Biotin for Hair, Skin & Nails — The Marketing Claim vs the Actual Evidence
Biotin is the most successfully marketed vitamin in the cosmetic supplement industry. American consumers spend an estimated $1.5 billion annually on biotin-containing hair, skin, and nail products. The trouble is that the marketing claim — that biotin grows hair, strengthens nails, and clears skin for everyone — rests on essentially zero randomized controlled trials in biotin-replete adults. The definitive Patel 2017 systematic review identified only 18 published studies of biotin for hair or nails. All 18 were either uncontrolled case series or studies in patients with documented biotin deficiency. This page walks through what the evidence does and does not support, identifies the populations where biotin supplementation has genuine value, and reframes biotin's real place in dermatology and trichology.
Table of Contents
- The Marketing Claim
- The Patel 2017 Systematic Review
- Hochman 1993 — The Brittle Nail Trial
- Where the Evidence Is Real: Deficiency Syndromes
- Where the Evidence Is Weak: Cosmetic Enhancement in Replete Adults
- What Dermatology's Real Evidence Base Looks Like
- Postpartum Hair Loss and Telogen Effluvium
- Alopecia Areata and Trichodynia
- Brittle Nail Syndrome — Evidence-Based Protocol
- Patient FAQ
- Cautions — Lab-Test Interference Comes First
- Key Research Papers
- Connections
- Featured Videos
The Marketing Claim
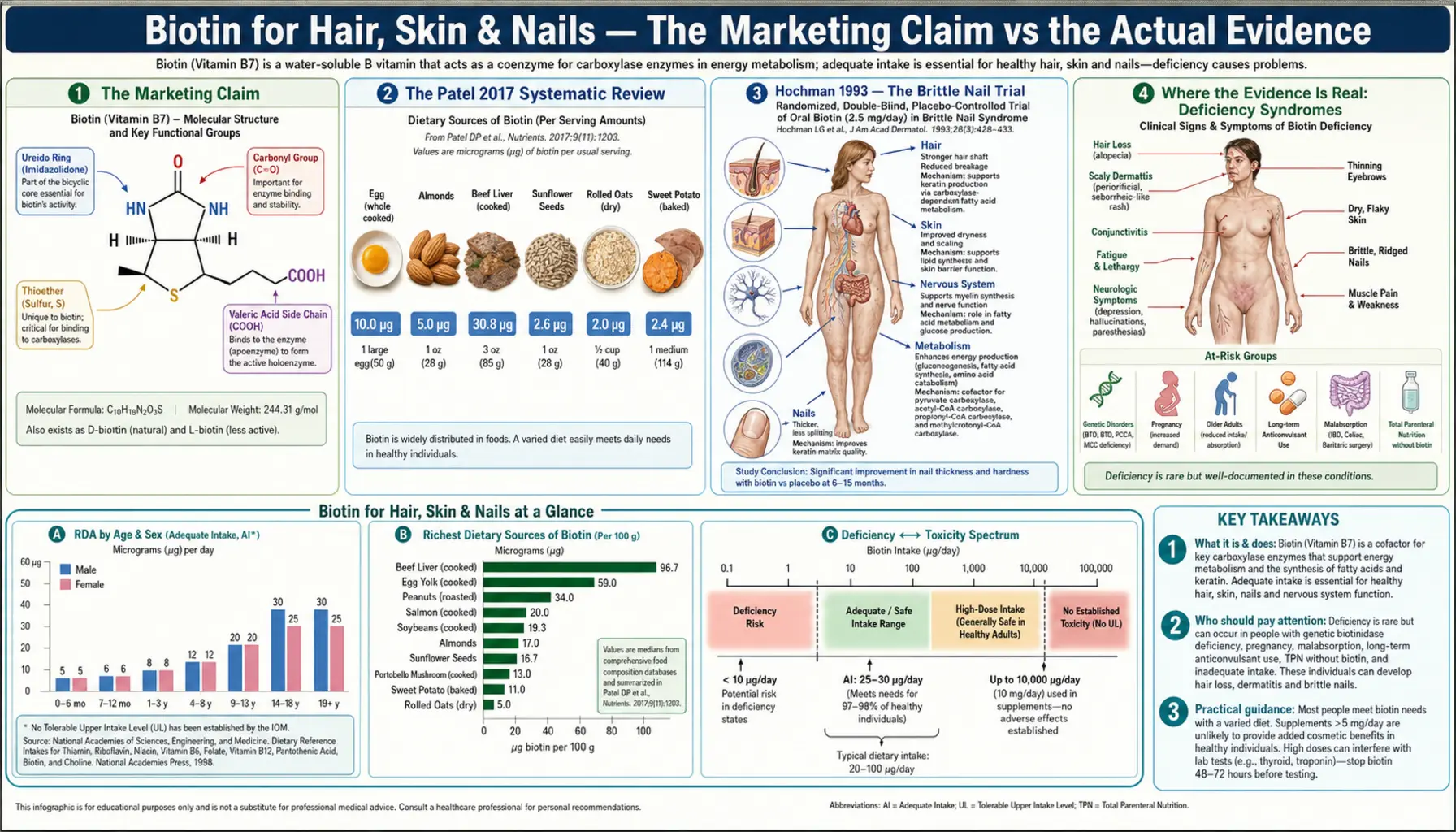
Walk down the supplement aisle of any drugstore in the United States and biotin dominates the hair-and-nail section. Bottles routinely contain 5,000 mcg or 10,000 mcg of biotin per capsule — 167× to 333× the Adequate Intake (AI) of 30 mcg/day for adults. The implied claim is universal: biotin grows hair, strengthens nails, and improves skin clarity in anyone who takes it.
This claim is the foundation of a market that the supplement industry estimates at roughly $1.5 billion per year in the United States alone for biotin-containing hair, skin, and nail products. Most consumers buying these products are not deficient in biotin. Clinical biotin deficiency is rare in industrialized countries with normal mixed diets — the AI is easily met by eggs, nuts, seeds, organ meats, salmon, and many vegetables; the gut microbiome contributes additional biotin; and the body recycles biotin efficiently via the enzyme biotinidase.
