Glutamine — Benefits Deep Dive
Glutamine is the single most abundant free amino acid in the human body — circulating in plasma at higher concentrations than any other amino acid and stored in skeletal muscle at roughly 60% of the total free amino-acid pool. Although the liver, lungs, and skeletal muscle synthesize it endogenously under ordinary conditions, glutamine becomes conditionally essential during catabolic stress: critical illness, major surgery, severe burns, sepsis, prolonged endurance exercise, and chemotherapy can all drive plasma glutamine below the threshold at which gut enterocytes, lymphocytes, and macrophages can no longer function normally. Four benefit pages below explore where supplemental glutamine produces the largest documented clinical effect — gut barrier repair in leaky gut and IBD, immune support in trauma and ICU populations, recovery from heavy training, and weight management through cravings, lean-mass preservation, and microbiome modulation.
Deep-Dive Articles
Gut Health & Leaky Gut
Glutamine as the primary fuel for enterocytes, the upregulation of tight-junction proteins (claudin-1, occludin, ZO-1), heat shock protein induction, mucin synthesis support, and the clinical protocol for repairing increased intestinal permeability driven by NSAIDs, alcohol, chronic stress, gluten sensitivity, dysbiosis, and intense exercise. Includes Benjamin 2012 Crohn's trial, Zhou 2019 post-infectious IBS trial, and the Achamrah bench-to-bedside framework.
Immune Function
Glutamine as the dominant fuel for rapidly dividing lymphocytes, neutrophils, and macrophages — consumed at rates rivaling glucose. The Wischmeyer burn and ICU trials, the REDOXS trial controversy, the conditional-essentiality framework of Lacey and Wilmore, immunonutrition in surgical patients, and why the "anti-fatigue" effect of glutamine in athletes is really an immune-support effect against the post-exercise "open-window" of vulnerability.
Exercise Recovery
The Newsholme depletion-in-overtraining hypothesis, plasma glutamine drops of 20-40% after marathon and ultra-endurance events, the BCAA-glutamine synergy, post-exercise glycogen resynthesis (Bowtell), muscle soreness attenuation (Legault, Street), and the oral-vs-IV question. Where the evidence is strong (recovery, immune protection, gut barrier in athletes) and where it remains thin (direct hypertrophy, strength gains in trained lifters).
