Alopecia
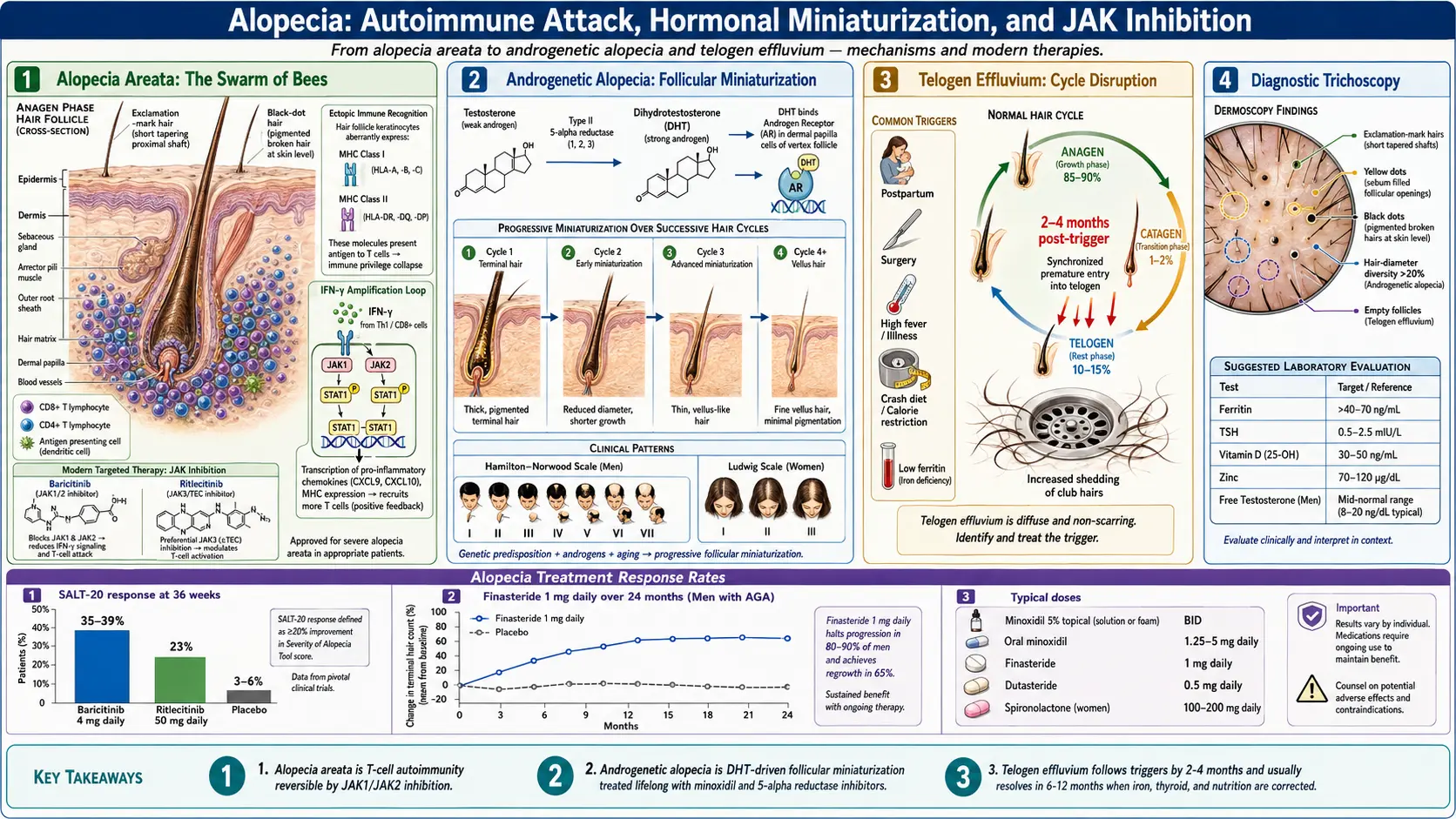
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
- Featured Videos
1. Overview
Alopecia is a broad medical term encompassing all forms of hair loss, ranging from autoimmune-mediated conditions to hormonally driven pattern baldness and scarring disorders. Hair loss can affect the scalp alone or the entire body, may be temporary or permanent, and results from a diverse array of genetic, autoimmune, hormonal, nutritional, and environmental causes. Alopecia is one of the most common dermatological complaints, affecting millions of people worldwide with significant impact on psychological well-being and quality of life.
