Vitamin A for Immune Function
Vitamin A was originally called the "anti-infective vitamin" by Edward Mellanby and Harry Green in the 1920s, before its mechanism was understood, simply because deficient animals died of infection at strikingly higher rates than replete animals. A century later, the mechanism is well-mapped: retinoic acid is a master regulator of T-cell differentiation (Th17/Treg balance), B-cell class switching to mucosal IgA, dendritic cell gut-homing imprinting, and natural killer cell function. The clinical translation has been one of global health's most successful interventions — the WHO 2×200,000 IU measles protocol roughly halves measles mortality in deficient children, and biannual supplementation programs in 80 countries prevent an estimated 600,000 deaths per year. This deep-dive walks through each immune mechanism, the pivotal clinical trials, and the practical implications for adult patients facing immune-related conditions.
Table of Contents
- The "Anti-Infective Vitamin" — Historical Context
- Mucosal Barrier Integrity (Gut, Lung, Eye, Reproductive Tract)
- T-Cell Maturation and Th17 / Treg Balance
- Dendritic Cells and Gut-Homing Imprinting
- B-Cell Class Switching to Mucosal IgA
- The WHO Measles Protocol (2×200,000 IU)
- Respiratory Infections and Pneumonia
- Diarrheal Disease and Gut Barrier
- Adult Immune Applications
- Cautions (Including the Negative Tuberculosis Signal)
- Key Research Papers
- Connections
- Featured Videos
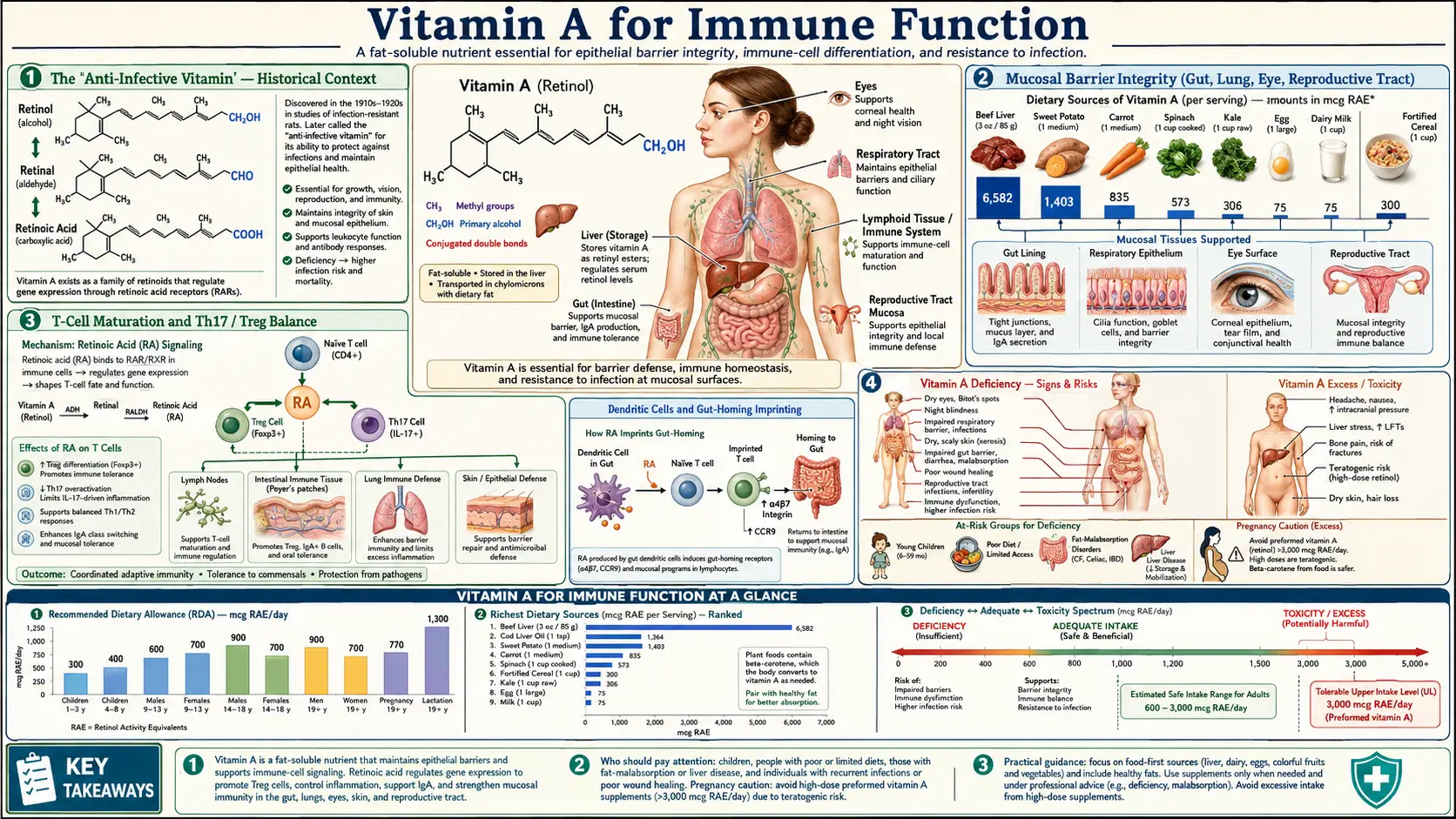
The "Anti-Infective Vitamin" — Historical Context
The phrase "anti-infective vitamin" was coined in the 1920s by Edward Mellanby and Harry Green, working separately, to describe the dramatic protective effect of Vitamin A against infection in laboratory animals. Mellanby's rats fed Vitamin-A-deficient diets developed not only the expected xerophthalmia but also pneumonia, otitis media, urinary tract infections, and severe diarrhea — all of which resolved when Vitamin A was added back to the diet. This was decades before any modern understanding of T cells, cytokines, or nuclear receptor signaling.
The clinical translation in humans came in fits and starts. The Lugar trial in Hyderabad in the 1930s suggested supplementation reduced respiratory mortality in children. The seminal modern work was done by Alfred Sommer at Johns Hopkins through field epidemiology in Indonesia in the 1970s and 1980s. Sommer's 1986 Lancet paper showed that biannual Vitamin A supplementation reduced overall under-5 mortality by 23% in deficient Indonesian children — far more than could be explained by eye disease alone. The reduction was driven primarily by deaths from measles, pneumonia, and diarrhea, confirming the broader immune-protective effect.
Subsequent meta-analyses (Imdad et al. Cochrane Review 2017, pooling 47 trials and over 1.2 million children) have confirmed an approximately 24% reduction in all-cause mortality and a 32% reduction in diarrhea-specific mortality from biannual Vitamin A supplementation in deficient populations. This is one of the largest documented mortality reductions for any nutritional intervention in any setting.
