Biotin (Vitamin B7) Deficiency: Symptoms, Causes, and Recovery
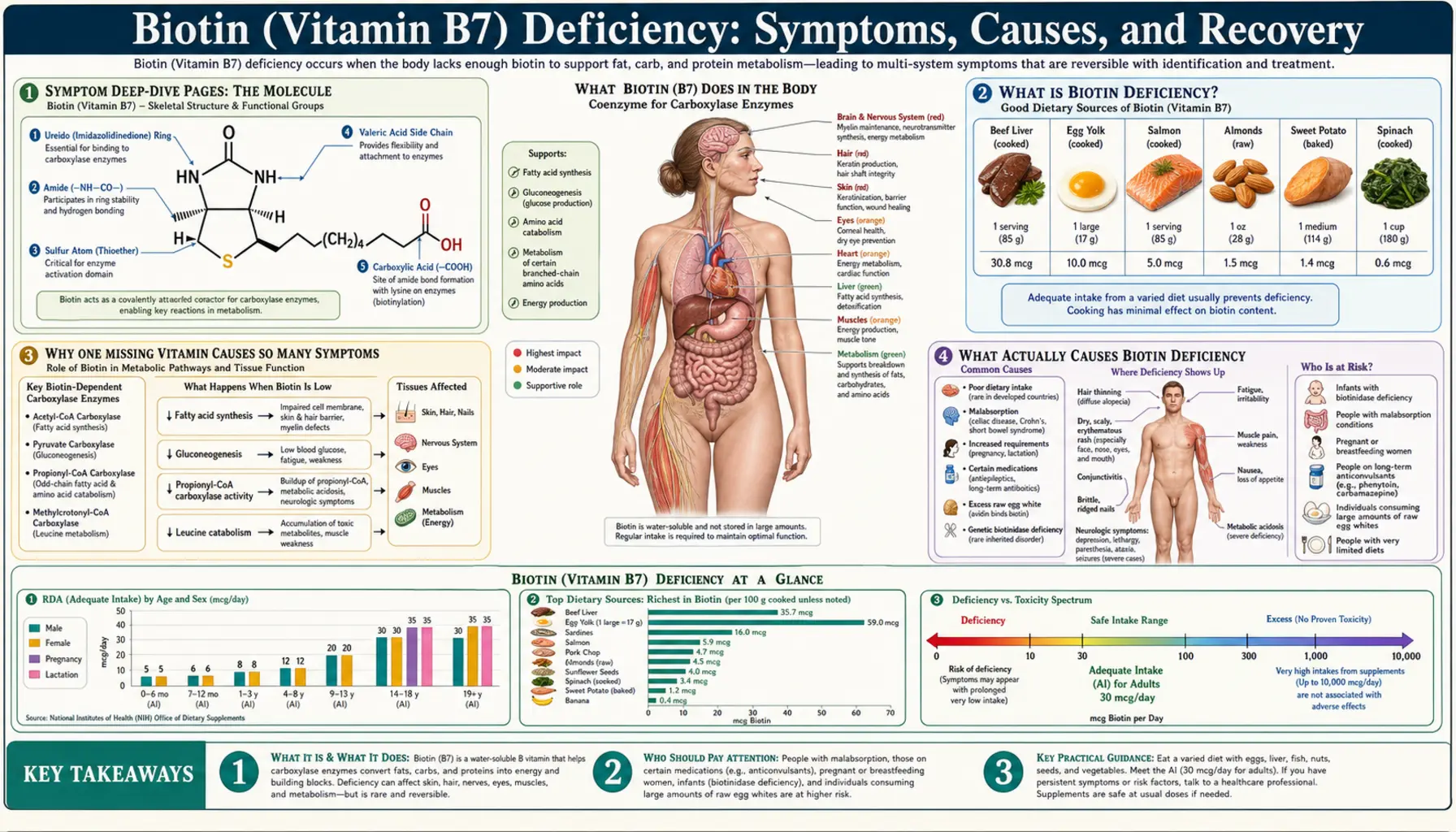
Biotin — vitamin B7, sometimes still called vitamin H — is a B vitamin your cells use to build fat, break down protein, and manage blood sugar. A true deficiency is genuinely uncommon, because biotin is found in many everyday foods and your gut bacteria make some as well. When it does happen, it leaves a recognizable fingerprint: thinning hair or hair loss, a scaly red rash that often rings the eyes, nose, and mouth, brittle splitting nails, and — in more severe or inherited cases — neurological symptoms such as deep tiredness, low mood, and tingling or numbness. The classic causes are unusual rather than ordinary: eating large amounts of raw egg white over time (a protein in it, avidin, locks onto biotin so the body cannot absorb it), an inherited enzyme problem called biotinidase deficiency that is now caught by newborn screening, long-term use of certain anti-seizure medicines, and prolonged intravenous feeding without added biotin. One honest point sits at the center of this page: because most people are not deficient, taking biotin supplements does not grow thicker hair or stronger nails in someone whose levels are already normal — the benefit only appears when there is a real shortage to correct. This hub explains what biotin deficiency is, why one missing vitamin produces such varied skin, hair, and nerve symptoms, what actually causes it, and how it is diagnosed and corrected — with deep-dive pages for each of the major symptoms.
Symptom Deep-Dive Pages
Hair Loss
Why a real biotin shortage can thin or shed hair, how this differs from the much more common causes of hair loss, and the honest truth about whether biotin supplements regrow hair in people who are not deficient.
Skin Rashes
The scaly, red, often itchy rash of biotin deficiency — classically ringing the eyes, nose, and mouth (periorificial) — what it looks like, why it forms, and the other skin conditions it can mimic.
Brittle Nails
How biotin deficiency can leave nails soft, thin, and prone to splitting and peeling — and why the evidence for biotin helping brittle nails applies mainly to people who actually lack it.