Alopecia is classified into two major categories: non-scarring (non-cicatricial) alopecia, in which the hair follicle is preserved and hair regrowth is potentially achievable, and scarring (cicatricial) alopecia, in which the hair follicle is permanently destroyed by inflammation and replaced by fibrosis. The major forms of alopecia include:
- Alopecia areata (AA) — autoimmune-mediated patchy hair loss with preserved follicles
- Androgenetic alopecia (AGA) — hormone-dependent pattern hair loss (male-pattern and female-pattern baldness)
- Telogen effluvium — diffuse hair shedding due to metabolic stress, illness, or medications
- Anagen effluvium — acute hair loss from chemotherapy or radiation
- Traction alopecia — hair loss from chronic tension on hair follicles
- Trichotillomania — compulsive hair pulling disorder
- Scarring alopecias — lichen planopilaris, frontal fibrosing alopecia, central centrifugal cicatricial alopecia, discoid lupus
Recent advances in understanding the immunopathogenesis of alopecia areata have led to breakthrough treatments, including the FDA approval of the JAK inhibitor baricitinib (Olumiant) in 2022 as the first systemic therapy approved for severe alopecia areata, followed by ritlecitinib (Litfulo) and deuruxolitinib. Meanwhile, androgenetic alopecia remains the most prevalent form of hair loss, with established treatments including minoxidil, finasteride, dutasteride, and emerging therapies such as oral minoxidil and platelet-rich plasma.
2. Epidemiology
Alopecia areata has a lifetime incidence of approximately 2.1%, making it one of the most common autoimmune diseases. It affects both sexes equally and can occur at any age, though approximately 60% of patients experience their first episode before age 20. The prevalence varies by geographic region, with studies reporting rates of 0.1-0.2% point prevalence globally. Alopecia areata accounts for approximately 0.7-3.8% of dermatology clinic visits. The condition affects all races and ethnicities, with some studies suggesting slightly higher prevalence in African American and Hispanic populations.
Androgenetic alopecia is the most common cause of hair loss worldwide, affecting up to 80% of men and 50% of women by age 70. In men, the prevalence increases with age: approximately 30% by age 30, 50% by age 50, and 80% by age 70. The Hamilton-Norwood classification identifies seven stages of male-pattern baldness. Female-pattern hair loss (FPHL) affects approximately 12% of women by age 30, 25% by age 50, and up to 40% by age 70, classified using the Ludwig scale into three grades of severity.
Telogen effluvium is the second most common cause of hair loss seen by dermatologists, with a higher incidence in women. It frequently follows pregnancy (postpartum telogen effluvium affecting 40-50% of women), surgery, severe illness, crash dieting, or significant psychological stress, typically presenting 2-4 months after the triggering event.
3. Pathophysiology
Alopecia Areata: Autoimmune Mechanisms
Alopecia areata is a T-cell-mediated autoimmune disease that targets the hair follicle. Under normal conditions, the hair follicle bulb maintains immune privilege during the anagen (growth) phase, achieved through downregulation of MHC class I expression, local production of immunosuppressive molecules (TGF-beta, alpha-MSH, ACTH, IGF-1), and expression of Fas ligand that induces apoptosis of infiltrating lymphocytes. In alopecia areata, this immune privilege collapses, leading to ectopic expression of MHC class I and MHC class II molecules on the hair follicle epithelium. This exposes previously sequestered hair follicle-associated autoantigens — including trichohyalin, keratin 16, and melanocyte-associated antigens — to the adaptive immune system.