The dominant clinical question, then, is not whether biotin works at all for hair and nails — it clearly does in patients who are deficient — but whether biotin works in the population actually buying biotin supplements: women in their 30s, 40s, and 50s with normal dietary intake who notice some hair thinning or nail breakage and reach for the bottle that promises improvement.
The Patel 2017 Systematic Review
In 2017, Patel and colleagues published a systematic review in Skin Appendage Disorders titled "A Review of the Use of Biotin for Hair Loss." The paper systematically searched the literature for any published clinical evidence that biotin supplementation improves hair or nail outcomes.
The conclusion was striking. Patel identified 18 published case reports and case series of biotin used for hair or nail problems. Every single one of them fell into one of two categories:
- Patients with a documented underlying cause of biotin deficiency — biotinidase deficiency, holocarboxylase synthetase deficiency, valproic acid use, isotretinoin use, long-term anticonvulsant therapy, total parenteral nutrition without biotin supplementation, or chronic raw-egg-white consumption (avidin binding).
- Children with rare inherited disorders — primarily the carboxylase deficiencies described in detail on the Multiple Carboxylase Deficiency page.
Critically: zero of the 18 studies were randomized, placebo-controlled trials of biotin supplementation in healthy, biotin-replete adults seeking cosmetic enhancement of hair or nails. The published evidence base for the dominant consumer use case is empty.
The Patel review is the definitive answer to the question "is there RCT evidence that biotin grows hair in non-deficient adults?" The answer is no. There is also no RCT evidence that it doesn't — the studies simply have not been done. But the marketing claims rest on extrapolation from deficiency states to repletion states, which is a logically unjustified leap. Iron supplementation visibly cures the pallor of iron-deficiency anemia; that does not mean iron makes everyone's skin glow.
Hochman 1993 — The Brittle Nail Trial
The strongest individual piece of evidence that biotin can improve a cosmetic indication comes from a 1993 study by Hochman, Scher, and Meyerson published in Cutis. The trial enrolled 35 patients with brittle nail syndrome — a poorly understood condition characterized by thin, soft, fragile fingernails that split, peel, and break easily.