Neurological Symptoms
The lethargy, depression, and tingling or numbness (paresthesia) seen in more severe biotin deficiency, and why inherited biotinidase deficiency makes the nervous system especially vulnerable.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Biotin Deficiency?
- Why One Missing Vitamin Causes So Many Symptoms
- What Actually Causes Biotin Deficiency
- Who Is Most at Risk
- How Biotin Deficiency Is Diagnosed
- How Biotin Deficiency Is Corrected
- The Hair-and-Nail Supplement Myth
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Is Biotin Deficiency?
Biotin is one of the eight B vitamins. It is water-soluble (it dissolves in water rather than being stored in fat), so the body keeps only a modest reserve and relies on a steady supply. Biotin deficiency simply means the body does not have enough biotin to run the handful of essential reactions that depend on it. The vitamin has gone by several names — you may see it called vitamin B7, the older name vitamin H (from the German Haar und Haut, "hair and skin," reflecting the symptoms that first drew attention to it), or, in older biochemistry texts, coenzyme R.
The single most important thing to understand is that true biotin deficiency is uncommon. Biotin is present in a wide range of foods, the daily requirement is small, and bacteria living in the large intestine produce some biotin as well. For these reasons there is no defined Recommended Dietary Allowance (RDA) for biotin; instead, expert panels set an Adequate Intake (AI) of about 30 micrograms per day for adults, an amount most people reach without trying. Frank deficiency in an otherwise healthy, well-fed adult is rare enough that when a doctor sees it, they look hard for a specific reason — an inherited enzyme problem, an unusual diet, a medication, or a feeding tube without added biotin.
When biotin does run short, the picture is fairly characteristic. It typically builds up over weeks to months and shows up first in the fast-growing, high-turnover tissues — skin, hair, and nails — before the nervous system is affected:
- Hair — thinning, increased shedding, and in more advanced cases loss of hair from the scalp and even the eyebrows and eyelashes. (Deep dive: Hair Loss.)