Weight Loss Support
The sublingual L-glutamine craving-extinction technique (1-2 g under the tongue, relief in minutes via gluconeogenic glucose support to the brain), preservation of lean muscle mass during calorie restriction, the de Souza 2015 gut-microbiota shift in overweight adults, the Greenfield 2009 GLP-1 augmentation finding, and the Laviano 2014 pilot trial in obese non-dieting women. Why glutamine is a foundational metabolic-support nutrient, not a fat burner.
Table of Contents
- Deep-Dive Articles
- Why Glutamine Produces Effects Across Many Systems
- Research Papers: Gut Health & Leaky Gut
- Research Papers: Immune Function & Critical Care
- Research Papers: Exercise Recovery
- Research Papers: Weight Loss, Metabolic Health, Cravings
- Research Papers: Cross-Cutting (Mechanism, Glutathione, Safety)
- External Authoritative Resources
- Connections
- Featured Videos
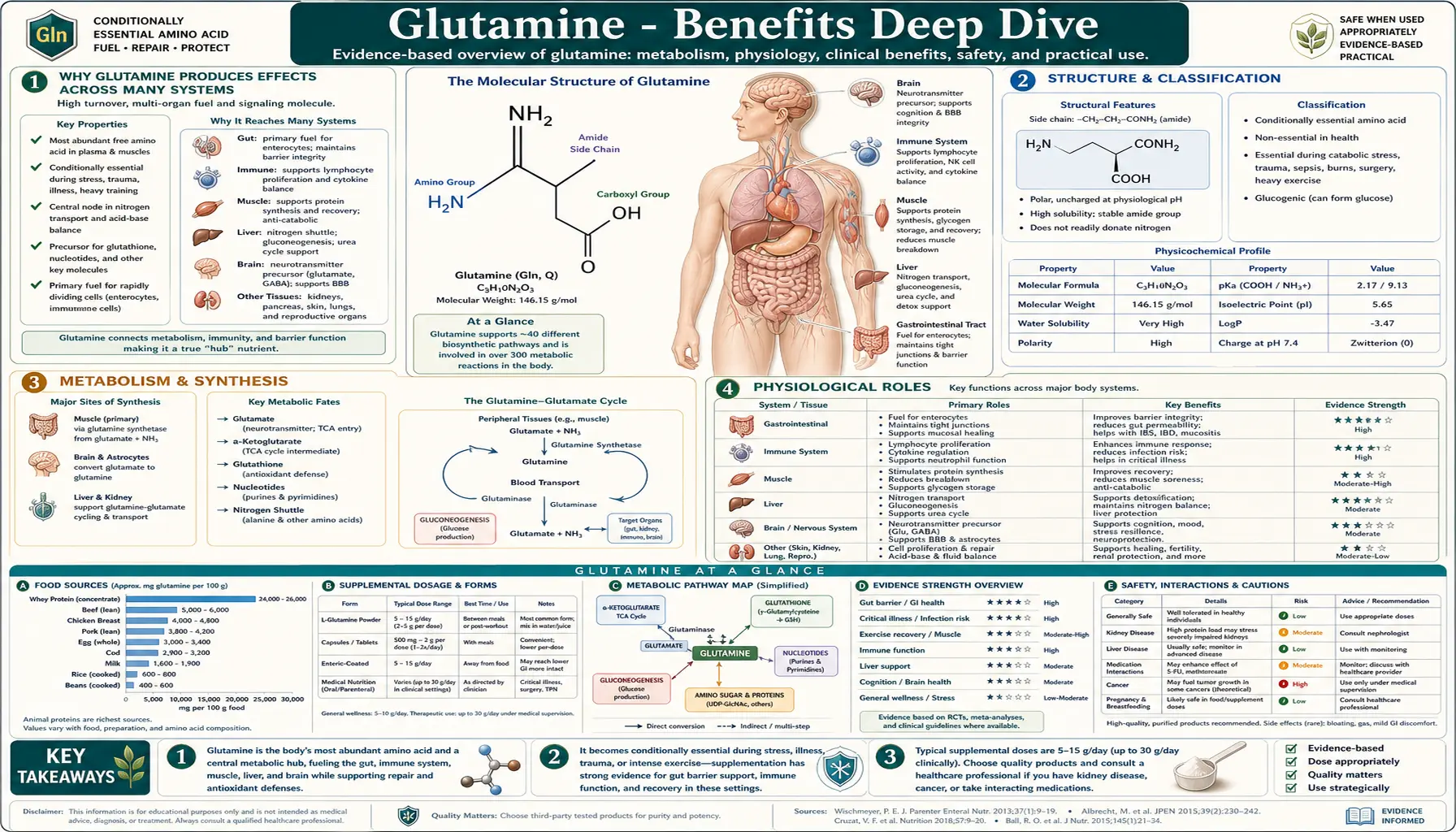
Why Glutamine Produces Effects Across Many Systems
Most amino acids have one or two principal jobs. Glutamine has at least five, which is why it shows up in nearly every major organ system and why supplementing it can produce measurable effects on gut, immunity, recovery, and metabolism simultaneously. The molecule is unusual because it carries two nitrogen atoms (one in the alpha-amino group, one in the amide side chain), making it the body's preferred nitrogen carrier between tissues. Five distinct roles map to five distinct clinical effect categories.
- Primary fuel for enterocytes (intestinal lining cells) — enterocytes turn over every 3-5 days and prefer glutamine over glucose for ATP production. This is the mechanism behind the gut-barrier and leaky-gut effects: without adequate glutamine, the rapidly dividing intestinal epithelium cannot maintain its tight junctions, mucus layer, or rate of turnover, and increased intestinal permeability ensues.
- Primary fuel for rapidly dividing immune cells — lymphocytes, neutrophils, and macrophages consume glutamine at rates comparable to or exceeding glucose, especially during an active immune response. This is the mechanism behind the immune-support effects in burns, trauma, ICU patients, and post-exercise athletes, all of whom show measurable plasma glutamine depletion correlated with infection risk.