Mucosal Barrier Integrity (Gut, Lung, Eye, Reproductive Tract)
The first line of immune defense is not the immune system in the conventional sense — it is the epithelial barrier that physically separates the body's interior from the outside world. The gut, the respiratory tract, the conjunctiva, and the genitourinary tract are all lined with specialized epithelium that secretes mucus, antimicrobial peptides, and secretory IgA. The integrity of these epithelial barriers depends critically on retinoic acid signaling through the RAR/RXR nuclear receptor complex.
Without adequate Vitamin A, the epithelium undergoes squamous metaplasia — mucus-producing columnar epithelium converts to dry, keratinized squamous epithelium. The conjunctival version of this is visible as Bitot's spots and xerophthalmia. The same process occurs less visibly in the respiratory tree, the gut, and the urinary tract, where it:
- Reduces mucus secretion that traps pathogens and irritants
- Eliminates the cilia that sweep trapped material out of the airways
- Reduces antimicrobial peptide production (defensins, lysozyme)
- Disrupts the tight junctions between epithelial cells, allowing pathogen translocation
- Eliminates the goblet cells that produce the protective mucin layer
The net effect is that pathogens that would normally be cleared by mechanical and chemical defenses now establish infection. The deficient child becomes a near-universal target for any opportunistic respiratory or enteric pathogen circulating in the community — which is why diarrhea and pneumonia are the leading killers of deficient children worldwide, far more than the iconic blindness.
T-Cell Maturation and Th17 / Treg Balance
Beyond the mucosal barrier, retinoic acid plays a direct role in adaptive immunity through its effects on T-cell differentiation. Naive CD4+ T cells encountering antigen can differentiate down several distinct paths: Th1 (cellular immunity, intracellular pathogens), Th2 (humoral immunity, parasites), Th17 (mucosal defense, extracellular bacteria, fungi), or Treg (regulatory T cells that suppress inflammation and prevent autoimmunity).
The balance between Th17 and Treg is particularly sensitive to retinoic acid concentration. In the presence of adequate retinoic acid, naive T cells encountering antigen in mucosal lymphoid tissue tend toward the Treg phenotype, producing IL-10 and TGF-beta to maintain mucosal tolerance to commensal bacteria and food antigens. Without retinoic acid, the same encounter pushes toward the Th17 phenotype, producing IL-17 and IL-22, which is appropriate for fighting fungal and extracellular bacterial infection but pathological when chronic and untargeted — the Th17 axis drives several autoimmune conditions including psoriasis, ankylosing spondylitis, and inflammatory bowel disease.