- Skin — a dry, scaly, red rash that classically forms around the eyes, nose, and mouth (described as periorificial, meaning "around the openings"), sometimes with cracking at the corners of the mouth and an itchy, eczema-like appearance. (Deep dive: Skin Rashes.)
- Nails — soft, thin, brittle nails that split, peel, or break easily. (Deep dive: Brittle Nails.)
- Nervous system (more severe or inherited cases) — deep tiredness and lethargy, low mood or depression, and tingling or numbness in the hands and feet (paresthesia). In infants with inherited forms, far more serious problems — seizures, poor muscle tone, and developmental delay — can occur. (Deep dive: Neurological Symptoms.)
It is worth separating two very different situations that both fall under "biotin deficiency." The first is acquired deficiency in older children and adults — usually mild, slow, and tied to a specific cause such as a long-term raw-egg-white habit or anticonvulsant medication. The second is inherited deficiency, where a child is born with a faulty enzyme (most often biotinidase deficiency) that prevents the body from recycling its own biotin; this can cause severe illness in infancy and is the reason biotin status is now part of newborn screening in many countries. Both are covered below, because the symptoms overlap but the urgency and treatment differ greatly.
Why One Missing Vitamin Causes So Many Symptoms
It can seem strange that a shortage of one small molecule produces effects as different as a facial rash, falling hair, splitting nails, and tingling feet. The explanation is that biotin does not have one narrow job — it is a coenzyme, a helper molecule that a small family of critical enzymes cannot work without. Take biotin away and several core chemical assembly lines slow down at once, and the tissues that depend most heavily on those assembly lines complain first.
In everyday terms, biotin clips onto and activates a group of enzymes called carboxylases. There are five of them in humans, and together they sit at major crossroads of metabolism: building fatty acids (the raw material for healthy skin and the protective oils that keep skin and hair supple), breaking down certain amino acids from protein, and helping the body make new glucose to keep blood sugar steady. Lardy and colleagues first mapped these metabolic functions of biotin decades ago, and Said's modern reviews describe how central they remain. When biotin is in short supply, these carboxylases cannot be switched on properly, and two things follow.
First, the products these enzymes are supposed to make — especially certain fats — fall short. Skin and hair are built and maintained from fatty building blocks, so a slowdown in fat synthesis shows up as a scaly rash, fragile hair, and weak nails. This is why the earliest and most visible signs cluster in the skin, hair, and nails: these tissues renew themselves constantly and are unusually demanding of the very pathways biotin powers. Second, partly processed intermediates back up behind the stalled enzymes — one of them, 3-hydroxyisovaleric acid, spills into the urine and is actually used as an early laboratory marker of biotin shortage before any symptoms appear.
The nervous system enters the story when the deficiency is more severe or, especially, when it is inherited. Nerve cells are metabolically hungry and sensitive to disruptions in energy and amino-acid handling, so a deeper biotin shortfall produces lethargy, mood changes, and the pins-and-needles feeling of paresthesia. In inherited biotinidase deficiency the brain is particularly vulnerable because the body cannot recycle the biotin it already has, so the shortage can become profound — which is why untreated infants can develop seizures and lasting neurological damage.
The unifying idea to carry into the symptom pages is simple: biotin is a shared tool used by several essential enzymes, so one missing tool slows many jobs — and the busiest workshops (skin, hair, nails, and nerves) notice the shortage first.
What Actually Causes Biotin Deficiency
Because a normal diet easily supplies enough biotin, deficiency almost always traces back to a specific, identifiable cause rather than simply "not eating well." The recognized causes fall into a few clear groups.