The protocol was uncontrolled — all 35 patients received 2.5 mg biotin per day for 6 months or longer. Outcomes were measured by patient self-report and clinical examination. The findings:
- 22 patients (63%) reported clinical improvement in nail firmness and reduced breakage
- Average nail-plate thickness increased by approximately 25%, measured by scanning electron microscopy in a subset of patients (this finding was independently confirmed by Colombo and colleagues in a separate electron microscopy study)
- Symptom improvement typically required 3-6 months of consistent daily dosing — not a quick fix
The Hochman trial has been cited thousands of times and remains the principal scientific support for biotin's use in brittle nail syndrome. Two earlier studies by Floersheim in 1989 reached similar conclusions in smaller cohorts.
What the Hochman finding does not support: that biotin grows hair, clears acne, plumps skin, reverses wrinkles, or strengthens already-healthy nails in adults without brittle nail syndrome. The finding is specific to one clinical condition (brittle nail syndrome), one dose (2.5 mg/day), one outcome (nail plate thickness), and one duration (6+ months). Generalizations beyond those parameters are not supported.
It is also worth noting that brittle nail syndrome is a real but heterogeneous condition. Some patients have iron deficiency, hypothyroidism, peripheral artery disease, or systemic illness underlying the brittleness. The Hochman cohort was not rigorously screened for these. The improvement seen in 63% of patients could reflect biotin's effect on a subset whose brittleness was driven by sub-clinical biotin insufficiency (an undocumented but plausible mechanism), or it could reflect non-specific effects of attention, supplementation in general, or natural waxing-and-waning of the condition. Without a placebo arm, attribution is uncertain.
Where the Evidence Is Real: Deficiency Syndromes
Biotin supplementation produces unambiguous, well-documented improvement in hair, skin, and nail symptoms in the following populations where deficiency or insufficiency is the underlying cause:
- Biotinidase deficiency — the inherited inability to recycle biotin from biotinylated proteins. Untreated, presents with alopecia (often total), seborrheic dermatitis, and seizures in infancy. Treatment with 5-20 mg biotin daily for life completely prevents these symptoms. Newborn screening for biotinidase deficiency was added to all 50 US state panels by 2013 specifically because the symptoms are devastating and the treatment is cheap and effective. See the Multiple Carboxylase Deficiency page for details.
- Holocarboxylase synthetase deficiency — the inability to attach biotin to apocarboxylase enzymes. Presents in infancy with skin rash and metabolic acidosis. Responds to high-dose biotin.
- Chronic raw-egg-white consumption — the avidin protein in raw egg white binds biotin with an affinity (Kd ~10^-15 M) that essentially makes it permanently unavailable. Body-builders and raw-food enthusiasts consuming multiple raw eggs daily for months can develop frank biotin deficiency with hair loss, scaly red rash, and conjunctivitis. Discontinuation of raw eggs + biotin replacement resolves symptoms within weeks.
- Long-term anticonvulsant therapy — carbamazepine, phenytoin, phenobarbital, and primidone accelerate biotin catabolism. Patients on multi-year anticonvulsant regimens can develop measurable biotin insufficiency that responds to supplementation.
- Isotretinoin (Accutane) therapy — case reports document nail brittleness and hair changes during isotretinoin courses that respond to concurrent biotin.
- Total parenteral nutrition (TPN) without biotin — before biotin became a standard TPN additive in the 1980s, patients on long-term TPN developed dermatitis and hair loss that resolved with biotin addition. Modern TPN formulations include biotin, so this is now historical.
- Severe inflammatory bowel disease, short bowel syndrome, gastric bypass — severely impaired intestinal absorption can reduce biotin status; supplementation is reasonable.
In each of these populations, biotin supplementation is correcting an actual deficiency. The evidence is solid. The mechanism is clear (replacing what's missing). The benefit is reproducible.