The resulting immune attack involves a dense "swarm of bees" pattern of CD8+ and CD4+ T lymphocytes surrounding the hair follicle bulb. These infiltrating T cells produce IFN-gamma, TNF-alpha, and IL-15, which further amplify the autoimmune response. The IFN-gamma-JAK-STAT signaling pathway is central to disease pathogenesis: IFN-gamma activates JAK1/JAK2 in follicular keratinocytes, leading to STAT1 phosphorylation and further MHC class I/II upregulation, creating a self-amplifying inflammatory loop. The NKG2D-activating receptor on CD8+ T cells recognizes MICA and ULBP stress ligands on hair follicle cells, contributing to targeted follicular destruction.
Androgenetic Alopecia: Hormonal Mechanisms
Androgenetic alopecia results from a genetically determined sensitivity of hair follicles to dihydrotestosterone (DHT), a potent androgen derived from testosterone by the enzyme 5-alpha reductase. There are two isoforms: type I 5-alpha reductase (present in sebaceous glands and skin) and type II 5-alpha reductase (predominant in hair follicles, prostate, and liver). DHT binds to androgen receptors in genetically susceptible hair follicles on the scalp vertex and frontal areas, triggering a process called follicular miniaturization. This involves progressive shortening of the anagen (growth) phase, elongation of the telogen (resting) phase, and gradual transformation of thick terminal hairs into thin, unpigmented vellus hairs.
At the molecular level, DHT-androgen receptor signaling upregulates TGF-beta1 and TGF-beta2 in dermal papilla cells, promotes DKK-1 (Dickkopf-1, a Wnt inhibitor) expression that suppresses hair follicle growth, and increases prostaglandin D2 (PGD2) production through prostaglandin D2 synthase overexpression. Elevated PGD2 acts through the GPR44 receptor to inhibit hair growth and promote follicular regression. Conversely, prostaglandin E2 (PGE2) and prostaglandin F2-alpha promote hair growth, creating an imbalance in prostaglandin signaling in balding scalp.
Hair Cycle Disruption in Telogen Effluvium
Normal hair growth follows a cycle of anagen (growth, 2-7 years, 85-90% of hairs), catagen (regression, 2-3 weeks, 1-2%), and telogen (rest/shedding, 2-4 months, 10-15%). In telogen effluvium, a physiological stressor causes a synchronized premature transition of a large proportion of anagen hairs into the telogen phase. After the typical 2-4 month telogen duration, these hairs are shed simultaneously, resulting in diffuse hair thinning. The trigger event — surgery, febrile illness, childbirth, crash dieting, severe emotional stress, or medication changes — typically precedes the onset of shedding by 2-4 months.
4. Etiology and Risk Factors
Alopecia Areata Risk Factors
- Genetic predisposition — strong HLA associations (HLA-DRB1*11:04, HLA-DQB1*03:01); first-degree relatives have a 5-fold increased risk; over 14 susceptibility loci identified by GWAS, including CTLA-4, IL-2/IL-21, and ULBP genes
- Personal or family history of autoimmune disease — thyroid disease (8-28%), vitiligo (4%), type 1 diabetes, celiac disease
- Atopic diathesis — atopic dermatitis, asthma, and allergic rhinitis are more prevalent in alopecia areata patients (up to 40%)
- Trisomy 21 (Down syndrome) — increased alopecia areata prevalence (6-9%) compared to general population
- Psychological stress — emotional trauma and stressful life events frequently precede disease onset
- Viral infections — Epstein-Barr virus and cytomegalovirus have been associated with alopecia areata onset or flares
Androgenetic Alopecia Risk Factors
- Genetic factors — polygenic inheritance; androgen receptor (AR) gene polymorphism on the X chromosome is the strongest genetic determinant; 20p11 locus associations
- Age — prevalence increases progressively with each decade of life
- Androgens — elevated DHT levels and increased 5-alpha reductase activity in susceptible follicles
- Polycystic ovary syndrome (PCOS) — hyperandrogenism is a major contributor to female-pattern hair loss in premenopausal women
- Metabolic syndrome — insulin resistance, obesity, and dyslipidemia are associated with earlier onset and greater severity