- Large amounts of raw egg white — the classic cause. Raw egg white contains a protein called avidin that binds biotin extremely tightly and prevents the gut from absorbing it. Eating a few raw eggs is harmless, but consuming many raw egg whites every day for a long period (a habit seen historically in some bodybuilders and in people following unusual diets) can lock up enough biotin to cause deficiency. The phenomenon was first described almost a century ago and earned the memorable name "egg-white injury," later confirmed in humans by Scott. Crucially, cooking deactivates avidin — heat changes the protein's shape so it can no longer grab biotin — which is why cooked eggs are not only safe but are themselves a good source of biotin. (See the Eggs page.)
- Inherited biotinidase deficiency. Biotinidase is the enzyme that frees biotin from food and, just as importantly, recycles biotin within the body. Children born with little or no working biotinidase cannot reclaim their own biotin and become progressively deficient. Wolf's work on this condition is the reason newborn screening for it exists; caught early, it is treated simply and effectively with lifelong oral biotin, but if missed it can cause seizures, hearing and vision loss, and developmental delay. A related inherited problem, holocarboxylase synthetase deficiency, prevents biotin from being attached to its enzymes and presents even earlier in infancy.
- Long-term anticonvulsant (anti-seizure) medications. Several older anti-seizure drugs — including phenytoin, phenobarbital, primidone, and carbamazepine — can lower biotin status over time. They appear to do so by interfering with biotin absorption, accelerating its breakdown, and competing with it, so people on these medicines for years can drift toward marginal deficiency. (Valproate can also disturb biotin handling.)
- Prolonged intravenous feeding (total parenteral nutrition) without biotin. When someone is fed entirely through a vein for a long time and the nutrient mixture does not include biotin, deficiency can develop — a problem recognized in early TPN before biotin was routinely added. Modern parenteral formulas include biotin specifically to prevent this.
- Heavy, long-term alcohol use. Alcohol can impair the intestinal absorption of biotin and is associated with poorer biotin status, adding to the broader nutritional deficiencies common in chronic alcohol use.
- Pregnancy. Research by Mock and colleagues found that a surprising fraction of women develop marginal (mild, subclinical) biotin deficiency during otherwise normal pregnancy, likely from increased demand. This rarely causes obvious symptoms in the mother, but because biotin is important for normal development, it is an area of active study and a reason prenatal vitamins typically include biotin.
- Certain other situations. Severe, prolonged malnutrition; some malabsorption conditions affecting the gut; and a rare metabolic quirk that increases biotin breakdown have all been linked to low biotin. Smoking may modestly speed biotin breakdown as well.
A practical takeaway: if you are eating ordinary food (including any cooked eggs), are not on long-term anti-seizure medicine, are not living on raw egg whites, and were not flagged at birth, your odds of true biotin deficiency are very low. When deficiency is found, the most useful next question is always why — because fixing the cause matters as much as replacing the vitamin.
Who Is Most at Risk
Rather than the whole population, biotin deficiency concentrates in a handful of specific groups. Recognizing yourself (or a loved one) here is the main reason to take the possibility seriously.
- Newborns and infants with an inherited enzyme defect. This is the most important high-risk group. Babies with biotinidase deficiency or holocarboxylase synthetase deficiency can become severely ill in the first weeks to months of life. Newborn screening exists precisely to catch biotinidase deficiency before symptoms start; a positive screen is followed by confirmatory testing and, if needed, lifelong biotin.
- People taking anti-seizure medicines for years. Long-term users of phenytoin, phenobarbital, primidone, or carbamazepine drift toward lower biotin status and are the most common adult group with measurable depletion.
- Anyone regularly eating large amounts of raw egg white. Certain dietary trends, raw-food regimens, and old-style bodybuilding habits (raw eggs in shakes) put people at risk. The risk is dose- and time-dependent — it takes a lot of raw white, consumed regularly over a long period.
- People on long-term intravenous (parenteral) nutrition. Especially if the formula is not supplemented with biotin — though modern formulas usually are.
- People with heavy, chronic alcohol use. Both from impaired absorption and from the poor overall diet that often accompanies it.
- Pregnant women. At risk of marginal (mild) deficiency rather than the dramatic, symptomatic kind — one reason prenatal supplements contain biotin.
