Glutamine for Exercise Recovery
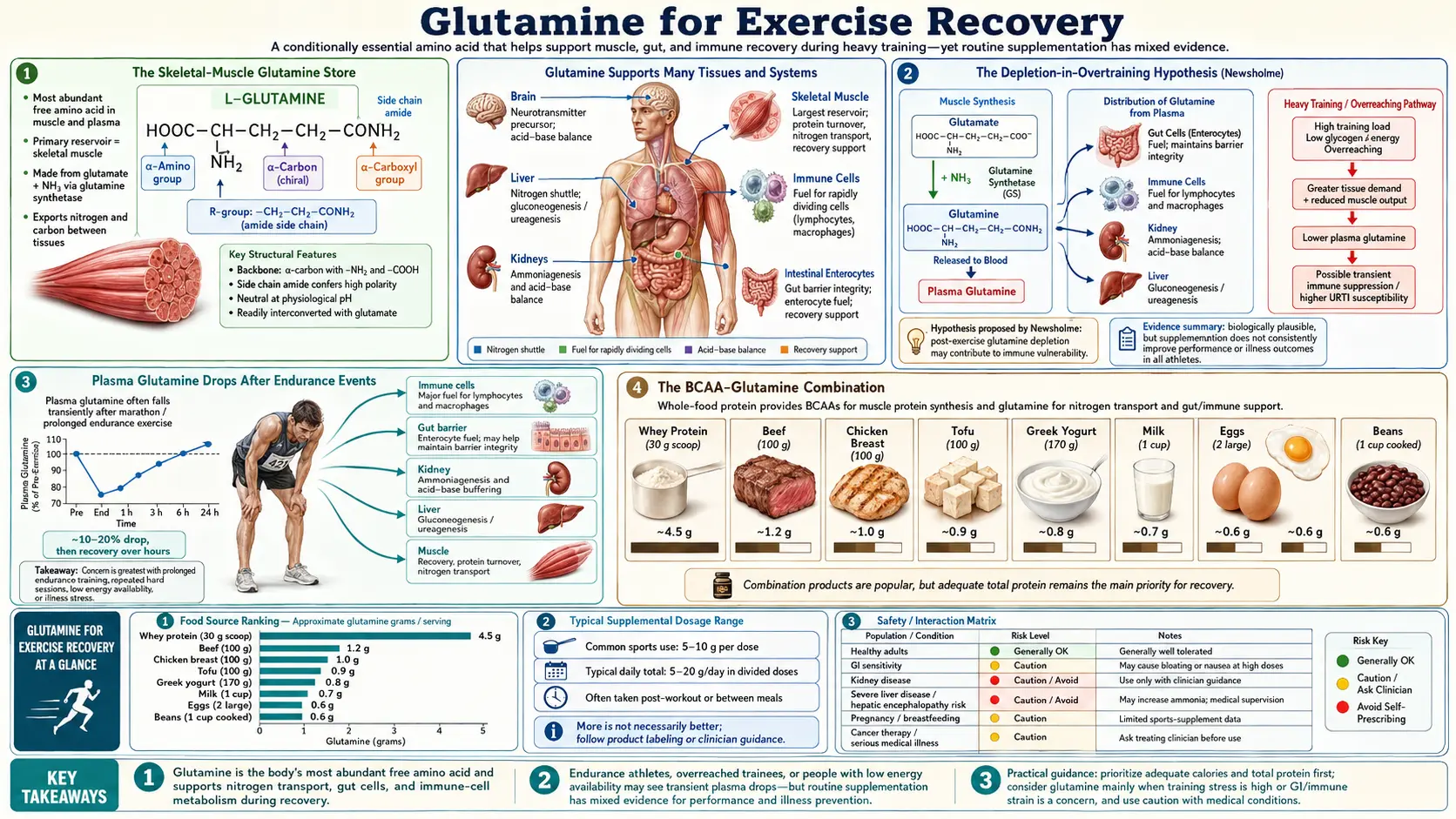
Skeletal muscle is the body's glutamine warehouse — roughly 60% of the intramuscular free amino acid pool is glutamine, and that store is the body's principal buffer against the glutamine demands of the immune system, gut, and kidney under stress. Prolonged or intense exercise drains this store in a measurable way: plasma glutamine falls 20-40% after marathons and ultra-endurance events and remains depressed for 12-72 hours, and chronic overtraining is associated with persistently low plasma glutamine that Eric Newsholme proposed as one of the biochemical markers of the overtraining syndrome. The clinical picture for the recreational lifter is more nuanced — glutamine has not been shown to increase strength, lean mass, or hypertrophy in well-fed weight-trained subjects — but for endurance athletes, athletes during high-volume training blocks, and athletes managing post-exercise URTIs and gut symptoms, the evidence supports a meaningful role for supplementation. This deep-dive walks through the depletion mechanism, the trial evidence, the BCAA-glutamine combination, and where the evidence is strong versus where it remains thin.