- Smoking — associated with increased risk and earlier onset of androgenetic alopecia
Telogen Effluvium Triggers
- Physiological stress — postpartum, surgery, severe illness, high fever, hemorrhage
- Nutritional deficiency — iron deficiency (with or without anemia), zinc deficiency, protein malnutrition, biotin deficiency, vitamin D deficiency
- Medications — beta-blockers, retinoids, anticonvulsants, anticoagulants, antithyroid drugs, oral contraceptive discontinuation
- Thyroid dysfunction — both hypothyroidism and hyperthyroidism
- Rapid weight loss — crash dieting, bariatric surgery
- Psychological stress — significant emotional trauma, bereavement, divorce
5. Clinical Presentation
Alopecia Areata
Alopecia areata classically presents as well-circumscribed, smooth, round or oval patches of non-scarring hair loss on the scalp, with no visible skin changes (no scaling, erythema, or scarring). The scalp skin within patches appears normal or slightly peach-colored. Characteristic findings include:
- Exclamation mark hairs — short, broken hairs (3-4 mm) that taper from a normal-width distal end to a narrowed, hypopigmented proximal end near the scalp; pathognomonic for active alopecia areata
- Positive hair pull test — gentle traction at the periphery of active patches yields easily extracted telogen and dystrophic anagen hairs
- Cadaverized (black dot) hairs — broken hairs at the scalp surface appearing as black dots
- White/gray hair sparing — non-pigmented hairs may be selectively spared, as the autoimmune attack preferentially targets melanocyte-associated antigens
- Nail changes — present in 10-66% of patients; include fine pitting (stippled or grid-like "sandpapered" nails), trachyonychia (rough, ridged nails), Beau's lines, onychorrhexis, and rarely red lunulae
Clinical subtypes include: alopecia totalis (complete loss of scalp hair), alopecia universalis (complete loss of all body hair including eyebrows, eyelashes, and body hair), ophiasis pattern (band-like loss along the temporal and occipital scalp margins, treatment-resistant), and sisaipho (inverse ophiasis) (hair loss sparing the scalp margins).
Androgenetic Alopecia
In men, androgenetic alopecia follows the Hamilton-Norwood classification, progressing from bitemporal recession (type II) through frontal thinning (type III-IV) to vertex (crown) involvement (type V-VI) and eventually confluent frontal-vertex baldness (type VII) with preservation of a horseshoe-shaped fringe of hair around the occipital and temporal regions. In women, the Ludwig classification describes diffuse thinning over the crown with preservation of the frontal hairline in three grades of severity. The Sinclair scale and Olsen pattern (Christmas-tree pattern of widening at the central part) are also used. Hair miniaturization results in replacement of thick terminal hairs with fine, short, unpigmented vellus hairs.
Telogen Effluvium
Telogen effluvium presents as diffuse, non-patterned hair thinning affecting the entire scalp, typically noticed as increased shedding during washing and brushing. Patients often report losing 200-300 or more hairs per day (compared to normal loss of 50-100 hairs daily). The hair pull test is diffusely positive. The condition usually presents 2-4 months after the triggering event and, in acute telogen effluvium, resolves spontaneously over 6-12 months once the trigger is removed. Chronic telogen effluvium (lasting >6 months) is more common in middle-aged women and may have no identifiable trigger.
6. Diagnosis
Clinical Assessment
The diagnosis of most forms of alopecia is primarily clinical, based on the pattern, distribution, and characteristics of hair loss. A thorough history should document onset, duration, progression, triggering events, family history of hair loss, medications, nutritional status, menstrual history (in women), and associated symptoms. Physical examination includes assessment of hair loss pattern, scalp skin quality (scarring vs. non-scarring), hair pull test, and examination of nails and body hair.