This Th17/Treg balance has therapeutic implications. Retinoic acid analogs are being explored as adjuncts in inflammatory bowel disease, multiple sclerosis (some animal-model evidence), and graft-versus-host disease. Conversely, Vitamin A deficiency disrupts mucosal tolerance and is associated with increased allergic sensitization, food allergy, and atopic disease in observational studies. The mechanism is the same Th17/Treg disequilibrium, just expressed in different organ systems.
For the related immune-modulating effects of Vitamin D, which works through a separate but parallel nuclear receptor pathway, see our Vitamin D3 page. The two fat-soluble vitamins are often discussed together because both signal through the RXR retinoid X receptor partner and produce complementary effects on adaptive immunity.
Dendritic Cells and Gut-Homing Imprinting
A particularly elegant aspect of retinoic acid immunology is the role of dendritic cells in "imprinting" T cells with gut-homing receptors. CD103+ dendritic cells in mesenteric lymph nodes constitutively express retinaldehyde dehydrogenase (RALDH), the enzyme that converts dietary retinal to active retinoic acid. When these dendritic cells present antigen to a naive T cell, the locally produced retinoic acid induces expression of two surface receptors on the T cell: CCR9 (a chemokine receptor that recognizes thymus-expressed chemokine TECK/CCL25 produced by small intestinal epithelium) and integrin alpha4-beta7 (which binds MAdCAM-1 expressed on mucosal vessel endothelium).
The dual expression of CCR9 and alpha4-beta7 functionally addresses the T cell to the gut. After clonal expansion in the mesenteric lymph node, the activated T cell exits via the thoracic duct, enters circulation, and is recruited preferentially back to the small intestinal lamina propria where the initial antigen encounter occurred — precisely where its effector function is needed.
Without adequate retinoic acid in the dendritic cell's local environment, the gut-homing imprinting fails. T cells activated against gut pathogens do not return to the gut to fight them. This is a beautiful concrete molecular mechanism behind the older epidemiologic observation that Vitamin A deficient children get more diarrheal disease — their adaptive immune cells literally lose the address tags that would send them to the gut.
B-Cell Class Switching to Mucosal IgA
Retinoic acid also drives B-cell class switching toward the IgA isotype — the dominant antibody class secreted into mucosal surfaces. Secretory IgA dimers are secreted across the gut, airway, lacrimal, salivary, and mammary epithelium and provide the antigen-specific arm of mucosal immunity, complementing the non-specific epithelial barrier and antimicrobial peptides.
The class-switch recombination event that converts a B cell from producing IgM to producing IgA requires both TGF-beta and retinoic acid co-signals. Without adequate Vitamin A, mucosal IgA production drops — deficient children have measurably lower secretory IgA in saliva, breast milk, and intestinal washings, even when they have otherwise intact humoral immunity for systemic IgG responses.
The clinical relevance: breastfeeding mothers in deficient populations transmit fewer protective antibodies to their nursing infants. The WHO postpartum 200,000 IU Vitamin A dose for lactating mothers is intended to address this — it raises maternal Vitamin A status enough to support normal breast-milk IgA content, transferring measurable protection against gastrointestinal infection to the infant.
The WHO Measles Protocol (2×200,000 IU)
Measles is the most dramatic clinical demonstration of the Vitamin A immune connection. Measles infection itself depletes Vitamin A stores rapidly (the virus accelerates retinol turnover and the febrile illness causes anorexia and reduced intake). A child who was marginally deficient at the start of a measles infection can become severely deficient within days, and that deficiency in turn dramatically increases the risk of dying from measles complications — bacterial pneumonia superinfection, severe diarrhea with dehydration, encephalitis, or measles-associated keratomalacia and permanent blindness.
The Hussey and Klein 1990 NEJM trial established the modern WHO protocol. 189 South African children hospitalized with severe measles were randomized to two doses of 200,000 IU oral Vitamin A on consecutive days, or placebo. Results:
- Mortality was reduced by approximately 50% in the Vitamin A group
- Risk of severe complications (croup, pneumonia, diarrhea) was reduced
- Time to recovery was shorter
- Safety profile was excellent — no acute hypervitaminosis A despite the high dose
The WHO formally adopted the 2×200,000 IU protocol for measles management in all measles-endemic areas. The recommendation is to give the doses on two consecutive days, regardless of baseline Vitamin A status, to any child with measles in a setting where deficiency may be present. Cost is approximately 5 US cents per dose. This is one of the most cost-effective single interventions in global pediatric infectious disease.
