller sample sizes, shorter duration, less consistent outcomes. The mechanistic case is strong but the clinical evidence does not yet support strong recommendation for ALA as a primary prediabetes intervention. Lifestyle change (diet quality, exercise, sleep, stress management) remains the first-line approach; ALA may add modest incremental benefit when used alongside lifestyle measures.
Stacking with Berberine, Chromium, Metformin
ALA combines well with several other glucose-lowering interventions through complementary mechanisms:
ALA + Berberine
Berberine is the most powerful nutraceutical glucose-lowering agent — multiple meta-analyses show HbA1c reductions of 0.8-1.0 points, comparable to metformin. Berberine activates AMPK through a different upstream mechanism than ALA (LKB1 activation via mitochondrial Complex I inhibition). The combination produces additive effects on AMPK activation and glucose disposal. Typical dose: ALA 600 mg + berberine 500 mg, both 2-3 times daily with meals.
Caution: The combination can produce more substantial hypoglycemia in patients on insulin or sulfonylureas. Start low (300 mg each) and titrate up over 2-4 weeks.
ALA + Chromium
Chromium picolinate (200-1000 mcg/day) modestly improves insulin sensitivity through enhanced insulin receptor signaling and chromodulin activation. Effect size is small but additive with ALA. Useful in patients with documented or suspected chromium deficiency (often associated with poor diet quality, recent illness, or high carbohydrate intake).
ALA + Metformin
Metformin is the cornerstone of pharmacological diabetes therapy. ALA pairs well with metformin — both activate AMPK through different mechanisms, producing additive effects without dose-limiting interactions. The combination is the standard approach in integrative diabetes care for patients requiring more glycemic control than metformin alone provides.
ALA + Cinnamon
Cinnamon (Ceylon cinnamon preferred over Cassia for safety) provides modest glucose-lowering effects through enhanced insulin receptor signaling. Useful as a culinary integration with ALA supplementation.
The "metabolic syndrome stack"
The full integrative-medicine stack for metabolic syndrome typically includes:
- ALA 600 mg twice daily
- Berberine 500 mg three times daily
- Chromium 200-400 mcg/day
- Magnesium glycinate 200-400 mg/day (insulin signaling cofactor)
- Vitamin D3 2000-4000 IU/day if 25(OH)D is below 40 ng/mL
- CoQ10 100 mg/day (mitochondrial support)
Dosing Strategy for Different Glycemic States
- Prediabetes / metabolic syndrome (HbA1c 5.7-6.4%): 300-600 mg/day racemic ALA, on empty stomach, often combined with lifestyle intervention. Reassess HbA1c at 3 months.
- Type 2 diabetes, metformin alone, HbA1c 7.0-8.5%: 600 mg/day ALA added to metformin. Consider adding berberine if HbA1c remains above target after 3 months on the combination.
- Type 2 diabetes on insulin or sulfonylureas: Start at 300 mg/day, monitor blood glucose closely, titrate to 600 mg/day over 2-4 weeks. Be prepared to reduce insulin/sulfonylurea dose by 10-25% as ALA enhances insulin sensitivity.
- Diabetic neuropathy patient regardless of glycemic state: 600 mg/day ALA for neuropathy benefits; blood sugar effects are a bonus.
- Combined metabolic syndrome + insulin resistance + fatigue: ALA 600 mg + acetyl-L-carnitine 1 g, twice daily; expect 8-12 weeks for full effect.
- R-ALA users: Use approximately half the racemic dose (e.g., 300 mg R-ALA = 600 mg racemic equivalent).
Timing. Take on an empty stomach — 30 minutes before a meal or 2 hours after. Food reduces absorption by 30-50%. For twice-daily dosing, take before breakfast and before lunch (avoid evening dosing to prevent mild stimulation).
The Hypoglycemia Caution (Insulin, Sulfonylureas)
ALA enhances insulin sensitivity and stimulates non-insulin-mediated glucose uptake. The clinical consequence is that blood glucose can drop significantly when ALA is added to existing diabetes medications. The risk is highest with:
- Insulin (any type) — expect to reduce total daily dose by 10-25% over the first 2-4 weeks of ALA therapy
- Sulfonylureas (glipizide, glyburide, glimepiride) — sulfonylureas cause insulin release independent of blood glucose, so the combination can produce dangerous hypoglycemia. Consider switching to a non-sulfonylurea agent.
- Glinides (repaglinide, nateglinide) — similar risk profile to sulfonylureas
- Combination therapies including the above
Lower hypoglycemia risk with:
- Metformin alone — metformin does not cause hypoglycemia by itself; ALA + metformin is safe without dose adjustment
- DPP-4 inhibitors (sitagliptin, etc.) — minimal hypoglycemia risk
- SGLT2 inhibitors (empagliflozin, dapagliflozin) — minimal hypoglycemia risk
- GLP-1 agonists (semaglutide, liraglutide, tirzepatide) — minimal hypoglycemia risk on monotherapy
Monitoring protocol when starting ALA on insulin or sulfonylureas:
- Check blood glucose before each meal and at bedtime for the first 2 weeks
- Reduce insulin or sulfonylurea dose by 10% if any reading is below 80 mg/dL
- Reduce by 25% if any reading is below 60 mg/dL
- Coordinate with prescribing physician for systematic dose adjustments
The hypoglycemia risk should not deter ALA use in diabetic patients — it is a manageable side effect that resolves with appropriate medication adjustment. But it requires active monitoring and physician coordination during the introduction period.