Where the Evidence Is Weak: Cosmetic Enhancement in Replete Adults
The cosmetic claim — that biotin grows thicker, longer, shinier hair in already-replete adults — rests on:
- Extrapolation from deficiency-correction trials (a logically unjustified leap, as noted above)
- Anecdotal patient reports and influencer testimonials
- The fact that biotin is essential for keratin synthesis (true but irrelevant: the rate-limiting step in keratin synthesis in a replete person is not biotin availability)
- One marine-protein supplement trial (Glynis 2012) that included biotin as one of many ingredients and could not isolate biotin's individual contribution
- The general placebo effect for any subjective cosmetic outcome over a multi-month period during which the person is paying more attention to their hair and may also have improved overall self-care
The honest framing of the cosmetic claim: in a person with normal biotin status, supplementing with 5,000-10,000 mcg biotin daily probably does nothing to their hair, skin, or nails. It is unlikely to harm them either (biotin is water-soluble and well-tolerated up to high doses), with one large exception: the lab-test interference problem that can mimic Graves' disease, hide active heart attacks, or hide ectopic pregnancies.
The cost of cosmetic biotin supplementation is therefore not its $15-50/month price tag — it is the small but real risk that the next time the supplement-taker presents to an emergency department with chest pain, their troponin assay will read falsely low and a heart attack will be missed. That risk is essentially zero for any individual patient on any individual day; it becomes meaningful when integrated across the tens of millions of Americans taking high-dose biotin supplements at any given time.
What Dermatology's Real Evidence Base Looks Like
A useful reality check is to compare biotin's evidence base to the evidence base for the interventions dermatologists actually use for hair loss and nail brittleness in clinical practice. The contrast is striking.
| Intervention | RCTs in non-deficient adults | Effect size for hair regrowth |
|---|---|---|
| Topical minoxidil (Rogaine) | Dozens | Moderate; demonstrable in 40-60% of androgenetic alopecia patients |
| Finasteride (oral, men) | Many large-scale | Substantial; halts progression in ~80%, regrowth in ~50% |
| Low-dose oral minoxidil | Multiple recent RCTs | Substantial; comparable to topical with better adherence |
| Low-level laser therapy (LLLT) | Several RCTs | Mild; statistically positive in well-conducted trials |
| Spironolactone (women) | Smaller but real | Moderate for androgen-driven female pattern hair loss |
| Biotin (oral, non-deficient adults) | Zero | Not established |
The American Academy of Dermatology does not recommend biotin supplementation for hair loss in non-deficient patients precisely because the evidence base is empty. Dr. Patricia Mills MD, Dr. Antonella Tosti (one of the world's most-cited trichologists), and many other clinical experts have published on this discrepancy between consumer perception and clinical reality.
Postpartum Hair Loss and Telogen Effluvium
Many women experience significant hair shedding 2-6 months postpartum — this is postpartum telogen effluvium, a synchronized shift of hair follicles into the resting (telogen) phase triggered by the postpartum drop in estrogen. The shedding peaks 3-4 months after delivery and generally resolves spontaneously by 12-18 months.
The intersection with biotin: pregnancy is one of the documented populations at risk of marginal biotin insufficiency. Up to 50% of pregnant women develop measurable biotin insufficiency by the third trimester based on urinary biotin metabolite excretion (Mock 1997). Whether this contributes to postpartum hair loss is unproven but plausible. Supplementation with 300-1000 mcg biotin daily during pregnancy and lactation is a reasonable practice with low risk and theoretical benefit.
Postpartum patients who present with hair shedding should be evaluated for the conditions that actually drive postpartum hair loss beyond the physiologic telogen effluvium: iron deficiency (extremely common after delivery and breastfeeding), vitamin D deficiency, thyroid dysfunction (postpartum thyroiditis affects ~5% of women), and zinc deficiency. Correcting these has much larger demonstrated effect than biotin supplementation.
Alopecia Areata and Trichodynia
Alopecia areata is an autoimmune condition that causes patchy hair loss. Case reports document occasional patients with alopecia areata who also have low biotin levels and respond to supplementation. The mechanism is unclear — whether biotin acts as an immune modulator or whether the deficiency is incidental to the autoimmunity.
