Glutamine for Immune Function
Glutamine is the dominant metabolic fuel for the rapidly dividing cells of the immune system — lymphocytes, neutrophils, and macrophages all consume glutamine at rates that meet or exceed their glucose consumption. Eric Newsholme, the Oxford biochemist who first measured this in the early 1980s, framed it as a question of substrate availability: "Why is L-glutamine metabolism important to cells of the immune system in health, postinjury, surgery or infection?" His answer, refined by three decades of follow-up work, is that the immune system shares with the gut and rapidly dividing tumor cells an absolute substrate preference for glutamine over glucose. Under conditions of catabolic stress — trauma, sepsis, severe burns, major surgery, the post-exercise "open window" in athletes — plasma glutamine can fall below the threshold at which immune cells can no longer mount an effective response, and the result is a documented increase in infection-related morbidity and mortality. This deep-dive walks through the cell-biology mechanisms, the pivotal Wischmeyer burn and ICU trials, the REDOXS controversy, and the practical clinical applications.
Table of Contents
- Glutamine as Fuel for Immune Cells
- The Conditionally Essential Framework (Lacey & Wilmore 1990)
- Enterocytes, Mucosal IgA, and the Gut-Immune Interface
- Burns, Trauma, and Sepsis: The Wischmeyer Trials
- The REDOXS Controversy
- Major Surgery and Bone Marrow Transplant
- The Post-Exercise "Open Window" of Immune Vulnerability
- Chronic Infection Recovery and HIV
- Dosing, Routes, and Alanyl-Glutamine Dipeptide
- Cautions (Including the REDOXS-Era Caveats)
- Key Research Papers
- Connections
- Featured Videos
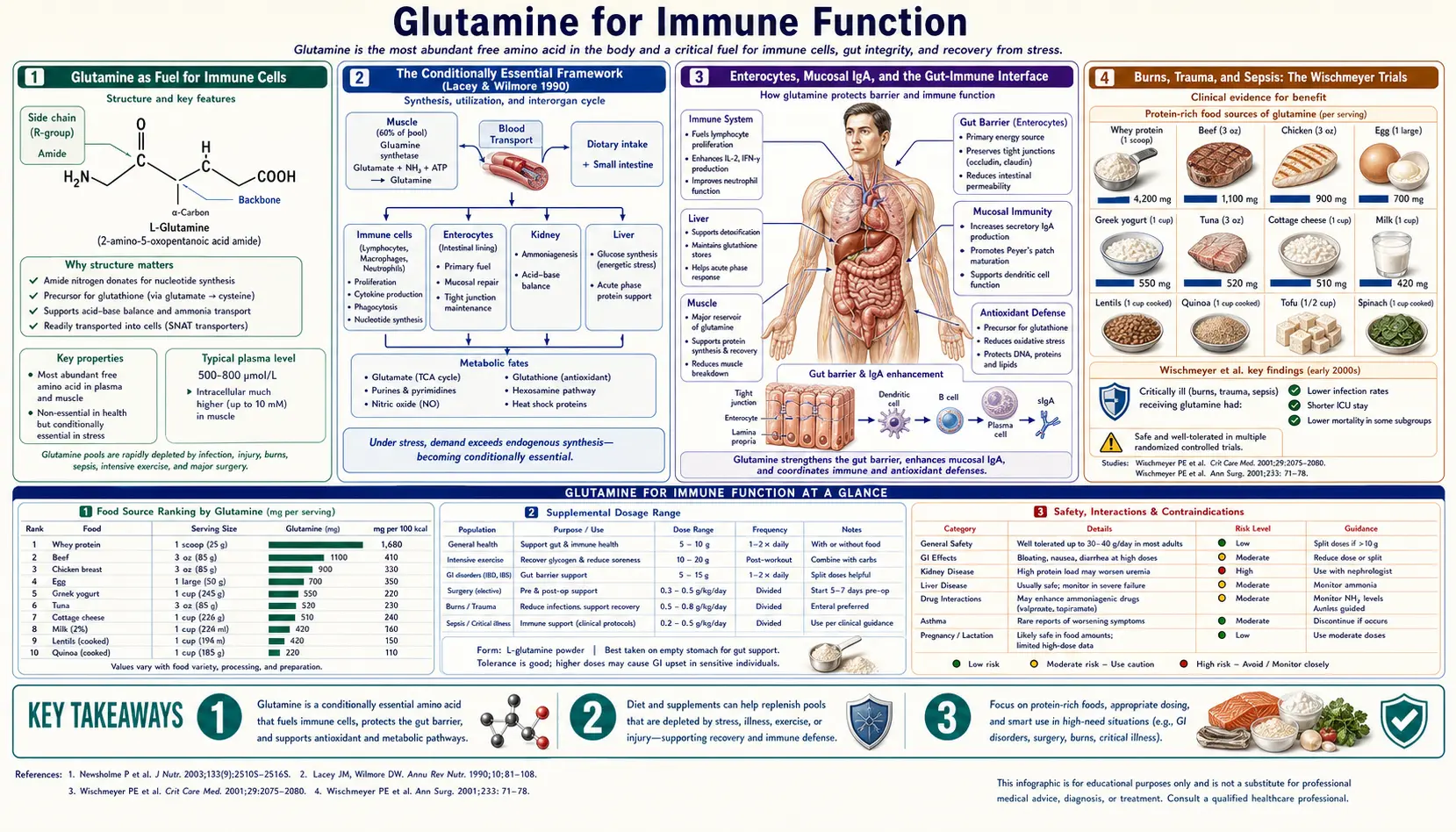
Glutamine as Fuel for Immune Cells
Resting lymphocytes consume glutamine at roughly the same rate as glucose. Activated lymphocytes — cells that have encountered antigen and are clonally expanding to mount a response — consume glutamine at rates that meet or exceed glucose utilization. The same is true for neutrophils (the front-line phagocytes of acute bacterial infection) and macrophages (which carry out both antigen presentation and tissue clean-up). Ardawi and Newsholme's 1983 paper in the Biochemical Journal on glutamine metabolism in rat lymphocytes was the foundational measurement that established this dependency.
