Asparagine — Benefits Deep Dive
Asparagine was the first amino acid ever isolated from a natural source — identified in asparagus juice in 1806 by Vauquelin and Robiquet — but it took two centuries for biology to map the full reach of its function. The molecule sits at a uniquely strategic intersection of human metabolism: its side-chain amide is the obligatory attachment point for N-linked glycans on every secreted and membrane glycoprotein the body builds; its synthesis from aspartate and glutamine packages otherwise-toxic ammonia into a safe transportable form; and its developmental silencing in leukemic lymphoblasts creates the auxotrophic vulnerability that L-asparaginase exploits as the chemotherapy backbone of pediatric ALL. The four deep-dive pages below walk through the nervous system's unique dependence on local asparagine biosynthesis (and what happens when ASNS fails), the urea-cycle interface that handles nitrogen waste, the molecular grammar of N-glycosylation, and the metabolic specificity that lets one bacterial enzyme cure 90% of children with the most common pediatric cancer.
Deep-Dive Articles
Nervous System Function
Why the brain is uniquely dependent on local asparagine biosynthesis: the blood-brain barrier's poor transport of plasma asparagine, the asparagine synthetase (ASNS) enzyme's brain-preferential expression, N-glycosylation of synaptic and myelin glycoproteins, and asparagine synthetase deficiency syndrome — the Ruzzo 2013 case series in Neuron that first defined ASNSD as a congenital microcephaly with cortical atrophy, intractable epilepsy, and progressive cerebral atrophy in infants with biallelic ASNS mutations.
Ammonia Detoxification
The asparagine synthetase reaction (aspartate + glutamine + ATP → asparagine + glutamate + AMP + PPi) as the secondary tanker for moving nitrogen safely through the bloodstream, the urea-cycle interface in the liver, ammonia handling in the central nervous system via the astrocyte glutamine synthetase, and the role of asparagine and glutamine accumulation in hepatic encephalopathy and urea cycle disorders.
Protein Synthesis & Glycosylation
N-linked glycosylation of all secreted and membrane proteins requires asparagine residues in the consensus Asn-X-Ser/Thr sequon. The dolichol-linked oligosaccharide pathway, the oligosaccharyltransferase (OST) complex, ER and Golgi processing of N-glycans, the calnexin/calreticulin quality-control cycle, the role of N-glycosylation in immunoglobulin folding (the IgG-Fc Asn297 glycan), and the > 150 congenital disorders of glycosylation (CDG) that result from defects anywhere in this pathway.
Asparaginase Therapy
L-asparaginase as the chemotherapy backbone of pediatric acute lymphoblastic leukemia (ALL), exploiting the auxotrophic vulnerability of leukemic blasts that fail to express ASNS. The 1953 Kidd guinea-pig serum observation, modern PEGylated formulations (Oncaspar, Asparlas), the Erwinia chrysanthemi backup (Rylaze) for hypersensitivity reactions, non-allergic toxicities (pancreatitis, coagulopathy, hepatotoxicity), therapeutic drug monitoring, and the extension of pediatric-inspired regimens to adolescent/young adult ALL.