For most alopecia areata patients, the evidence-based treatments are intralesional corticosteroid injections, topical corticosteroids, topical immunotherapy (diphenylcyclopropenone, squaric acid dibutylester), or for severe cases the newer JAK inhibitors (baricitinib, ritlecitinib). Biotin is not a recommended first-line treatment and should not be substituted for these.
However, a low-cost biotin trial (1-5 mg/day for 3-6 months) is reasonable as an adjunct alongside conventional treatment, particularly in patients with measured low serum biotin or those with one of the known biotin-depleting comorbidities.
Trichodynia — the sensation of scalp pain associated with hair shedding — has been associated in some case series with biotin and zinc insufficiency. Trial of supplementation is reasonable.
Brittle Nail Syndrome — Evidence-Based Protocol
This is the one consumer indication where biotin has at least an arguable evidence base (Hochman 1993 + Floersheim 1989 + Colombo electron microscopy). For patients with documented brittle nail syndrome (thin, soft, easily-split nails without underlying systemic disease):
- Dose: 2.5 mg (2500 mcg) per day — the Hochman dose
- Duration: Minimum 3-6 months before assessing response; many patients see no change for the first 2-3 months as new nail grows out from the matrix
- Adjuncts: Address potential confounders — check iron studies (ferritin should be >50 ng/mL), thyroid function, zinc, vitamin D. Use moisturizing nail oil daily (jojoba or vitamin E). Avoid acetone-based polish removers. Wear gloves for wet work.
- Lab-test interference: CRITICAL — instruct patient to discontinue biotin 3-5 days before any blood work and to mention biotin use to any clinician ordering tests. See the Lab-Test Interference page.
- Realistic expectations: About 60% of patients see meaningful improvement; 40% do not respond. Discontinue if no benefit after 6 months.
Patient FAQ
Q: Should I take biotin to grow my hair longer or thicker?
If you have normal dietary intake and no underlying medical condition, almost certainly no. The published RCT evidence in non-deficient adults is essentially zero. If you have a specific concern about hair loss, see a dermatologist for evaluation — the conditions that actually drive hair loss (androgenetic alopecia, iron deficiency, thyroid dysfunction, telogen effluvium, alopecia areata) have evidence-based treatments and biotin is not one of them.
Q: Should I take biotin for brittle nails?
For documented brittle nail syndrome, a trial of 2.5 mg/day for 3-6 months is reasonable based on Hochman 1993 and Floersheim 1989. Get baseline iron studies and thyroid function first — these conditions also cause nail brittleness and addressing them is higher-yield than biotin.
Q: Why does my collagen-and-biotin gummy claim to make my hair grow?
The supplement industry can make these claims under US dietary supplement law as long as they don't claim to treat a disease. Marketing language ("supports healthy hair") is structurally different from a medical claim. The published evidence does not support these claims in non-deficient adults.
Q: Is biotin dangerous?
At supplemental doses (up to 10,000 mcg or even higher), biotin itself is non-toxic — no upper limit has been established and no direct adverse effects have been reported. The serious issue is laboratory test interference (see that page) — biotin can cause your thyroid panel to falsely mimic Graves' disease and your troponin to falsely read low, potentially leading to a missed heart attack. Always inform your healthcare provider about biotin use.
Q: How long does it take for biotin to start working if I am deficient?
For deficiency symptoms (rash, hair loss, brittle nails), improvement typically begins within 2-4 weeks of starting replacement and continues over 3-6 months. Nail changes lag behind because the new nail must grow out from the matrix (a process that takes 4-6 months for a full fingernail replacement).
Q: Is the biotin in my hair shampoo doing anything?
Almost certainly not. Biotin is not appreciably absorbed through intact skin or scalp. The active ingredients in hair products that have any plausible effect are different (minoxidil, ketoconazole, caffeine-based products with limited evidence).