The biochemistry is straightforward: glutamine enters the cell, is deaminated to glutamate by glutaminase, and then enters the TCA cycle as alpha-ketoglutarate — a process called glutaminolysis. This generates ATP, but more importantly, it generates carbon skeletons for nucleotide biosynthesis (essential for DNA replication during cell division) and nitrogen for purine and pyrimidine synthesis. A lymphocyte that has just recognized antigen and is about to divide every 6-12 hours for several days needs nucleotides, and glutamine is the principal source.
This is the reason that under catabolic stress — major surgery, severe burns, sepsis, prolonged endurance exercise — the body breaks down skeletal muscle protein specifically to liberate glutamine for the immune system. Skeletal muscle stores roughly 70-80% of the body's free amino acid pool, and glutamine accounts for roughly 60% of that intramuscular pool. The muscle wasting visible in chronically ill or septic patients is in significant part a glutamine-redistribution phenomenon: muscle protein is being cannibalized to keep the gut and immune system alive.
The Conditionally Essential Framework (Lacey & Wilmore 1990)
The phrase "conditionally essential amino acid" was coined by Joanne Lacey and Douglas Wilmore in a 1990 Nutrition Reviews paper that became the conceptual foundation for the modern field of immunonutrition. Their argument: glutamine is non-essential under ordinary conditions because healthy adults synthesize it in adequate quantities. But under specific clinical conditions — major trauma, severe burns, sepsis, the metabolic stress of intensive care — endogenous synthesis cannot keep up with demand, plasma glutamine falls, and at some threshold the deficit becomes clinically significant. In those settings, glutamine must be supplied from outside the body and is functionally essential.
The Lacey-Wilmore framework set off a 30-year research program to map exactly which catabolic stress states reliably deplete plasma glutamine, what threshold of depletion correlates with clinical harm, and which patient populations benefit most from supplementation. The classical observation from intensive care medicine is that plasma glutamine below approximately 420 µmol/L on ICU admission predicts increased mortality, independent of other markers of severity — making it one of the few amino acid measurements with prognostic value at the bedside.
Enterocytes, Mucosal IgA, and the Gut-Immune Interface
Roughly 70% of the body's immune tissue resides in the gut-associated lymphoid tissue (GALT), and the integrity of the gut barrier is itself a major component of immune defense. Glutamine's role here is dual: it fuels the enterocytes that make up the physical barrier (covered in detail in the companion Gut Health & Leaky Gut deep dive), and it supports the secretory IgA production that constitutes the chemical layer of mucosal immunity.