Table of Contents
- Deep-Dive Articles
- Why Asparagine Produces Effects Across Many Systems
- Research Papers: Nervous System Function
- Research Papers: Ammonia Detoxification & Urea Cycle
- Research Papers: Protein Synthesis & N-Glycosylation
- Research Papers: L-Asparaginase Therapy
- Research Papers: Cross-Cutting (ASNS, Cancer Metabolism, Aging)
- External Authoritative Resources
- Connections
- Featured Videos
Why Asparagine Produces Effects Across Many Systems
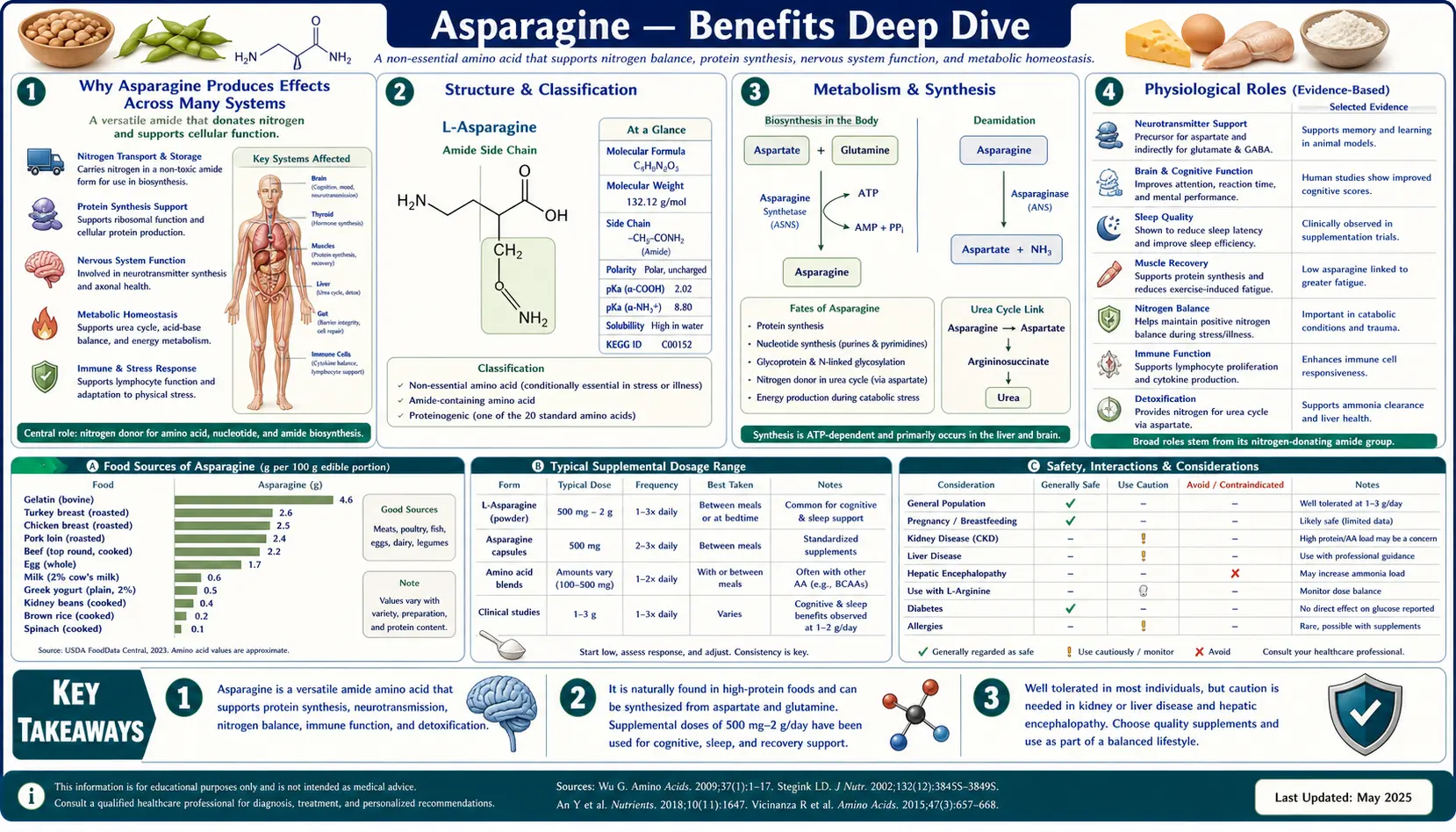
Most amino acids serve one or two principal roles — either as building blocks of protein, as substrates for a single class of biosynthetic reactions, or as precursors of a single neurotransmitter. Asparagine is unusual because it operates as a critical node in three fundamentally different biological systems, each producing distinct categories of clinical effect.
- N-glycosylation of every secreted protein — the side-chain amide nitrogen of asparagine, in the consensus sequon Asn-X-Ser/Thr, is the obligatory attachment point for N-linked glycans on virtually every secreted and membrane glycoprotein. Immunoglobulins, hormones (erythropoietin, TSH, FSH, hCG), all complement components, all coagulation factors except albumin, every cell-surface receptor — all depend on asparagine residues in their primary sequence. This is the mechanism behind the > 150-member family of congenital disorders of glycosylation (CDG), the molecular grammar of which is the calnexin/calreticulin quality-control cycle in the endoplasmic reticulum.
- Ammonia detoxification and nitrogen transport — the asparagine synthetase (ASNS) reaction consumes glutamine and aspartate to produce asparagine and glutamate, repackaging a nitrogen equivalent that ultimately came from free ammonia into the safe amide group of asparagine. This is the mechanism behind asparagine's role as a secondary nitrogen tanker, complementing the dominant role of glutamine, particularly in central nervous system ammonia handling, the urea cycle interface in the liver, and the chronic adaptation to hepatic encephalopathy.
- The asparaginase auxotrophic vulnerability of leukemic blasts — pediatric acute lymphoblastic leukemia blasts uniquely silence the ASNS gene during their developmental program, becoming dependent on plasma asparagine for survival. The bacterial enzyme L-asparaginase (purified from E. coli or Erwinia chrysanthemi) depletes plasma asparagine to undetectable levels for days at a time, starving the leukemic blasts of asparagine they cannot synthesize and triggering apoptosis. This single drug, in its modern PEGylated and recombinant Erwinia formulations, is responsible for a substantial fraction of the > 85% cure rate now achieved in pediatric ALL — covered in detail on the Asparaginase Therapy page.