Trichoscopy (Dermoscopy of the Scalp)
Trichoscopy is an invaluable non-invasive diagnostic tool:
- Alopecia areata — exclamation mark hairs, black dots, yellow dots (follicular infundibula filled with keratinous material), short vellus hairs, tapered hairs, broken hairs; active disease shows clustered short vellus hairs
- Androgenetic alopecia — hair diameter diversity (>20% difference between thickest and thinnest hairs), miniaturized hairs, peripilar brown halo sign, yellow dots, thin wavy hairs
- Telogen effluvium — empty follicles, predominantly normal terminal hairs without miniaturization, upright regrowing hairs
Laboratory Evaluation
- Complete blood count — anemia screening
- Iron studies — serum ferritin (aim for >40-70 ng/mL for optimal hair growth), serum iron, TIBC
- Thyroid function tests — TSH, free T4, anti-TPO antibodies
- Vitamin D (25-hydroxyvitamin D)
- Zinc level
- Hormonal evaluation (in women with androgenetic alopecia) — total and free testosterone, DHEA-S, androstenedione, prolactin; rule out PCOS
- ANA — if scarring alopecia or lupus suspected
- RPR/VDRL — secondary syphilis (moth-eaten alopecia)
Scalp Biopsy
Scalp biopsy with horizontal and vertical sectioning is indicated when the diagnosis is uncertain or to differentiate scarring from non-scarring alopecia. In alopecia areata, biopsy shows peribulbar lymphocytic infiltrate ("swarm of bees" pattern) around anagen or early catagen follicles, increased catagen/telogen follicles, and miniaturized follicles, with preserved follicular architecture. In androgenetic alopecia, biopsy demonstrates progressive follicular miniaturization with an increased ratio of vellus to terminal hairs (>2:1) and absence of significant inflammation. Scarring alopecias show destruction of the follicular unit with fibrosis.
7. Treatment
Alopecia Areata: JAK Inhibitors
Baricitinib (Olumiant), a selective JAK1/JAK2 inhibitor, was approved by the FDA in June 2022 as the first systemic treatment for severe alopecia areata in adults. In the pivotal BRAVE-AA1 and BRAVE-AA2 phase 3 trials, baricitinib 4 mg daily achieved a Severity of Alopecia Tool (SALT) score of 20 or less (indicating 80% or greater scalp hair coverage) in approximately 35-39% of patients at 36 weeks, compared to 3-6% with placebo. Ritlecitinib (Litfulo), a selective JAK3/TEC family kinase inhibitor, was FDA-approved in June 2023 for alopecia areata in patients aged 12 years and older. In the ALLEGRO-2b/3 trial, ritlecitinib 50 mg daily achieved SALT 20 or less in approximately 23% of patients at 24 weeks. Deuruxolitinib (CTP-543), a selective JAK1/JAK2 inhibitor, demonstrated strong efficacy in phase 3 trials (THRIVE-AA1 and THRIVE-AA2) and is undergoing regulatory review.
Alopecia Areata: Conventional Therapies
- Intralesional corticosteroid injections — triamcinolone acetonide (5-10 mg/mL) injected into the dermis of affected patches every 4-6 weeks; first-line for limited (<50% scalp involvement) alopecia areata; regrowth in 60-70% of treated patches
- Topical corticosteroids — high-potency steroids (clobetasol propionate 0.05%) for limited disease, particularly in children
- Topical immunotherapy — diphenylcyclopropenone (DPCP) or squaric acid dibutylester (SADBE) applied to induce contact dermatitis and divert immune response; used for extensive disease; response rates of 50-70% but high relapse rates
- Topical minoxidil — 5% solution as adjunctive therapy to promote regrowth
- Oral corticosteroid pulse therapy — prednisone pulse (200 mg once weekly or 300 mg monthly) for rapidly progressive disease
- Methotrexate — 15-25 mg weekly, sometimes combined with low-dose prednisone; used as steroid-sparing agent for recalcitrant cases
Androgenetic Alopecia: Established Treatments
- Minoxidil (topical) — FDA-approved in 2% (women) and 5% (men and women) formulations; applied twice daily; promotes hair growth by prolonging anagen phase and increasing follicular size; mechanism involves potassium channel opening and increased blood flow; response in 30-40% of users; available as solution, foam, and 5% spray