- Inter-organ nitrogen carrier — glutamine is the principal vehicle that shuttles nitrogen from peripheral tissues to the liver (for urea synthesis), kidney (for ammonia production and acid-base balance), and gut (for nucleotide synthesis). During catabolic stress, skeletal muscle breaks down its protein stores specifically to liberate glutamine for these other tissues, which is why prolonged stress, sepsis, or starvation produces visible muscle wasting.
- Gluconeogenic substrate — both the liver and the renal cortex can convert glutamine to glucose, making it a non-carbohydrate source of blood sugar between meals and during fasting. This is the mechanism behind the sublingual craving-extinction technique: a small dose dissolved under the tongue rapidly supplies the brain with usable glucose precursor, blunting the urgency of a sugar or alcohol craving within minutes.
- Precursor to glutamate (and downstream GABA) and to glutathione — in the brain, glutamine crosses the blood-brain barrier and feeds the glutamate-glutamine cycle that supplies both the principal excitatory neurotransmitter (glutamate) and, indirectly, the principal inhibitory neurotransmitter (GABA). Throughout the body, glutamine supplies the glutamate backbone of glutathione, the most abundant endogenous antioxidant. Glutamine depletion therefore impairs both neurotransmission and antioxidant defense in addition to its more obvious gut and immune effects.
The therapeutic implication of these five overlapping roles is that under conditions of catabolic stress — burn injury, sepsis, major surgery, intense endurance training, severe inflammatory bowel disease, chemotherapy, prolonged calorie restriction — the demand for glutamine in any one of these roles can starve the others. The classical observation from intensive care medicine is that plasma glutamine below approximately 420 µmol/L on ICU admission predicts increased mortality, independent of other markers of severity. The fifth deep-dive page on this hub explores the metabolic side of this story: how glutamine supplementation can support healthy body composition during caloric restriction by preserving the lean muscle that would otherwise be cannibalized to supply glutamine to gut, immune, and renal systems.
Research Papers: Gut Health & Leaky Gut
- Kim MH, Kim H (2017). The Roles of Glutamine in the Intestine and Its Implication in Intestinal Diseases. International Journal of Molecular Sciences. — PubMed
- Rao R, Samak G (2012). Role of Glutamine in Protection of Intestinal Epithelial Tight Junctions. Journal of Epithelial Biology and Pharmacology. — PubMed
- Achamrah N, Déchelotte P, Coëffier M (2017). Glutamine and the regulation of intestinal permeability: from bench to bedside. Current Opinion in Clinical Nutrition and Metabolic Care. — PubMed
- Wang B et al. (2015). Glutamine and intestinal barrier function. Amino Acids. — PubMed
- Van der Hulst RR et al. (1993). Glutamine and the preservation of gut integrity. The Lancet. — PubMed
- Benjamin J et al. (2012). Glutamine and whey protein improve intestinal permeability and morphology in patients with Crohn's disease. Digestive Diseases and Sciences. — PubMed
- Zhou Q et al. (2019). Randomised placebo-controlled trial of dietary glutamine supplements for postinfectious irritable bowel syndrome. Gut. — PubMed
- Rapin JR, Wiernsperger N (2010). Possible links between intestinal permeability and food processing: A potential therapeutic niche for glutamine. Clinics. — PubMed
- dos Santos R de GC et al. (2010). Alanyl-glutamine in the treatment of chronic diarrhea in children. Journal of Pediatric Gastroenterology and Nutrition. — PubMed
- Souba WW (1993). Glutamine: a key substrate for the splanchnic bed. Annual Review of Nutrition. — PubMed
Research Papers: Immune Function & Critical Care