- People with significant intestinal malabsorption. Conditions that broadly impair nutrient uptake can include biotin among the affected vitamins.
If you do not fall into any of these categories, isolated thinning hair, a brittle nail, or a patch of dry skin is far more likely to come from something other than biotin deficiency — a point each symptom deep-dive page returns to honestly.
How Biotin Deficiency Is Diagnosed
Diagnosing biotin deficiency is less routine than checking, say, potassium or vitamin D, because the deficiency is uncommon and there is no single quick test on a standard panel. Diagnosis usually rests on the combination of a fitting clinical picture, a plausible cause, and specialized laboratory testing, with the response to biotin treatment often serving as the final confirmation.
- The clinical story. The pattern of a periorificial scaly rash, hair thinning or loss, and brittle nails — especially together, and especially alongside a known risk factor such as raw-egg-white intake, long-term anticonvulsants, or TPN — is what first raises suspicion. In infants, the screening result and early symptoms guide the work-up.
- Urinary 3-hydroxyisovaleric acid. Rather than measuring biotin in the blood (which is technically tricky and an unreliable marker of mild deficiency), the most sensitive early indicator is a rise in 3-hydroxyisovaleric acid in the urine. This compound builds up when one of the biotin-dependent enzymes is starved of biotin, so it climbs before symptoms appear and is the marker Mock's research used to detect even marginal deficiency.
- Blood biotin levels. Direct serum or plasma biotin can be measured but is considered insensitive for detecting marginal deficiency, so a "normal" blood biotin does not fully rule it out. It is more useful at the extremes.
- Tests for inherited forms. When an enzyme defect is suspected (notably in infants flagged by newborn screening), specific tests measure biotinidase enzyme activity in the blood, and genetic testing can confirm the diagnosis. This is essential because the inherited forms need lifelong treatment, not a short course.
- Supporting blood work. Routine panels such as a Comprehensive Metabolic Panel and a Complete Blood Count do not diagnose biotin deficiency, but they help a clinician look for other explanations for hair loss, rash, or fatigue (such as thyroid problems, iron deficiency, or zinc deficiency) that are far more common and must be considered.
One important and frequently overlooked caveat sits at the intersection of biotin and the lab: biotin supplements can interfere with many common blood tests. High-dose biotin (the kind in some over-the-counter "hair, skin, and nails" products) can throw off immunoassay-based tests — including some thyroid hormone, vitamin D, hormone, and even certain cardiac (troponin) tests — producing falsely high or falsely low results. Avery and others reviewed this for laboratory scientists, and regulators have warned about it. The practical advice: tell your doctor and the lab if you take biotin, and they may ask you to stop it for a few days before testing. This interference is the single most clinically relevant downside of biotin supplements in people who do not need them — covered further on the Vitamin B7 Toxicity page.
How Biotin Deficiency Is Corrected
The good news is that biotin deficiency — once correctly identified — responds well and often quickly to treatment. The guiding principles are: supply enough biotin, remove or manage the cause, and match the approach to whether the deficiency is acquired or inherited.
- Food first for everyday adequacy. For preventing deficiency and meeting the roughly 30 micrograms-per-day Adequate Intake, ordinary food is more than sufficient. Biotin is found in cooked eggs (especially the yolk), organ meats such as liver, salmon and other fish, meat, seeds and nuts, legumes, whole grains, and many vegetables. Because biotin is so widespread, a varied diet quietly covers the requirement.
- Removing the cause. Often the most effective single step. Stopping a heavy raw-egg-white habit (or simply cooking the eggs), reviewing long-term anticonvulsant therapy with the prescribing doctor, ensuring intravenous-feeding formulas include biotin, and addressing alcohol use each let biotin status recover. Where the cause is a medication that cannot be changed, supplemental biotin can offset the depletion under medical guidance.