- Oral minoxidil (low-dose) — increasingly used off-label at 1.25-5 mg daily for men and 0.625-2.5 mg daily for women; demonstrates superior efficacy to topical formulation with better compliance; requires monitoring for hypertrichosis, peripheral edema, and cardiovascular effects
- Finasteride (oral) — FDA-approved for men at 1 mg daily; selective type II 5-alpha reductase inhibitor that reduces serum DHT by approximately 70%; halts progression in 80-90% and promotes regrowth in 65% of men over 2 years; sexual side effects (decreased libido, erectile dysfunction) reported in 1-2% of users; not approved for women due to teratogenicity but used off-label in postmenopausal women at 2.5-5 mg
- Dutasteride (oral) — dual type I and type II 5-alpha reductase inhibitor; 0.5 mg daily; reduces serum DHT by approximately 90%; superior to finasteride in head-to-head trials; FDA-approved for benign prostatic hyperplasia but used off-label for AGA; similar side effect profile to finasteride
- Spironolactone — anti-androgen used in women at 100-200 mg daily for female-pattern hair loss; blocks androgen receptors and inhibits androgen synthesis; contraindicated in pregnancy
Surgical Treatment
- Hair transplantation — follicular unit transplantation (FUT/strip method) or follicular unit extraction (FUE); relocates DHT-resistant occipital follicles to balding areas; gold standard surgical treatment for androgenetic alopecia; results in 1-2 sessions; increasingly refined with robotic-assisted FUE
- Scalp micropigmentation — cosmetic tattooing to simulate the appearance of hair follicles on the scalp
Emerging and Adjunctive Therapies
- Platelet-rich plasma (PRP) — autologous concentrated platelets injected into the scalp; releases growth factors (PDGF, VEGF, TGF-beta) that stimulate hair follicle stem cells; typically 3-4 sessions monthly followed by maintenance every 3-6 months
- Low-level laser therapy (LLLT) — FDA-cleared devices (helmets, combs) using red light (650-670 nm); stimulates cellular metabolism in hair follicles; modest benefit as adjunctive treatment
- Clascoterone (topical androgen receptor inhibitor) — topical antiandrogen being investigated for androgenetic alopecia
8. Complications
- Psychological distress — depression, anxiety, social phobia, body dysmorphic symptoms, and diminished self-esteem; particularly severe in women, children, and patients with alopecia totalis/universalis
- Associated autoimmune diseases — alopecia areata patients have increased risk of thyroid disease, vitiligo, type 1 diabetes, inflammatory bowel disease, and other autoimmune conditions
- Nail dystrophy — present in up to 66% of alopecia areata patients; may persist even after scalp hair regrows
- Sun damage to exposed scalp — increased risk of sunburn and actinic damage on hairless scalp areas
- Ocular complications — loss of eyelashes and eyebrows in alopecia universalis increases risk of foreign body entry and eye irritation
- Treatment-related adverse effects — JAK inhibitor risks include increased infections, herpes zoster reactivation, venous thromboembolism, elevated cholesterol, and (with long-term use) potential malignancy risk; finasteride sexual side effects; minoxidil-induced hypertrichosis and cardiovascular effects
- Scarring and permanent hair loss — in cicatricial alopecias, delayed diagnosis and treatment leads to irreversible follicular destruction
- Traction alopecia scarring — chronic traction can progress from reversible to irreversible scarring alopecia if the causative hairstyle is not discontinued
9. Prognosis
Alopecia areata has a variable and often unpredictable course. In limited disease (fewer than 5 patches), spontaneous remission occurs in approximately 50% of patients within one year without treatment. However, lifetime recurrence rates are high, with 85% or more of patients experiencing at least one relapse. Approximately 5-10% of patients with alopecia areata progress to alopecia totalis or universalis. Poor prognostic factors include: onset before puberty, duration longer than one year, extensive involvement (>50% scalp), ophiasis pattern, nail involvement, atopy, and family history. With JAK inhibitor therapy, 35-40% of patients with severe disease achieve clinically meaningful regrowth, though relapse is common upon treatment discontinuation.