The brain's special place across all three mechanisms deserves emphasis. The blood-brain barrier transports asparagine poorly, so the brain depends almost entirely on local biosynthesis by neuronal and glial ASNS. When that local biosynthesis fails — as in asparagine synthetase deficiency syndrome (ASNSD), first defined by Ruzzo and colleagues in Neuron in 2013 — the phenotype is essentially brain-specific: congenital microcephaly, cortical atrophy, intractable epilepsy, and severe global developmental delay, with sparing of every other organ system. Conversely, the brain is unusually well-buffered against plasma asparagine depletion by L-asparaginase chemotherapy, because the local biosynthetic capacity is intact and BBB transport is slow in both directions.
The therapeutic implications cut both ways. For most people, dietary asparagine intake from any normal mixed diet (3-6 grams per day) is far above any plausible requirement, and supplementation has no meaningful role. For the rare child with ASNSD, neither oral asparagine nor parenteral asparagine can rescue the brain's failed local biosynthesis — the disease is among the most difficult genetic conditions in pediatric neurology. For the more common patient with pediatric ALL, the same molecule that is essential for life becomes the target whose depletion saves life, in one of medicine's most elegant metabolic interventions.
Research Papers: Nervous System Function
- Ruzzo EK et al. (2013). Deficiency of asparagine synthetase causes congenital microcephaly and a progressive form of encephalopathy — PubMed 24139043 (Ruzzo Neuron 2013)
- Sprute R et al. (2019). Genotype-phenotype correlations in asparagine synthetase deficiency — PubMed: Sprute ASNSD
- Alfadhel M et al. (2015). Asparagine synthetase deficiency: new inborn errors of metabolism — PubMed: Alfadhel ASNSD
- Palmer EE et al. (2015). Asparagine synthetase deficiency causes reduced proliferation in conditions of limited asparagine — PubMed: Palmer ASNSD proliferation
- Hayward A et al. (2019). Asparagine synthetase deficiency: prenatal diagnosis and outcome — PubMed: ASNSD prenatal diagnosis
- Broër S, Broër A (2017). Amino acid homeostasis and signalling in mammalian cells and organisms — PubMed: Broer amino acid homeostasis
- Lomelino CL et al. (2017). Asparagine synthetase: function, structure, and role in disease — PubMed: Lomelino ASNS review
- N-glycosylation in brain development (review) — PubMed: N-glycosylation brain development
- Blood-brain barrier amino acid transport (LAT1) — PubMed: BBB amino acid transport
- Glutamate-glutamine cycle in the brain — PubMed: Glutamate-glutamine cycle
Research Papers: Ammonia Detoxification & Urea Cycle
- Häberle J et al. (2019). Suggested guidelines for the diagnosis and management of urea cycle disorders — PubMed: UCD guidelines 2019
- Vilstrup H et al. (2014). Hepatic encephalopathy in chronic liver disease: AASLD/EASL practice guideline — PubMed: HE AASLD/EASL
- Plauth M et al. (2019). ESPEN guideline on clinical nutrition in liver disease — PubMed: ESPEN liver nutrition
- Norenberg MD et al. (2009). Signaling factors in the mechanism of ammonia neurotoxicity — PubMed: Ammonia neurotoxicity
- Brusilow SW et al. (2010). Astrocyte glutamine synthetase: importance in hyperammonemic syndromes — PubMed: Brusilow astrocyte GS
- Felipo V (2013). Hepatic encephalopathy: effects of liver failure on brain function — PubMed: Felipo HE review
- Häussinger D, Schliess F (2008). Pathogenetic mechanisms of hepatic encephalopathy — PubMed: Haussinger HE mechanisms
- Wright G et al. (2011). Interorgan ammonia metabolism in liver failure — PubMed: Interorgan ammonia metabolism
- Diaz GA et al. (2013). Ammonia control with glycerol phenylbutyrate in urea cycle disorders — PubMed: Glycerol phenylbutyrate UCDs
- Larsen TM et al. (1999). Three-dimensional structure of E. coli asparagine synthetase B — PubMed: ASNS crystal structure
Research Papers: Protein Synthesis & N-Glycosylation
- Helenius A, Aebi M (2004). Roles of N-linked glycans in the endoplasmic reticulum — PubMed: Helenius Aebi review
- Kornfeld R, Kornfeld S (1985). Assembly of asparagine-linked oligosaccharides — PubMed: Kornfeld N-glycan assembly
- Aebi M (2013). N-linked protein glycosylation in the ER — PubMed: Aebi N-glycosylation