Table of Contents
- The Skeletal-Muscle Glutamine Store
- The Depletion-in-Overtraining Hypothesis (Newsholme)
- Plasma Glutamine Drops After Endurance Events
- The BCAA-Glutamine Combination
- Glycogen Resynthesis (Bowtell 1999)
- Muscle Soreness and Recovery (Legault, Street)
- Exercise-Induced Gut Permeability
- Oral vs IV Glutamine
- Where the Evidence Is Strong — And Where It Remains Thin
- Dosing Protocols for Athletes
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Skeletal-Muscle Glutamine Store
The free amino-acid pool in skeletal muscle is dominated by glutamine: roughly 60% of the intramuscular free amino acid pool is glutamine, and the total body free glutamine pool is approximately 70-80 grams, with the vast majority residing in skeletal muscle. By comparison, plasma free glutamine accounts for only a few hundred milligrams. Skeletal muscle is therefore functioning as the body's glutamine warehouse, releasing glutamine into circulation on demand whenever the immune system, gut, kidney, or liver require it.
Under ordinary resting conditions this works smoothly — muscle synthesizes glutamine continuously (the glutamine synthetase reaction adds an amide nitrogen from ammonia to glutamate, using ATP), and exports it to circulation at a rate that matches uptake by the immune system, gut, kidney, and liver. Under conditions of catabolic stress — major trauma, sepsis, severe burns, intense or prolonged exercise — muscle glutamine release accelerates, but eventually demand outstrips intramuscular synthesis, and net protein breakdown follows to liberate additional amino acids that can feed into the glutamine synthesis pathway.
This is the mechanism behind the visible muscle wasting of chronically ill or septic patients, and it is also the mechanism behind the more subtle catabolism that competitive endurance athletes experience during heavy training blocks.
The Depletion-in-Overtraining Hypothesis (Newsholme)
In the early 1990s, Eric Newsholme at Oxford proposed that the so-called overtraining syndrome — the constellation of fatigue, performance decrement, sleep disturbance, mood symptoms, and increased URTI susceptibility that affects athletes in chronic high-volume training — could be partly explained by chronic depletion of plasma glutamine. Athletes in heavy training were measured to have plasma glutamine levels 20-40% below those of less-active controls or below their own pre-season baseline, with the lowest values correlating with the most severe symptoms.
The depletion-in-overtraining hypothesis has held up partially. Glutamine depletion is reliably documented in overtrained athletes, and supplementation does appear to attenuate some of the immune consequences (URTI rate, lymphocyte function). But overtraining syndrome is multifactorial — cortisol elevation, autonomic dysregulation, central fatigue mechanisms, sleep disruption, micronutrient depletion, and possibly mitochondrial adaptations all play roles — and glutamine repletion does not by itself reverse the syndrome. The Walsh 1998 Sports Medicine review and the Coqueiro 2019 Nutrients update treat glutamine as one component of overtraining management, not as a silver bullet.