The relevance to other viral infections has been studied less extensively. There is suggestive evidence for benefit in severe respiratory syncytial virus infection in deficient children, and Vitamin A supplementation has been part of the WHO RSV management guideline in deficient populations. For HIV mother-to-child transmission, results have been mixed and Vitamin A is no longer a primary intervention in that setting.
Respiratory Infections and Pneumonia
Pneumonia is the leading cause of death in children under five worldwide, killing approximately 700,000 children per year. A substantial fraction of this mortality is concentrated in populations with significant Vitamin A deficiency.
The Cochrane meta-analysis of Vitamin A supplementation for childhood mortality (Imdad et al. 2017) found that biannual high-dose Vitamin A reduced pneumonia mortality by approximately 27% in deficient populations. The effect is mechanistically explained by the mucosal-barrier integrity, restored ciliary function, mucus production, and antimicrobial peptide synthesis discussed above.
For adults in the developed world, the question of Vitamin A and respiratory infection is more nuanced. Adults with frankly low serum retinol (less than 0.7 µmol/L) clearly benefit from repletion in terms of reduced infection susceptibility. Adults with adequate baseline Vitamin A status do not appear to benefit from supraphysiologic dosing for infection prevention — the relationship is more like a step-function than a dose-response. Repletion of deficiency helps; pushing already-adequate intake higher does not.
The exception is patients with documented malabsorption (cystic fibrosis, advanced Crohn's disease, post-bariatric surgery), who often have subclinical Vitamin A deficiency despite normal dietary intake and may benefit from targeted supplementation as part of management of their increased infection susceptibility. For more on respiratory infection management, see our Pneumonia page.
Diarrheal Disease and Gut Barrier
Diarrhea is the second leading cause of childhood mortality globally (after pneumonia). Vitamin A's gut-barrier and mucosal-IgA effects translate to a meaningful reduction in diarrhea mortality in supplementation trials — the Imdad Cochrane meta-analysis found 32% reduction in diarrhea-specific mortality with biannual Vitamin A supplementation in deficient populations.
The gut-barrier mechanism is twofold:
- Structural integrity — retinoic acid maintains the goblet cells that produce the protective mucin layer (Muc2 is the dominant gel-forming mucin in the colon, Muc5AC in the small intestine), maintains tight junction proteins (claudins, occludin, ZO-1) that prevent paracellular translocation, and supports the antimicrobial peptide-producing Paneth cells in small-intestinal crypts
- Adaptive immunity addressed to the gut — the CCR9 / alpha4-beta7 imprinting of T cells and the IgA class switching of B cells both depend on retinoic acid as discussed above. Even when a Vitamin A deficient child mounts an immune response to a gut pathogen, that response is poorly directed to the gut tissue.
The clinical implication for adult patients is that any condition associated with chronic diarrhea (inflammatory bowel disease, SIBO, post-infectious irritable bowel) should prompt assessment of fat-soluble vitamin status, including Vitamin A. Treating the gut condition without addressing the secondary nutrient deficiency is incomplete.
Adult Immune Applications
For adult patients in the developed world, the Vitamin-A-and-immunity story plays out differently than in the deficient pediatric population. Most adults are not Vitamin A deficient, and supraphysiologic supplementation does not provide additive immune benefit. The relevant applications are concentrated in specific clinical contexts:
- Inflammatory bowel disease (Crohn's, ulcerative colitis) — both fat malabsorption and intestinal inflammation produce Vitamin A deficiency in 20-30% of patients. Repletion to normal serum retinol restores mucosal integrity and may reduce flare frequency. Typical regimen: 5,000-10,000 IU/day retinyl palmitate or 1 tsp cod liver oil daily, monitored with serum retinol every 6-12 months.
- Cystic fibrosis — routine Vitamin A supplementation is part of standard CF care due to pancreatic insufficiency-driven fat malabsorption. Liquid water-soluble Vitamin A preparations are typically used. Dosing follows CF Foundation guidelines based on age.
- Bariatric surgery — gastric bypass and duodenal switch procedures dramatically reduce fat-soluble vitamin absorption. Lifelong Vitamin A supplementation (10,000 IU/day or equivalent) is required, with periodic monitoring.
- Chronic kidney disease — counterintuitively, advanced CKD patients can have elevated serum retinol due to impaired renal clearance of retinol-binding protein. Supplementation should be conservative in advanced CKD.