Studies of critically ill patients on parenteral nutrition without glutamine supplementation have shown progressive villous atrophy, decreased mucosal IgA, and increased bacterial translocation across the gut wall — the classical "gut-origin sepsis" of intensive care. The Van der Hulst 1993 Lancet trial demonstrated that adding glutamine to TPN preserved gut barrier function and reduced bacterial translocation, a finding that helped drive the routine addition of glutamine dipeptide to modern parenteral nutrition formulations.
In ambulatory populations, the connection between gut barrier and systemic immunity is less dramatic but still measurable. Athletes engaged in prolonged endurance training transiently develop increased intestinal permeability, and the subsequent translocation of endotoxin into systemic circulation is one of the mechanisms behind the well-documented post-exercise immune dip discussed below.
Burns, Trauma, and Sepsis: The Wischmeyer Trials
The clinical setting where the case for glutamine supplementation is strongest is severe burn injury. Severely burned patients lose plasma glutamine within hours of the burn (the burn wound itself is metabolically active and consumes large quantities of glutamine), and the resulting deficit correlates with infectious complications, sepsis, and mortality. Paul Wischmeyer's research program at the University of Chicago and later Duke established that enteral or parenteral glutamine supplementation in burn patients:
- Reduced gram-negative bacteremia (Wischmeyer 2001, Critical Care Medicine)
- Reduced overall infectious morbidity and improved mortality (Garrel 2003, Critical Care Medicine)
- Restored plasma glutamine to physiologic ranges within 24-48 hours of starting supplementation
- Was well-tolerated even at the high doses (0.3-0.5 g/kg/day) used in these trials
The Garrel trial in particular was a milestone: adult burn patients given enteral glutamine had a roughly 25% reduction in mortality compared to a similar control population, a magnitude of effect that few other nutritional interventions match in any setting. The American Burn Association and the Society of Critical Care Medicine subsequently incorporated glutamine supplementation into guidelines for severe burn management.
Beyond burns, glutamine has been studied in major trauma, post-surgical patients, and septic shock. The Novak 2002 meta-analysis in Critical Care Medicine pooled the earlier trial data and concluded that glutamine supplementation reduced infectious complications and length of stay in critically ill patients, particularly in surgical and trauma populations.
The REDOXS Controversy
In 2013, Daren Heyland and colleagues published the REDOXS trial in the New England Journal of Medicine: a multi-center randomized trial of 1,223 critically ill ICU patients with multi-organ failure randomized to high-dose glutamine plus antioxidants, glutamine alone, antioxidants alone, or placebo. The result was unexpected and disturbing: the glutamine groups had numerically higher in-hospital and 6-month mortality than the non-glutamine groups, with the difference reaching statistical significance for the combined high-dose intervention.
REDOXS forced a re-evaluation of the field. Subsequent analysis identified several issues that likely explain the discordant result:
- Dosing was at the upper end of historical trials. The combined IV + enteral glutamine load in REDOXS was approximately 0.5 g/kg/day, well above the 0.2-0.3 g/kg/day used in most earlier positive trials.
- Many enrolled patients had multi-organ failure including renal and hepatic dysfunction. Glutamine generates ammonia during metabolism, and in patients with impaired renal or hepatic clearance, supraphysiologic glutamine loading may produce subclinical hyperammonemia that worsens outcomes.
- Baseline plasma glutamine was not measured at enrollment. A subgroup analysis suggested that patients with baseline plasma glutamine in the normal-to-high range did worse with supplementation, while those with low baseline glutamine showed a non-significant trend toward benefit — consistent with the hypothesis that glutamine supplementation helps only when there is a deficit to correct.
The post-REDOXS consensus is that glutamine remains indicated in burn patients, in select surgical populations, and in patients with documented or strongly suspected glutamine deficiency, but routine high-dose supplementation in all-comers ICU patients is no longer recommended. The Cruzat 2018 Nutrients review provides the modern integrated framework: dose appropriately (0.2-0.3 g/kg/day enteral), avoid in multi-organ failure with renal or hepatic dysfunction, and target the populations with documented benefit.
Major Surgery and Bone Marrow Transplant
Outside the ICU, the surgical and bone-marrow-transplant literature on glutamine remains generally favorable. Ziegler's 1992 Annals of Internal Medicine trial in patients undergoing allogeneic bone marrow transplantation showed that glutamine-supplemented parenteral nutrition reduced length of stay, infectious morbidity, and improved nitrogen balance — a setting where the catabolic stress of conditioning chemotherapy and the immunosuppression of transplant make glutamine demand particularly high.