Plasma Glutamine Drops After Endurance Events
Castell and Newsholme's 1997 paper in Nutrition documented the classic finding: marathon runners showed a 20% drop in plasma glutamine in the hours after race completion, with values remaining below baseline for 24-72 hours. Ultra-endurance events (Ironman triathlons, multi-day stage races) produce larger and longer-lasting drops. The mechanism is a combination of accelerated immune-cell uptake during the post-exercise inflammatory response, accelerated gut uptake to repair exercise-induced barrier dysfunction, and reduced rate of intramuscular synthesis during the recovery period.
The clinical relevance: this post-event glutamine valley correlates with the well-documented post-event "open-window" of immune vulnerability, during which marathon runners and ultra-endurance athletes experience URTIs at roughly 2-6× the rate of less-active controls. The Castell trial found that glutamine supplementation (5 g immediately and 5 g two hours post-event) reduced URTI rate in the week following a marathon from approximately 51% to 19%.
For practical purposes, endurance athletes whose training or competition schedule includes events longer than 90-120 minutes typically supplement with 5-10 g of L-glutamine daily during the high-volume period, with an additional 5 g immediately after long sessions or races.
The BCAA-Glutamine Combination
Branched-chain amino acids (leucine, isoleucine, valine) and glutamine are often combined in sports-nutrition products because they target complementary aspects of the muscle catabolism problem. BCAAs — particularly leucine — are the principal anabolic-signaling amino acids, activating mTORC1 and driving muscle protein synthesis. Glutamine does not directly activate mTORC1 to a meaningful degree (the early literature on this was complicated by cell-culture artifacts), but it supplies the gut and immune system substrate that prevents the catabolic side of the equation from overwhelming the anabolic stimulus of leucine.
In trained subjects, isolated glutamine supplementation has not been shown to increase muscle protein synthesis, strength, or hypertrophy in well-controlled trials. The BCAA-glutamine combination has more support, but the active ingredient is generally the BCAAs — glutamine is the gut-and-immune supporting partner, not the anabolic driver. The Gleeson 2008 Journal of Nutrition review on dosing in exercise covers this nuance: glutamine's role in sports nutrition is recovery and immune support, not direct hypertrophy.
Glycogen Resynthesis (Bowtell 1999)
Bowtell and colleagues' 1999 paper in the Journal of Applied Physiology tested whether oral glutamine could accelerate post-exercise glycogen resynthesis. The answer turned out to be yes, modestly: glutamine combined with carbohydrate produced approximately 25% greater muscle glycogen resynthesis at 2 hours post-exercise compared to carbohydrate alone, even when total carbohydrate intake was matched.
The mechanism is gluconeogenic: hepatic and renal conversion of glutamine to glucose adds to the blood-glucose pool available for muscle glycogen synthesis. For an endurance athlete who needs to recover quickly between sessions (multi-day races, two-a-day training, tournaments), this incremental glycogen-resynthesis effect can be meaningful. Typical post-exercise dosing for this purpose: 0.1 g/kg glutamine (roughly 7-8 g for a 70-80 kg athlete) combined with the post-exercise carbohydrate dose.
Muscle Soreness and Recovery (Legault, Street)
The Legault, Bagnall, and Kimmerly 2015 trial in IJSNEM randomized recreational athletes to oral L-glutamine or placebo and assessed recovery of muscle strength and soreness following a session of unilateral knee-extension eccentric exercise. The glutamine group showed:
- Faster recovery of peak torque at 24 and 72 hours post-exercise
- Lower subjective muscle soreness ratings at 24, 48, and 72 hours
- No effect on serum creatine kinase or other markers of structural muscle damage
The Street et al. 2011 trial in the Journal of Exercise Science and Fitness reported similar findings using a different eccentric exercise protocol. The Cordova-Martinez 2021 trial in professional basketball players found that glutamine supplementation during a competitive season reduced muscular damage biomarkers and shortened perceived recovery time between games.
The consistent finding across these trials is that glutamine modestly accelerates functional recovery (strength return, perceived soreness) without affecting the underlying structural muscle damage. The mechanism is probably some combination of immune-modulation (reducing the secondary inflammatory damage that follows initial mechanical injury), gut-barrier preservation (reducing the systemic endotoxin load from exercise-induced permeability), and possibly direct effects on muscle glutamine availability for protein synthesis during the repair phase.