- Cruzat V, Macedo Rogero M, Noel Keane K, Curi R, Newsholme P (2018). Glutamine: Metabolism and Immune Function, Supplementation and Clinical Translation. Nutrients 10(11):1564. — PubMed
- Newsholme P (2001). Why is L-glutamine metabolism important to cells of the immune system in health, postinjury, surgery or infection? Journal of Nutrition. — PubMed
- Calder PC, Yaqoob P (1999). Glutamine and the immune system. Amino Acids. — PubMed
- Ardawi MS, Newsholme EA (1983). Glutamine metabolism in lymphocytes of the rat. Biochemical Journal. — PubMed
- Wischmeyer PE (2003). Clinical applications of L-glutamine: past, present, and future. Nutrition in Clinical Practice. — PubMed
- Novak F, Heyland DK, Avenell A, Drover JW, Su X (2002). Glutamine supplementation in serious illness: a systematic review of the evidence. Critical Care Medicine 30(9):2022-9. — PubMed
- Heyland D, Muscedere J, Wischmeyer PE et al. (2013). A randomized trial of glutamine and antioxidants in critically ill patients (REDOXS trial). NEJM 368:1489-1497. — PubMed
- Wischmeyer PE et al. (2001). Glutamine administration reduces gram-negative bacteremia in severely burned patients. Critical Care Medicine. — PubMed
- Garrel D et al. (2003). Decreased mortality and infectious morbidity in adult burn patients given enteral glutamine supplements. Critical Care Medicine. — PubMed
- Ziegler TR et al. (1992). Clinical and metabolic efficacy of glutamine-supplemented parenteral nutrition after bone marrow transplantation. Annals of Internal Medicine. — PubMed
- Lacey JM, Wilmore DW (1990). Is glutamine a conditionally essential amino acid? Nutrition Reviews. — PubMed
Research Papers: Exercise Recovery
- Castell LM, Newsholme EA (1997). The effects of oral glutamine supplementation on athletes after prolonged, exhaustive exercise. Nutrition. — PubMed
- Legault Z, Bagnall N, Kimmerly DS (2015). The Influence of Oral L-Glutamine Supplementation on Muscle Strength Recovery and Soreness Following Unilateral Knee Extension Eccentric Exercise. International Journal of Sport Nutrition and Exercise Metabolism. — PubMed
- Coqueiro AY, Raizel R, Bonvini A, Tirapegui J, Rogero MM (2019). Glutamine as an Anti-Fatigue Amino Acid in Sports Nutrition. Nutrients. — PubMed
- Street B et al. (2011). Glutamine supplementation in recovery from eccentric exercise attenuates strength loss and muscle soreness. Journal of Exercise Science and Fitness. — PubMed
- Bowtell JL et al. (1999). Effect of oral glutamine on whole body carbohydrate storage during recovery from exhaustive exercise. Journal of Applied Physiology. — PubMed
- Hickson RC et al. (1995). Glutamine prevents downregulation of myosin heavy chain synthesis and muscle atrophy from glucocorticoids. American Journal of Physiology. — PubMed
- Biolo G, Zorat F, Antonione R, Ciocchi B (2005). Muscle glutamine depletion in the intensive care unit. International Journal of Biochemistry and Cell Biology. — PubMed
- Gleeson M (2008). Dosing and efficacy of glutamine supplementation in human exercise and sport training. Journal of Nutrition. — PubMed
- Cordova-Martinez A et al. (2021). Effect of glutamine supplementation on muscular damage biomarkers in professional basketball players. Nutrients. — PubMed
- Walsh NP, Blannin AK, Robson PJ, Gleeson M (1998). Glutamine, exercise and immune function. Links and possible mechanisms. Sports Medicine. — PubMed
Research Papers: Weight Loss, Metabolic Health, Cravings
- Laviano A, Molfino A, Lacaria MT, Canelli A, De Leo S, Preziosa I, Rossi Fanelli F (2014). Glutamine supplementation favors weight loss in nondieting obese female patients: A pilot study. European Journal of Clinical Nutrition. — PubMed
- de Souza AZ, Zambom AZ, Abboud KY et al. (2015). Oral supplementation with L-glutamine alters gut microbiota of obese and overweight adults. Nutrition. — PubMed