In elective major abdominal surgery, perioperative glutamine supplementation (typically 0.3-0.4 g/kg/day) is associated with reduced postoperative infections and shorter hospital stays in multiple smaller trials and at least two meta-analyses. The effect size is modest but consistent. The ESPEN (European Society for Clinical Nutrition and Metabolism) guidelines currently recommend perioperative glutamine in selected high-risk surgical patients, particularly those undergoing major upper GI surgery, pancreatectomy, or esophagectomy.
The Post-Exercise "Open Window" of Immune Vulnerability
Lucy Castell and Eric Newsholme's 1997 paper in Nutrition introduced what became known as the "open-window hypothesis": after prolonged exhaustive exercise (marathons, ultra-endurance events, multi-hour training sessions), plasma glutamine drops by 20-40% and remains depressed for 12-72 hours. During this window, athletes experience measurable suppression of lymphocyte function and a 2-6× higher rate of upper respiratory tract infection compared to less-active controls. Glutamine supplementation in their original trial reduced the post-event URTI rate in marathon runners.
Subsequent work has nuanced this picture. The post-exercise immune dip is real and reliably reproducible, but the contribution of glutamine specifically (versus generalized stress hormones, cytokines, and other catabolic signals) is harder to isolate. Modern sports-nutrition reviews (Coqueiro 2019, Walsh 1998) treat glutamine as one component of post-event recovery rather than a standalone immune intervention — alongside carbohydrate replenishment, vitamin D adequacy, and sleep. The companion Exercise Recovery deep-dive page explores this further.
For practical purposes, endurance athletes preparing for or recovering from events lasting more than two hours typically supplement with 5-10 g of L-glutamine per day during the high-training-load period, with an additional 5 g immediately post-event. The evidence is suggestive rather than definitive, but the safety profile is excellent and the cost is low.
Chronic Infection Recovery and HIV
The Calder & Yaqoob 1999 Amino Acids review surveyed the role of glutamine in chronic infection and HIV. HIV-positive patients with wasting syndrome typically show low plasma glutamine, and supplementation has been studied as an adjunct to antiretroviral therapy for preserving lean body mass and supporting immune function. Several small trials showed weight gain and trends toward improved CD4 counts in glutamine-supplemented patients, though large definitive trials were never completed before the advent of effective antiretrovirals made HIV-wasting syndrome much less common.
For chronic infection recovery in immunocompetent patients — the post-Lyme, post-mononucleosis, post-COVID (where appropriate to discuss with one's clinician), or general "post-viral fatigue" populations — glutamine is sometimes used as part of immune-support protocols at 5-10 g/day for 4-12 weeks. The evidence base is weak compared to the burn-and-trauma literature, but the mechanism is biologically plausible and the safety profile permits an empirical trial.
Dosing, Routes, and Alanyl-Glutamine Dipeptide
Oral Powder (Most Common Outpatient Form)
- Maintenance immune support: 5 g once or twice daily, on an empty stomach, dissolved in room-temperature water
- Acute illness or post-event recovery: 10 g 2-3 times daily for 5-14 days, then taper
- Burn or surgical pre-habilitation (outpatient phase): 0.3 g/kg/day in divided doses for 2 weeks before elective surgery, continued post-operatively as tolerated
Alanyl-Glutamine Dipeptide (Parenteral / Enteral Tube Feeds)
Free L-glutamine is unstable in solution at neutral pH and degrades to ammonia and pyroglutamic acid when stored in IV bags, which is why clinical parenteral glutamine is administered as the more stable L-alanyl-L-glutamine dipeptide (brand name Dipeptiven). This is the form used in most modern ICU and surgical trials, and the form referenced in the ESPEN guidelines for parenteral nutrition. Typical dosing is 0.3-0.4 g/kg/day as the dipeptide.
Timing
Oral glutamine is best absorbed on an empty stomach. Avoid hot beverages (denaturation). Do not combine with high-protein meals if you want maximum absorption — other amino acids compete for the same intestinal transporters.
Cautions (Including the REDOXS-Era Caveats)
- Multi-organ failure with renal or hepatic dysfunction — the principal lesson of REDOXS. Avoid supraphysiologic glutamine in this setting; the increase in ammonia generation may not be safely cleared.