Exercise-Induced Gut Permeability
Prolonged intense exercise — particularly endurance events in heat — produces a transient but measurable increase in intestinal permeability. The mechanism is splanchnic ischemia (blood is shunted away from the gut to the muscles), followed by reperfusion injury and inflammatory damage to the gut barrier. Endurance athletes are well aware of this phenomenon under its informal name: "runner's gut" or "runner's diarrhea."
The systemic consequence is endotoxemia — bacterial LPS translocates across the compromised gut barrier into systemic circulation, where it activates innate immune signaling. This is one of the mechanisms contributing to the post-exercise immune dip and to the systemic inflammation that follows prolonged events. Glutamine supplementation supports the recovery of gut barrier function in this setting (covered in detail in the companion Gut Health & Leaky Gut page), reducing endotoxin translocation and the downstream inflammatory cascade.
Several trials in marathon runners and triathletes have measured this directly: glutamine supplementation in the days before and immediately after long endurance events reduces serum LPS and pro-inflammatory cytokines compared to placebo, and reduces self-reported GI symptoms during long events.
Oral vs IV Glutamine
Oral L-glutamine powder is the form used in essentially all sports nutrition contexts. Bioavailability is good (roughly 70-80% survives first-pass splanchnic extraction; the splanchnic bed retains 20-30% for enterocyte and hepatic use, which is itself a desirable effect for the gut-barrier and gut-permeability applications). Onset of plasma elevation is approximately 30-45 minutes for ingested doses up to 10 g.
IV glutamine (as the alanyl-glutamine dipeptide) is used in clinical critical-care settings and has no role in normal sports-nutrition contexts — the cost, risk, and inconvenience are unjustified outside of patients who cannot tolerate enteral feeding. The clinical IV-dosing protocols (0.3-0.4 g/kg/day) are also much higher than the doses sports-nutrition athletes typically use.
Where the Evidence Is Strong — And Where It Remains Thin
Evidence is strong (or at least consistent across multiple trials)
- Reduced post-event URTI rate in endurance athletes — Castell 1997 and replications
- Modestly accelerated glycogen resynthesis post-exercise — Bowtell 1999
- Reduced subjective muscle soreness and faster strength recovery after eccentric exercise — Legault 2015, Street 2011
- Reduced exercise-induced gut permeability and endotoxin translocation — multiple smaller trials
- Reduced muscular damage biomarkers during competitive season — Cordova-Martinez 2021
- Improved nitrogen balance and lean-mass preservation during catabolic stress — clinical-care literature extrapolated to extreme training contexts
Evidence is thin or absent
- Increased muscle protein synthesis in well-fed trained subjects — not supported
- Direct hypertrophy or strength gains in resistance-trained subjects — not supported in well-controlled trials
- Improved aerobic capacity or VO2max — not supported
- Performance benefit in single-session events under 90 minutes — not supported
The take-home for athletes: glutamine is a recovery and immune-support nutrient, not a performance-enhancing aid. It earns its place in the supplement stack for athletes with high training volume, endurance athletes, and athletes managing recurrent URTIs or gut symptoms — not for power athletes or recreational lifters looking for hypertrophy.
Dosing Protocols for Athletes
Endurance athletes during high-volume training blocks
- 5 g L-glutamine on an empty stomach in the morning
- 5 g immediately post-training (combine with carbohydrate for glycogen resynthesis)
- Total daily dose 10-15 g during peak weeks; taper to 5 g/day off-season
Around-event protocol for marathons, ultras, triathlons
- 5 g daily for 2 weeks before the event
- 5 g 2 hours before the event start (helps preserve gut barrier under exercise load)
- 5 g immediately at finish
- 5 g twice daily for 5-7 days post-event (URTI prevention window)
Strength / resistance training athletes
- 5 g post-workout, combined with whey protein or other complete-protein source — primarily as gut-immune support during high-volume blocks; little expected anabolic benefit
- Not necessary in off-season or maintenance training
Recovery from a defined overtraining episode
- 10-20 g/day in divided doses for 2-4 weeks
- Combined with rest, nutritional adequacy, and management of contributing factors (sleep, stress, micronutrient status)
Cautions
- Liver disease / hepatic encephalopathy — avoid; impaired ammonia clearance.