Cautions — Lab-Test Interference Comes First
- Laboratory test interference is the dominant safety issue. Supplemental doses of biotin (5,000 mcg and up, including the 2,500 mcg used in the Hochman brittle-nail protocol) interfere with streptavidin-biotin immunoassays used throughout hospital labs. The interference can falsely mimic Graves' disease (suppressed TSH, elevated free T4), can falsely lower troponin (potentially masking active myocardial infarction), can falsely elevate or lower hCG, parathyroid hormone, 25(OH)D, cortisol, sex hormones, and tumor markers. See the dedicated Lab-Test Interference page for details. Stop biotin at least 72 hours before any bloodwork at doses up to 10 mg; longer (5-7 days) for doses above 10 mg.
- Inform every clinician. Whenever any medical visit might generate lab work — primary care, endocrinology, cardiology, oncology, OB/GYN, the emergency department — spontaneously volunteer that you take biotin and at what dose. Do not wait to be asked.
- Avoid raw egg whites in combination with biotin marketing claims. If you are eating multiple raw eggs daily (smoothies, bodybuilding shakes), the avidin in raw egg white binds biotin so tightly that no oral biotin supplement will fix the resulting deficiency. Cook the eggs.
- Biotin does not replace dermatologic evaluation for hair loss. Significant hair loss warrants medical evaluation. Androgenetic alopecia, alopecia areata, telogen effluvium, thyroid disorders, iron deficiency, and many systemic illnesses can present with hair loss. Reaching for a biotin bottle delays appropriate diagnosis.
- Brittle nails can signal systemic disease. Brittle nail syndrome can be the presenting sign of iron deficiency anemia, hypothyroidism, Raynaud's phenomenon, peripheral artery disease, or eating disorders. Workup before reaching for a supplement.
- Pregnancy supplementation should stay modest. 300-1000 mcg daily during pregnancy is reasonable; 5,000+ mcg cosmetic doses during pregnancy unnecessarily increase the risk of lab-test interference during prenatal panels (false hCG, free thyroxine, etc.).
Key Research Papers
- Patel DP, Swink SM, Castelo-Soccio L (2017). A Review of the Use of Biotin for Hair Loss. Skin Appendage Disorders. — PubMed
- Hochman LG, Scher RK, Meyerson MS (1993). Brittle nails: response to daily biotin supplementation. Cutis. — PubMed
- Floersheim GL (1989). Treatment of brittle fingernails with biotin. Z Hautkr. — PubMed
- Colombo VE et al. (1990). Treatment of brittle fingernails and onychoschizia with biotin: scanning electron microscopy. J Am Acad Dermatol. — PubMed
- Trueb RM (2016). Serum biotin levels in women complaining of hair loss. Int J Trichology. — PubMed
- Soleymani T, Lo Sicco K, Shapiro J (2017). The Infatuation With Biotin Supplementation: Is There Truth Behind Its Rising Popularity? JAMA Dermatology. — PubMed
- Glynis A (2012). A double-blind, placebo-controlled study evaluating the efficacy of an oral supplement in women with self-perceived thinning hair. J Clin Aesthet Dermatol. — PubMed
- Almohanna HM et al. (2019). The Role of Vitamins and Minerals in Hair Loss: A Review. Dermatology and Therapy. — PubMed
- Mock DM, Stadler DD, Stratton SL, Mock NI (1997). Biotin status assessed longitudinally in pregnant women. J Nutr. — PubMed
- Lipner SR (2018). Rethinking biotin therapy for hair, nail, and skin disorders. J Am Acad Dermatol. — PubMed
- Walth CB, Wessman LL, Wipf A, Carina A, Hordinsky MK, Farah RS (2018). Response to: "Rethinking biotin therapy for hair, nail, and skin disorders." — PubMed
PubMed Topic Searches
- PubMed: biotin hair loss
- PubMed: biotin brittle nail
- PubMed: biotin seborrheic dermatitis
- PubMed: biotin telogen effluvium
- PubMed: biotin alopecia
Connections
- Vitamin B7 Overview
- Benefits Hub
- Lab-Test Interference
- Multiple Carboxylase Deficiency
- High-Dose MS Trials
- Biotin and Hair Health
- Hair Loss
- Alopecia
- Iron
- Zinc
- Collagen
- Vitamin D
- TSH (Thyroid)
- Ferritin
- Eggs
- All Vitamins