- Hepatic encephalopathy — the same ammonia issue, more acutely. Glutamine should not be supplemented in active encephalopathy.
- Active cancer — "glutamine addiction" of rapidly dividing tumor cells (Wise & Thompson 2010) is a real phenomenon. Some studies suggest benefit from glutamine in reducing chemotherapy-induced mucositis (Sayles 2016); others raise concerns about fueling tumor growth. Cancer patients should consult their oncology team.
- Seizure disorders — glutamine is the metabolic precursor to glutamate, the principal excitatory neurotransmitter; use cautiously.
- Severe renal insufficiency or dialysis — consult nephrology before supplementing.
- Routine high-dose supplementation in unselected ICU populations — not recommended post-REDOXS. Reserve for burns, trauma, selected surgical patients, and documented deficiency.
Key Research Papers
- Ardawi MS, Newsholme EA (1983). Glutamine metabolism in lymphocytes of the rat. Biochemical Journal. Foundational measurement establishing glutamine's role in lymphocyte metabolism. — PubMed
- Lacey JM, Wilmore DW (1990). Is glutamine a conditionally essential amino acid? Nutrition Reviews. The classic paper introducing the conditionally essential concept. — PubMed
- Newsholme P (2001). Why is L-glutamine metabolism important to cells of the immune system in health, postinjury, surgery or infection? Journal of Nutrition. — PubMed
- Calder PC, Yaqoob P (1999). Glutamine and the immune system. Amino Acids. — PubMed
- Cruzat V, Macedo Rogero M, Noel Keane K, Curi R, Newsholme P (2018). Glutamine: Metabolism and Immune Function, Supplementation and Clinical Translation. Nutrients 10(11):1564. The modern integrated review. — PubMed
- Wischmeyer PE (2003). Clinical applications of L-glutamine: past, present, and future. Nutrition in Clinical Practice. — PubMed
- Wischmeyer PE et al. (2001). Glutamine administration reduces gram-negative bacteremia in severely burned patients. Critical Care Medicine. — PubMed
- Garrel D et al. (2003). Decreased mortality and infectious morbidity in adult burn patients given enteral glutamine supplements. Critical Care Medicine. — PubMed
- Novak F, Heyland DK, Avenell A, Drover JW, Su X (2002). Glutamine supplementation in serious illness: a systematic review of the evidence. Critical Care Medicine 30(9):2022-9. — PubMed
- Heyland D, Muscedere J, Wischmeyer PE et al. (2013). A randomized trial of glutamine and antioxidants in critically ill patients (REDOXS trial). NEJM 368:1489-1497. The trial that reshaped ICU glutamine practice. — PubMed
- Ziegler TR et al. (1992). Clinical and metabolic efficacy of glutamine-supplemented parenteral nutrition after bone marrow transplantation. Annals of Internal Medicine. — PubMed
- Van der Hulst RR, van Kreel BK, von Meyenfeldt MF et al. (1993). Glutamine and the preservation of gut integrity. The Lancet 341(8857):1363-5. — PubMed
- Sayles C et al. (2016). Oral glutamine in preventing treatment-related mucositis in adult patients with cancer. Nutrition in Clinical Practice. — PubMed
- Castell LM, Newsholme EA (1997). The effects of oral glutamine supplementation on athletes after prolonged, exhaustive exercise. Nutrition. The "open window" paper. — PubMed
PubMed Topic Searches
- PubMed: Glutamine and immune cell function
- PubMed: Glutamine in burns, sepsis, ICU
- PubMed: Alanyl-glutamine dipeptide
- PubMed: Glutamine, exercise, and the open window
- PubMed: Glutamine in surgical infection prevention
Connections
- Glutamine Overview
- Glutamine Benefits Hub
- Glutamine for Gut Health & Leaky Gut
- Glutamine for Exercise Recovery
- Glutamine for Weight Loss Support
- Arginine
- Cysteine
- Glycine
- NAC & Glutathione
- Vitamin D3
- Vitamin A for Immune Function
- Vitamin C
- Zinc
- Selenium
- Immune Boosting
- Gut Healing
- Fatigue
- Pneumonia
- Crohn's Disease
- Inflammatory Bowel Disease
- Inflammatory Markers
- Bone Broth