Androgenetic alopecia is a progressive, lifelong condition without spontaneous remission. Without treatment, hair loss continues gradually over decades. Finasteride halts progression in approximately 80-90% of men and produces visible regrowth in 65% over 2 years of continuous use; discontinuation leads to loss of benefits within 6-12 months. Minoxidil produces visible improvement in 30-40% of users but similarly requires continuous use. Hair transplantation provides permanent results in properly selected patients, as transplanted occipital follicles retain their DHT resistance.
Telogen effluvium generally has an excellent prognosis when the triggering cause is identified and addressed. Acute telogen effluvium typically resolves completely within 6-12 months. Chronic telogen effluvium may persist for years but rarely results in clinically significant permanent hair loss.
10. Prevention
- Alopecia areata — primary prevention is not possible; stress management and prompt treatment of flares may reduce severity; monitoring for associated autoimmune conditions (annual thyroid screening recommended)
- Androgenetic alopecia — early initiation of finasteride or minoxidil can significantly slow progression; genetic counseling may guide proactive treatment; maintaining healthy weight and metabolic parameters may delay onset
- Telogen effluvium — adequate nutrition (iron, zinc, vitamin D, protein), gradual weight loss rather than crash dieting, stress management, and medication review when possible
- Traction alopecia — avoid tight hairstyles (braids, ponytails, weaves, extensions) and chemical straighteners; early intervention prevents progression to scarring
- Nutritional optimization — maintain ferritin >40-70 ng/mL, adequate zinc, vitamin D (>30 ng/mL), biotin, and protein intake for optimal hair health
- Scalp sun protection — sunscreen, hats, or head coverings for exposed scalp areas
- Gentle hair care — minimize heat styling, chemical treatments, and excessive mechanical stress on hair
11. Recent Research and Advances
The landscape of alopecia treatment has been transformed by the development of JAK inhibitors, which represent the most significant therapeutic advance in dermatology in recent years. The approval of baricitinib (Olumiant) in 2022 and ritlecitinib (Litfulo) in 2023 for alopecia areata has provided effective systemic therapies for a condition that previously had no approved treatments. These agents work by blocking the JAK-STAT signaling pathway that drives the autoimmune attack on hair follicles. Long-term extension studies of baricitinib demonstrate sustained efficacy over 104 weeks of treatment, with continued improvement over time. Deuruxolitinib (JAK1/JAK2 inhibitor) has completed phase 3 trials with strong results and is anticipated for regulatory submission.
Research into topical JAK inhibitors for alopecia areata is expanding, with ruxolitinib cream and delgocitinib being investigated. Combination strategies pairing JAK inhibitors with phototherapy, PRP, or immunomodulators are being explored to enhance response rates and potentially allow lower drug doses.
In androgenetic alopecia, oral low-dose minoxidil (0.625-5 mg daily) has emerged as a major clinical advance, offering superior efficacy and improved compliance compared to topical formulations. Large retrospective studies and randomized trials have established its safety profile at low doses. Clascoterone (topical androgen receptor inhibitor) is being investigated for AGA after its approval for acne. Research into prostaglandin pathway modulators, Wnt pathway activators (e.g., SM04554/clascoterone), and hair follicle stem cell biology continues to expand potential therapeutic targets.
Hair follicle bioengineering and hair follicle organoid technology represent frontier approaches. Researchers have successfully generated hair follicle organoids from induced pluripotent stem cells (iPSCs) in the laboratory, and clinical applications are being developed for future cell-based hair restoration therapies. Exosome therapy and microneedling-enhanced drug delivery are emerging adjunctive approaches being investigated in clinical trials.