- Severe kidney disease — consult a nephrologist; the renal glutamine-to-ammonia pathway is normally protective but in severe CKD can become problematic.
- Active cancer — consult oncology team; "glutamine addiction" of some tumor cell types is a real concern.
- Seizure disorders — glutamine converts to glutamate; use cautiously and start low.
- Inadequate carbohydrate intake — glutamine cannot substitute for proper periworkout carbohydrate; treating it as a "low-carb glycogen hack" produces neither the glycogen-resynthesis benefit nor the recovery benefit.
- Acute GI distress while running — if oral glutamine is taken too close to event start, it can occasionally cause GI symptoms in sensitive individuals; test pre-event dosing during training first.
Key Research Papers
- Castell LM, Newsholme EA (1997). The effects of oral glutamine supplementation on athletes after prolonged, exhaustive exercise. Nutrition. The foundational "open-window" trial. — PubMed
- Legault Z, Bagnall N, Kimmerly DS (2015). The Influence of Oral L-Glutamine Supplementation on Muscle Strength Recovery and Soreness Following Unilateral Knee Extension Eccentric Exercise. International Journal of Sport Nutrition and Exercise Metabolism. — PubMed
- Street B et al. (2011). Glutamine supplementation in recovery from eccentric exercise attenuates strength loss and muscle soreness. Journal of Exercise Science and Fitness. — PubMed
- Bowtell JL et al. (1999). Effect of oral glutamine on whole body carbohydrate storage during recovery from exhaustive exercise. Journal of Applied Physiology. — PubMed
- Coqueiro AY, Raizel R, Bonvini A, Tirapegui J, Rogero MM (2019). Glutamine as an Anti-Fatigue Amino Acid in Sports Nutrition. Nutrients. The modern sports-nutrition review. — PubMed
- Walsh NP, Blannin AK, Robson PJ, Gleeson M (1998). Glutamine, exercise and immune function. Links and possible mechanisms. Sports Medicine. The classic mechanistic review. — PubMed
- Gleeson M (2008). Dosing and efficacy of glutamine supplementation in human exercise and sport training. Journal of Nutrition. — PubMed
- Hickson RC et al. (1995). Glutamine prevents downregulation of myosin heavy chain synthesis and muscle atrophy from glucocorticoids. American Journal of Physiology. — PubMed
- Biolo G, Zorat F, Antonione R, Ciocchi B (2005). Muscle glutamine depletion in the intensive care unit. International Journal of Biochemistry and Cell Biology. — PubMed
- Cordova-Martinez A et al. (2021). Effect of glutamine supplementation on muscular damage biomarkers in professional basketball players. Nutrients. — PubMed
- Cruzat V et al. (2018). Glutamine: Metabolism and Immune Function, Supplementation and Clinical Translation. Nutrients. — PubMed
PubMed Topic Searches
- PubMed: Glutamine, exercise, and endurance recovery
- PubMed: Glutamine and overtraining
- PubMed: Glutamine and post-eccentric soreness
- PubMed: Glutamine and glycogen resynthesis
- PubMed: Glutamine and post-event URTIs
Connections
- Glutamine Overview
- Glutamine Benefits Hub
- Glutamine for Gut Health & Leaky Gut
- Glutamine for Immune Function
- Glutamine for Weight Loss Support
- Leucine (BCAA)
- Isoleucine
- Valine
- Arginine
- Glycine
- NAC & Glutathione
- Magnesium
- Zinc
- Vitamin D3
- Vitamin C
- Stress Management
- Gut Healing
- Fatigue
- Pain
- Bone Broth
- Collagen
- Inflammatory Markers