- Oral biotin supplements for acquired deficiency. When a true deficiency is confirmed, modest oral biotin doses correct it reliably, and the visible signs — rash, hair, nails — improve over weeks to months as the affected tissues regrow. Skin changes tend to respond fastest; hair and nails take longer simply because they grow slowly.
- Lifelong, higher-dose biotin for inherited forms. Biotinidase and holocarboxylase synthetase deficiencies are treated with pharmacological doses of biotin for life. This treatment is dramatically effective and inexpensive when started early — another reason newborn screening matters so much. Sweetman's classic review of inheritable, biotin-treatable disorders helped establish this approach.
For most acquired cases, the outlook is excellent: correct the shortage, fix the cause, and the skin, hair, and nail changes reverse. The key is making the correct diagnosis in the first place — which brings us to a widespread misunderstanding worth addressing head-on.
The Hair-and-Nail Supplement Myth
Biotin is marketed heavily for thicker hair, stronger nails, and clearer skin, and these products are enormously popular. It is important to be honest about what the science actually shows: biotin supplements help hair, skin, and nails only in people who are genuinely deficient. In people whose biotin levels are already normal — which is the vast majority — there is no good evidence that extra biotin grows hair, thickens nails, or improves skin.
The reasoning is straightforward. Biotin's beauty-related benefits come from correcting a shortage; once the body has enough, adding more does not push the relevant enzymes to work harder, because they are already fully supplied. Reviews of the published studies make this clear. Lipner's well-known analysis in the Journal of the American Academy of Dermatology found that nearly all the positive reports of biotin improving hair or nails involved people with an underlying deficiency or a specific inherited condition — not healthy adults seeking cosmetic gains. Trüeb, writing on the use of biotin for hair loss, reached the same cautionary conclusion: routine biotin for hair loss in non-deficient people is not supported by solid evidence.
This matters for two practical reasons. First, money and false hope: people spend on high-dose biotin expecting cosmetic results that, for the non-deficient, are unlikely to materialize. Second — and more importantly — those high doses can distort common blood tests (as covered in the Diagnosis section), occasionally leading to misdiagnosis of thyroid or other conditions. Because biotin is water-soluble and excess is largely excreted in urine, it does not build up to a classic poisoning the way fat-soluble vitamins can; the real-world harm is mainly this laboratory interference. The honest bottom line: if you suspect a deficiency, get it evaluated and treat the cause; if you simply want better hair or nails and are well-nourished, biotin is unlikely to be the answer. For more on the safety side, see the Vitamin B7 Toxicity hub, and for a deeper look at the cosmetic evidence see Biotin and Hair, Skin, and Nail Health.
When to Seek Care / Red Flags
Most adult biotin-related concerns are not emergencies, and the right step for gradual hair thinning, brittle nails, or a mild rash is a routine appointment to look for the many more common explanations first. However, certain situations do warrant prompt or urgent medical attention:
- A sick infant or a positive newborn screen. This is the true emergency in the biotin world. Seizures, unusual floppiness or stiffness, poor feeding, breathing trouble, a worsening rash, or hair loss in a young infant — especially if newborn screening flagged biotinidase deficiency — needs immediate medical evaluation, because early treatment prevents permanent harm.
- A spreading scaly rash with hair loss in someone with a clear risk factor. If you are on long-term anti-seizure medicine, have been living on raw egg whites, or are on intravenous nutrition, and you develop the classic combination of a periorificial rash, shedding hair, and brittle nails, see your doctor promptly so biotin status can be checked and corrected.
- New neurological symptoms. Persistent deep fatigue, new or worsening depression, or tingling and numbness in the hands and feet should be evaluated — not because biotin is the likely cause (it usually is not), but because these symptoms have important causes that need to be sorted out.
- Before blood tests, if you take biotin. This is a safety flag rather than a symptom: always tell your clinician and the lab that you take biotin supplements, because high doses can falsify thyroid, hormone, vitamin D, and cardiac (troponin) test results. You may be asked to pause it for a few days first.