- Greenfield JR et al. (2009). Oral glutamine increases circulating glucagon-like peptide 1, glucagon, and insulin concentrations in lean, obese, and type 2 diabetic subjects. American Journal of Clinical Nutrition. — PubMed
- Mansour A et al. (2015). Effect of glutamine supplementation on cardiovascular risk factors in patients with type 2 diabetes. Nutrition. — PubMed
- Samocha-Bonet D, Wong O, Synnott EL et al. (2011). Glutamine reduces postprandial glycemia and augments the glucagon-like peptide-1 response in type 2 diabetes patients. Journal of Nutrition. — PubMed
- Abboud KY et al. (2019). Oral Glutamine Supplementation Reduces Obesity, Pro-Inflammatory Markers, and Improves Insulin Sensitivity in DIO Wistar Rats. Nutrients. — PubMed
- Williams RJ (1959). Alcoholism: the nutritional approach. University of Texas Press (classical observation that glutamine reduces voluntary alcohol consumption). — PubMed
- Chang WK et al. (2003). Glutamine protects against intestinal injury from a methotrexate-induced inflammatory model. JPEN Journal of Parenteral and Enteral Nutrition (intestinal substrate role). — PubMed
- Iwashita S et al. (2005). Glutamine supplementation increases postprandial energy expenditure. JPEN Journal of Parenteral and Enteral Nutrition. — PubMed
- Reimann F, Tolhurst G, Gribble FM (2012). G-protein-coupled receptors in intestinal chemosensation (relevant to GLP-1 release by glutamine). Cell Metabolism. — PubMed
Research Papers: Cross-Cutting (Mechanism, Glutathione, Safety)
- Curi R et al. (2005). Molecular mechanisms of glutamine action. Journal of Cellular Physiology. — PubMed
- Roth E (2008). Nonnutritive Effects of Glutamine. Journal of Nutrition. — PubMed
- Amores-Sánchez MI, Medina MÁ (1999). Glutamine, as a precursor of glutathione, and oxidative stress. Molecular Genetics and Metabolism. — PubMed
- Flaring UB, Rooyackers OE, Wernerman J, Hammarqvist F (2003). Glutamine attenuates post-traumatic glutathione depletion in human muscle. Clinical Science. — PubMed
- Valencia E et al. (2002). Impact of oral L-glutamine on glutathione, glutamine, and glutamate blood levels in volunteers. Nutrition. — PubMed
- Albrecht J, Sidoryk-Węgrzynowicz M, Zielińska M, Aschner M (2010). Roles of glutamine in neurotransmission. Neuron Glia Biology. — PubMed
- Bak LK, Schousboe A, Waagepetersen HS (2006). The glutamate/GABA-glutamine cycle. Journal of Neurochemistry. — PubMed
- Wise DR, Thompson CB (2010). Glutamine addiction: a new therapeutic target in cancer. Trends in Biochemical Sciences. — PubMed
- Garlick PJ (2001). Assessment of the safety of glutamine and other amino acids. Journal of Nutrition. — PubMed
- Ziegler TR et al. (2000). Safety and metabolic effects of L-glutamine administration in humans. JPEN Journal of Parenteral and Enteral Nutrition. — PubMed
External Authoritative Resources
- Linus Pauling Institute — relevant Other Nutrients pages — LPI does not maintain a dedicated glutamine page, but related amino-acid metabolism pages are useful
- NIH Office of Dietary Supplements — Fact Sheets Index — includes amino acid factsheets for clinical reference
- MedlinePlus — Glutamine — consumer-facing summary of evidence, dosing, and cautions
- MDPI Nutrients — open-access journal hosting the Cruzat 2018 and Coqueiro 2019 reviews
- PubMed — All research on glutamine (more than 30,000 indexed papers)
- PubMed — Glutamine clinical trials
- PubMed — Glutamine meta-analyses
Connections
- Glutamine (Main Page)
- Glutamine for Gut Health & Leaky Gut
- Glutamine for Immune Function
- Glutamine for Exercise Recovery
- Glutamine for Weight Loss Support
- All Amino Acids
- Glutamic Acid (Glutamate)
- Glycine
- Cysteine (Glutathione Precursor)
- Arginine
- Leucine (BCAA)
- NAC & Glutathione
- Gut Healing
- Gut-Brain Axis
- Inflammatory Bowel Disease
- Irritable Bowel Syndrome
- Crohn's Disease
- Diabetes
- Obesity
- Bone Broth
- Probiotics
- Collagen
- Zinc
- Blood Sugar
- Fasting