12. References & Research
Historical Background
Alopecia has been recognized since antiquity, with the term "alopecia" derived from the Greek "alopex" (fox), referencing the mangy shedding of a fox's fur. Cornelius Celsus (25 BCE – 50 CE) provided early descriptions of alopecia areata in his medical encyclopedia De Medicina. The first detailed clinical description of alopecia areata as a distinct entity was provided by the French dermatologist Raymond Sabouraud in the early 1900s, who differentiated it from tinea capitis. James Hamilton published his landmark classification of male-pattern baldness in 1951, later refined by O'Tar Norwood in 1975 into the Hamilton-Norwood scale still used today. The autoimmune basis of alopecia areata was established through the work of Rodney Dawber and others in the 1970s-1980s. The breakthrough discovery of the role of NKG2D+ CD8+ T cells and JAK-STAT signaling was published by Angela Christiano and colleagues at Columbia University in 2014, directly leading to the clinical development of JAK inhibitors for alopecia areata.
Key Research Papers
- Pratt CH, King LE Jr, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nat Rev Dis Primers. 2017;3:17011.
- Xing L, Dai Z, Jabbari A, et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nat Med. 2014;20(9):1043-1049.
- King B, Ohyama M, Kwon O, et al. Two phase 3 trials of baricitinib for alopecia areata. N Engl J Med. 2022;386(18):1687-1699.
- King B, Mostaghimi A, Shimomura Y, et al. Ritlecitinib for alopecia areata: a phase 2b/3 trial (ALLEGRO). Lancet. 2023;401(10387):1518-1529.
- Petukhova L, Duvic M, Hordinsky M, et al. Genome-wide association study in alopecia areata implicates both innate and adaptive immunity. Nature. 2010;466(7302):113-117.
- Kaufman KD, Olsen EA, Whiting D, et al. Finasteride in the treatment of men with androgenetic alopecia. J Am Acad Dermatol. 1998;39(4 Pt 1):578-589.
- Olsen EA, Dunlap FE, Funicella T, et al. A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. J Am Acad Dermatol. 2002;47(3):377-385.
- Messenger AG, McKillop J, Farrant P, McDonagh AJ, Sheraton M. British Association of Dermatologists' guidelines for the management of alopecia areata. Br J Dermatol. 2012;166(5):916-926.
- Gilhar A, Etzioni A, Paus R. Alopecia areata. N Engl J Med. 2012;366(16):1515-1525.
- Cranwell W, Sinclair R. Male androgenetic alopecia. Endotext. South Dartmouth: MDText.com; 2016. PMID:25905192
- Sinclair RD. Female pattern hair loss: a pilot study investigating combination therapy with low-dose oral minoxidil and spironolactone. Int J Dermatol. 2018;57(1):104-109.
- Strazzulla LC, Wang EHC, Avila L, et al. Alopecia areata: disease characteristics, clinical evaluation, and new perspectives on pathogenesis. J Am Acad Dermatol. 2018;78(1):1-12.
- Hamilton JB. Patterned loss of hair in man; types and incidence. Ann N Y Acad Sci. 1951;53(3):708-728.
- Garza LA, Liu Y, Yang Z, et al. Prostaglandin D2 inhibits hair growth and is elevated in bald scalp of men with androgenetic alopecia. Sci Transl Med. 2012;4(126):126ra34.
- Almohanna HM, Ahmed AA, Tsatalis JP, Tosti A. The role of vitamins and minerals in hair loss: a review. Dermatol Ther (Heidelb). 2019;9(1):51-70.
Research Papers
Curated PubMed topic searches of peer-reviewed literature on Alopecia. Each link opens a live PubMed query so you always see the most current studies.
- PubMed: Alopecia areata treatment
- PubMed: Minoxidil and finasteride
- PubMed: JAK inhibitors
- PubMed: Telogen effluvium
- PubMed: Platelet-rich plasma
- PubMed: Autoimmune pathogenesis
- PubMed: Iron and ferritin in hair loss
- PubMed: Vitamin D and alopecia
- PubMed: Frontal fibrosing alopecia
- PubMed: Hair transplantation
- PubMed: Thyroid and hair loss
- PubMed: Stress and hair loss
Connections
- Zinc
- Hair Loss
- Vitiligo
- Iron
- Stress Management
- Eczema
- Psoriasis
- Vitamin D3
- Biotin
- Anemia
- Celiac Disease
- Lupus
- Testosterone
- PCOS
- Insulin Resistance
- Acne
- Complete Blood Count