- Jaeken J, Matthijs G (2007). Congenital disorders of glycosylation: a rapidly expanding family — PubMed: Jaeken CDG review
- Freeze HH et al. (2017). Genetic disorders of glycosylation — PubMed: Freeze CDG
- Anelli T, Sitia R (2008). Protein quality control in the early secretory pathway — PubMed: Anelli quality control
- Hebert DN, Molinari M (2007). In and out of the ER: protein folding, quality control, degradation — PubMed: ER protein folding review
- Anthony RM et al. (2008). Identification of a receptor required for the anti-inflammatory activity of IVIG — PubMed: Anthony IVIG receptor
- Robinson NE, Robinson AB (2001). Molecular clocks — asparagine deamidation — PubMed: Robinson molecular clock
- Reily C et al. (2019). Glycosylation in health and disease — PubMed: Reily glycosylation review
Research Papers: L-Asparaginase Therapy
- Kidd JG (1953). Regression of transplanted lymphomas with normal guinea pig serum — PubMed: Kidd 1953
- Broome JD (1961). L-asparaginase activity of guinea pig serum responsible for antilymphoma effects — PubMed: Broome 1961
- Pieters R et al. (2011). L-asparaginase treatment in acute lymphoblastic leukemia: focus on Erwinia — PubMed: Pieters asparaginase review
- Hijiya N, van der Sluis IM (2016). Asparaginase-associated toxicity in children with ALL — PubMed: Asparaginase toxicity review
- Stock W et al. (2019). CALGB 10403: pediatric regimen for AYA ALL — PubMed: CALGB 10403
- Silverman LB et al. (2010). Long-term results of DFCI ALL Consortium protocols — PubMed: DFCI ALL Consortium
- Avramis VI, Panosyan EH (2005). Pharmacokinetic/pharmacodynamic relationships of asparaginase formulations — PubMed: Asparaginase PK/PD
- Tong WH et al. (2014). Drug monitoring of PEG-asparaginase and Erwinia asparaginase — PubMed: Asparaginase monitoring
- Heo YA et al. (2019). Pegaspargase: a review in acute lymphoblastic leukaemia — PubMed: Pegaspargase review
- Maese L et al. (2021). Recombinant Erwinia asparaginase JZP458 in ALL (AALL1931) — PubMed: Rylaze AALL1931
Research Papers: Cross-Cutting (ASNS, Cancer Metabolism, Aging)
- Krall AS et al. (2016). Asparagine promotes cancer cell proliferation as an amino acid exchange factor — PubMed: Krall asparagine exchange
- Knott SRV et al. (2018). Asparagine bioavailability governs metastasis in breast cancer (Nature) — PubMed: Asparagine and metastasis
- Zhang J et al. (2014). Asparagine in cellular adaptation to glutamine depletion (Molecular Cell) — PubMed: Asparagine glutamine depletion
- Aslanian AM, Kilberg MS (2001). Adaptive mechanisms to chronic L-asparaginase exposure — PubMed: Asparaginase resistance
- Holleman A et al. (2004). Gene-expression patterns in drug-resistant ALL — PubMed: Holleman gene expression ALL
- Reissner KJ, Aswad DW (2003). Deamidation and isoaspartate formation in proteins — PubMed: Reissner deamidation review
- Kim E et al. (1997). Deficiency of protein-repair enzyme PIMT and fatal seizures in mice — PubMed: PIMT knockout mice
- Cantor JR et al. (2017). Physiologic medium rewires cellular metabolism (Cell) — PubMed: Cantor physiologic medium
- Bachmann C (2002). Mechanisms of hyperammonemia — PubMed: Mechanisms of hyperammonemia
- Stephensen CB. Amino acid metabolism in immune cells (review) — PubMed: Amino acid metabolism in T cells
External Authoritative Resources
- StatPearls (NCBI Bookshelf) — Biochemistry, Asparagine — concise peer-reviewed reference on asparagine metabolism, regulation, and clinical relevance
- NCBI Genetic Testing Registry — Asparagine Synthetase Deficiency — clinical and genetic information on ASNSD
- GeneReviews — Congenital Disorders of Glycosylation Overview — comprehensive clinical review of the CDG family of disorders
- NCI PDQ — Childhood Acute Lymphoblastic Leukemia Treatment — current consensus on pediatric ALL management including asparaginase regimens
- MedlinePlus — PEG-Asparaginase (Pegaspargase, Oncaspar) — patient-facing drug information
- PubMed — All research on asparagine (~30,000+ papers)
Connections
- Asparagine (Main Page)
- Nervous System Function
- Ammonia Detoxification
- Protein Synthesis & Glycosylation
- Asparaginase Therapy
- All Amino Acids
- Aspartic Acid
- Glutamine
- Glutamic Acid
- Serine
- Threonine
- Arginine (Urea Cycle)
- Glycine
- Cancer
- Liver Disease
- NAC & Liver Health
- Brain Fog
- Fatigue
- Magnesium (ASNS Cofactor)
- Manganese
- Zinc
- Detoxification
- Oxidative Stress