In short: in adults, isolated cosmetic symptoms rarely signal an emergency, but the combination of the classic rash, hair loss, and a known risk factor — and anything neurological in an infant — deserves timely medical care. For related skin and hair conditions, see Alopecia and Hair Loss (symptom overview).
Key Research Papers
- Said HM (2012). Biotin: Biochemical, Physiological and Clinical Aspects. Subcellular Biochemistry;56:1-19. — DOI: 10.1007/978-94-007-2199-9_1
- Lardy HA, Peanasky R (1953). Metabolic Functions of Biotin. Physiological Reviews;33(4):560-565. — DOI: 10.1152/physrev.1953.33.4.560
- Scott D (1958). Clinical Biotin Deficiency ("Egg White Injury"). Acta Medica Scandinavica;162(1):69-70. — DOI: 10.1111/j.0954-6820.1958.tb01753.x
- Sweetman L, Nyhan WL (1986). Inheritable Biotin-Treatable Disorders and Associated Phenomena. Annual Review of Nutrition;6(1):317-343. — DOI: 10.1146/annurev.nutr.6.1.317
- Wolf B (2015). The Story of Biotinidase Deficiency and Its Introduction into Newborn Screening. International Journal of Neonatal Screening;1(1):3-12. — DOI: 10.3390/ijns1010003
- Seymons K, De Moor A, De Raeve H, Lambert J (2004). Dermatologic Signs of Biotin Deficiency Leading to the Diagnosis of Multiple Carboxylase Deficiency. Pediatric Dermatology;21(3):231-235. — DOI: 10.1111/j.0736-8046.2004.21308.x
- Mock DM, Quirk JG, Mock NI (2002). Marginal biotin deficiency during normal pregnancy. The American Journal of Clinical Nutrition;75(2):295-299. — DOI: 10.1093/ajcn/75.2.295
- Mock DM, Stadler DD, Stratton SL, Mock NI (2009). Marginal Biotin Deficiency is Common in Normal Human Pregnancy and Is Highly Teratogenic in Mice. The Journal of Nutrition;139(1):154-157. — DOI: 10.3945/jn.108.095273
- Mock DM (2005). Marginal biotin deficiency is teratogenic in mice and perhaps humans: a review. The Journal of Nutritional Biochemistry;16(7):435-437. — DOI: 10.1016/j.jnutbio.2005.03.022
- Lipner SR, Scher RK (2018). Rethinking biotin therapy for hair, nail, and skin disorders. Journal of the American Academy of Dermatology;78(6):1236-1238. — DOI: 10.1016/j.jaad.2018.02.018
- Trüeb RM (2018). Comment on the Use of Biotin for Hair Loss. Skin Appendage Disorders;4(4):345-346. — DOI: 10.1159/000484489
- Avery G (2019). Biotin interference in immunoassay: a review for the laboratory scientist. Annals of Clinical Biochemistry;56(4):424-430. — DOI: 10.1177/0004563219842231
PubMed Topic Searches
- PubMed — Biotin deficiency: symptoms and diagnosis
- PubMed — Biotinidase deficiency and newborn screening
- PubMed — Avidin, raw egg white, and biotin deficiency
- PubMed — Biotin supplements for hair and nails: evidence
- PubMed — Anticonvulsants and biotin status
Connections
- Biotin Deficiency: Hair Loss
- Biotin Deficiency: Skin Rashes
- Biotin Deficiency: Brittle Nails
- Biotin Deficiency: Neurological Symptoms
- Vitamin B7 (Biotin) Overview
- Vitamin B7 Toxicity
- Vitamin B7 Benefits Hub
- Biotin and Hair, Skin, and Nail Health
- Biotin and Blood Sugar
- Comprehensive Metabolic Panel
- Complete Blood Count
- Alopecia
- Hair Loss (Symptom Overview)
- Eggs
- Salmon
- Beef