- Recurrent respiratory infection in adults — check serum retinol, zinc, vitamin D, and screen for fat malabsorption. Repletion if deficient produces clinical benefit; supraphysiologic dosing in adequate adults does not.
Cautions (Including the Negative Tuberculosis Signal)
- Teratogenicity in pregnancy — the most consequential warning, repeated across every Vitamin A page. Preformed retinol above 3,000 mcg RAE/day in pregnancy is associated with fetal malformations of the central nervous system, face, ears, and heart. Pregnant women should avoid high-dose retinol supplements, limit beef liver to no more than one small serving per week, and never use isotretinoin or any oral retinoid drug.
- Tuberculosis — the negative supplementation signal — a notable exception to the "more Vitamin A reduces infection" pattern. Some clinical trials of high-dose Vitamin A in pulmonary tuberculosis patients have shown no benefit or even potential harm (faster sputum culture conversion in placebo arm in one trial). The proposed mechanism is that Mycobacterium tuberculosis requires intracellular cholesterol metabolism, and retinoic acid may inadvertently support pathogen lipid metabolism in addition to host immunity. High-dose Vitamin A is not recommended as adjunct TB therapy.
- HIV infection — early enthusiasm for Vitamin A as part of HIV management has cooled. The ZVITAMBO trial in Zimbabwe found that postpartum maternal Vitamin A supplementation in HIV-positive women may have increased mother-to-child transmission risk. Current WHO guidance does not recommend Vitamin A as a primary HIV intervention.
- Chronic high-dose toxicity — sustained intake >10,000 IU/day of preformed retinol can produce hepatotoxicity, alopecia, bone loss, and increased fracture risk. Beta-carotene does not carry this risk because of feedback regulation of conversion.
- Beta-carotene in smokers — high-dose isolated beta-carotene (20-30 mg/day) increases lung cancer risk in current and former heavy smokers per the ATBC and CARET trials. Food-source beta-carotene is safe; isolated high-dose supplements are not for this population.
- Drug interactions — orlistat, cholestyramine, mineral oil, and other fat-malabsorption drugs reduce Vitamin A absorption. Anticonvulsants (phenytoin, phenobarbital) accelerate Vitamin A catabolism and can deplete stores with chronic use.
Key Research Papers
- Mellanby E, Green HN (1928). Vitamin A as an anti-infective agent. British Medical Journal. — PubMed
- Sommer A et al. (1986). Impact of vitamin A supplementation on childhood mortality. A randomised controlled community trial. The Lancet. — PubMed
- Hussey GD, Klein M (1990). A randomized, controlled trial of vitamin A in children with severe measles. NEJM. — PubMed
- Imdad A et al. (2017). Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database. — PubMed
- Mucida D et al. (2007). Reciprocal TH17 and regulatory T cell differentiation mediated by retinoic acid. Science. — PubMed
- Iwata M et al. (2004). Retinoic acid imprints gut-homing specificity on T cells. Immunity. — PubMed
- Mora JR et al. (2006). Generation of gut-homing IgA-secreting B cells by intestinal dendritic cells. Science. — PubMed
- WHO (2011). Guideline: Vitamin A supplementation in infants and children 6-59 months of age. — PubMed
- Coutsoudis A et al. (1999). Randomized trial testing the effect of vitamin A supplementation on pregnancy outcomes and early mother-to-child HIV transmission in Durban, South Africa. AIDS. — PubMed
- Hanekom WA et al. (1997). Vitamin A status and therapy in childhood pulmonary tuberculosis. Journal of Pediatrics. — PubMed
- Stephensen CB (2001). Vitamin A, infection, and immune function. Annual Review of Nutrition. — PubMed
- Ross AC (2012). Vitamin A and retinoic acid in T cell-related immunity. American Journal of Clinical Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Vitamin A measles mortality
- PubMed: Retinoic acid Th17/Treg
- PubMed: RA gut-homing imprinting
- PubMed: Vitamin A pneumonia/diarrhea mortality
- PubMed: IgA class switching
Connections
- Vitamin A Overview
- Vitamin A Benefits Hub
- Vitamin A for Vision
- Vitamin A for Skin
- Beta-Carotene vs Preformed
- Immune Boosting
- Vitamin D3 (RXR Partner)
- Vitamin C
- Zinc (RBP Synthesis)
- Pneumonia
- Crohn's Disease
- Celiac Disease
- Organ Meats (Beef Liver)
- Omega-3 Fatty Acids
- All Vitamins