Insulin Autoimmune Syndrome (Hirata's Disease)
A rare but serious adverse effect of ALA has been reported almost exclusively in patients of East Asian descent: Insulin Autoimmune Syndrome (IAS), also called Hirata's disease after the Japanese physician who first characterized it in 1970.
IAS presents as severe spontaneous hypoglycemia — sometimes profound, with blood glucose below 40 mg/dL — caused by autoantibodies against endogenous insulin. The autoantibodies bind insulin, releasing it inappropriately during fasting and causing reactive hypoglycemia.
The condition is strongly associated with the HLA-DRB1*04:06 allele, which has high prevalence in Japanese, Korean, and Chinese populations (10-30% allele frequency in some Asian populations) and is rare in European or African descent populations (less than 1%). The allele creates a genetic susceptibility that is triggered by certain drugs and compounds including ALA, methimazole, captopril, hydralazine, and several others.
The mechanism appears to involve ALA-mediated cleavage of insulin disulfide bonds, exposing previously hidden epitopes that the immune system recognizes as foreign. The autoantibody response can be self-sustaining once triggered.
Clinical implications
- Patients of Japanese, Korean, or Chinese descent considering ALA supplementation should be aware of this risk
- Symptoms to watch for: spontaneous hypoglycemia, particularly in fasting state; symptoms of low blood sugar without an obvious cause
- If hypoglycemia develops, discontinue ALA immediately and seek medical evaluation
- Diagnostic workup: anti-insulin antibody titers, HLA-DRB1 typing
- Treatment: discontinue offending agent; symptoms typically resolve over weeks to months as antibody titers fall
- For European or African descent populations, IAS is extremely rare and not a meaningful concern
CGM Monitoring When Starting ALA
Continuous glucose monitoring (CGM) systems — Dexcom G7, Freestyle Libre 3, Stelo, etc. — are now widely available without prescription in the US and provide an excellent tool for monitoring the glucose effects of ALA introduction. For patients on insulin or sulfonylureas, a 14-day CGM trial when starting ALA is highly recommended.
What CGM data shows during ALA introduction:
- Reduced post-meal glucose excursions — usually visible within 1-2 weeks
- Lower overnight average glucose — visible as flatter overnight tracing
- Possible mild reactive hypoglycemia 2-4 hours after meals in some patients — particularly those on insulin
- Higher time-in-range — the key clinical metric, typically improving from baseline by 5-15 percentage points over 4-8 weeks
See our CGM page for details on interpretation and the time-in-range metric.
Key Research Papers
- Akbari M et al. (2018). The effects of alpha-lipoic acid supplementation on glucose control and lipid profiles among patients with metabolic diseases: a systematic review and meta-analysis of randomized controlled trials. Metabolism. — PubMed
- Mohammadi V et al. (2022). The effect of alpha-lipoic acid on glycemic indices and insulin resistance in type 2 diabetes: meta-analysis. — PubMed
- Jacob S et al. (1999). Oral administration of RAC-alpha-lipoic acid modulates insulin sensitivity in patients with type-2 diabetes mellitus. Free Radic Biol Med. — PubMed
- Konrad T et al. (1999). Alpha-lipoic acid treatment decreases serum lactate and pyruvate concentrations and improves glucose effectiveness in lean and obese patients with type 2 diabetes. Diabetes Care. — PubMed
- Lee WJ et al. (2005). Alpha-lipoic acid increases insulin sensitivity by activating AMPK in skeletal muscle. Biochem Biophys Res Commun. — PubMed
- ALA + berberine combination metabolic syndrome — PubMed
- Insulin Autoimmune Syndrome and alpha lipoic acid — PubMed
- ALA polycystic ovary syndrome (PCOS) insulin resistance trials — PubMed
- ALA non-alcoholic fatty liver disease (NAFLD) trials — PubMed
- ALA gestational diabetes — PubMed
PubMed Topic Searches
- PubMed: ALA HbA1c
- PubMed: ALA insulin sensitivity
- PubMed: ALA AMPK activation
- PubMed: ALA GLUT4 translocation
- PubMed: ALA + metformin combination
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- Alpha Lipoic Acid Overview
- ALA Benefits Hub
- ALA for Neuropathy
- ALA for Mitochondria
- ALA for Neuroprotection
- Diabetes
- Diabetes Remission
- HbA1c
- Fasting Insulin
- Continuous Glucose Monitor
- Berberine
- Cinnamon
- Gymnema
- Magnesium Glycinate
- Chromium
- Vitamin D3
- CoQ10
- Blood Sugar (General)
- Anti-Inflammatory Diet