Vitamin B3 (Niacin) — Benefits Deep Dive
Vitamin B3 is unusual among nutrients because it is the obligate biochemical precursor to NAD+ and NADP+ — two coenzymes that together participate in more than 500 enzymatic reactions, more than any other vitamin-derived cofactor. That single fact explains why niacin shows up across four utterly different clinical domains: anti-aging NAD+ restoration, lipid management for cardiovascular prevention, classical deficiency dermatology, and orthomolecular psychiatry. Each benefit page below explores one of those four worlds in clinical-trial depth.
Deep-Dive Articles
NAD+ Precursor — Why All Roads Lead to NAD+
The four niacin family members — nicotinic acid, nicotinamide (NAM), nicotinamide riboside (NR), and nicotinamide mononucleotide (NMN) — all converge on NAD+ through three distinct biosynthetic routes: the Preiss-Handler pathway (nicotinic acid), the salvage pathway (NAM and NR via NRK enzymes), and the de novo kynurenine pathway from tryptophan. This page maps every route, compares cost-effectiveness of plain niacin/NAM against expensive NR/NMN supplements, and tackles the flush-vs-flush-free decision.
Cholesterol & Cardiovascular Disease
Niacin was the first lipid-modifying drug ever shown to reduce all-cause mortality — the 1975 Coronary Drug Project. AIM-HIGH (2011) and HPS2-THRIVE (2014) were negative when niacin was added on top of statins, leading mainstream cardiology to abandon it. This page walks the trial history honestly, explains why niacin still has a real place as monotherapy in statin-intolerant patients with high Lp(a) and ApoB, and gives the 1-3 g/day immediate-release titration protocol that works.
Pellagra & Skin Health
The classical deficiency story — the US South pellagra epidemic, Joseph Goldberger's brilliant epidemiology, the "4 Ds" of dermatitis-diarrhea-dementia-death, and why corn-based diets without nixtamalization caused the catastrophe. Then the modern skin chapter: hidden pellagra in chronic alcoholism, Crohn's, and Hartnup disease, plus topical niacinamide for acne, hyperpigmentation, barrier function, and the landmark ONTRAC trial showing 23% reduction in non-melanoma skin cancer.
Schizophrenia & Orthomolecular Psychiatry
Abram Hoffer's 1950s niacin trials in schizophrenia inaugurated orthomolecular psychiatry. Linus Pauling gave the field its name and intellectual scaffolding. The niacin flush test (reduced or absent flush response in a subset of schizophrenia patients) remains a fascinating biomarker. This page covers the original positive trials, why later controlled trials disappointed, the genuine pellagra-psychosis link, and the realistic place of high-dose B3 in OCD, anxiety, and depression today.
Table of Contents
- Deep-Dive Articles
- Why Niacin Produces Effects Across So Many Conditions
- The Four Forms of Vitamin B3 Compared
- Research Papers: NAD+ Metabolism & Longevity
- Research Papers: Cholesterol & Cardiovascular
- Research Papers: Pellagra, Skin & Dermatology
- Research Papers: Psychiatry & Mental Health
- Research Papers: Cross-Cutting (Forms, Safety, Mechanism)
- External Authoritative Resources
- Connections
- Featured Videos
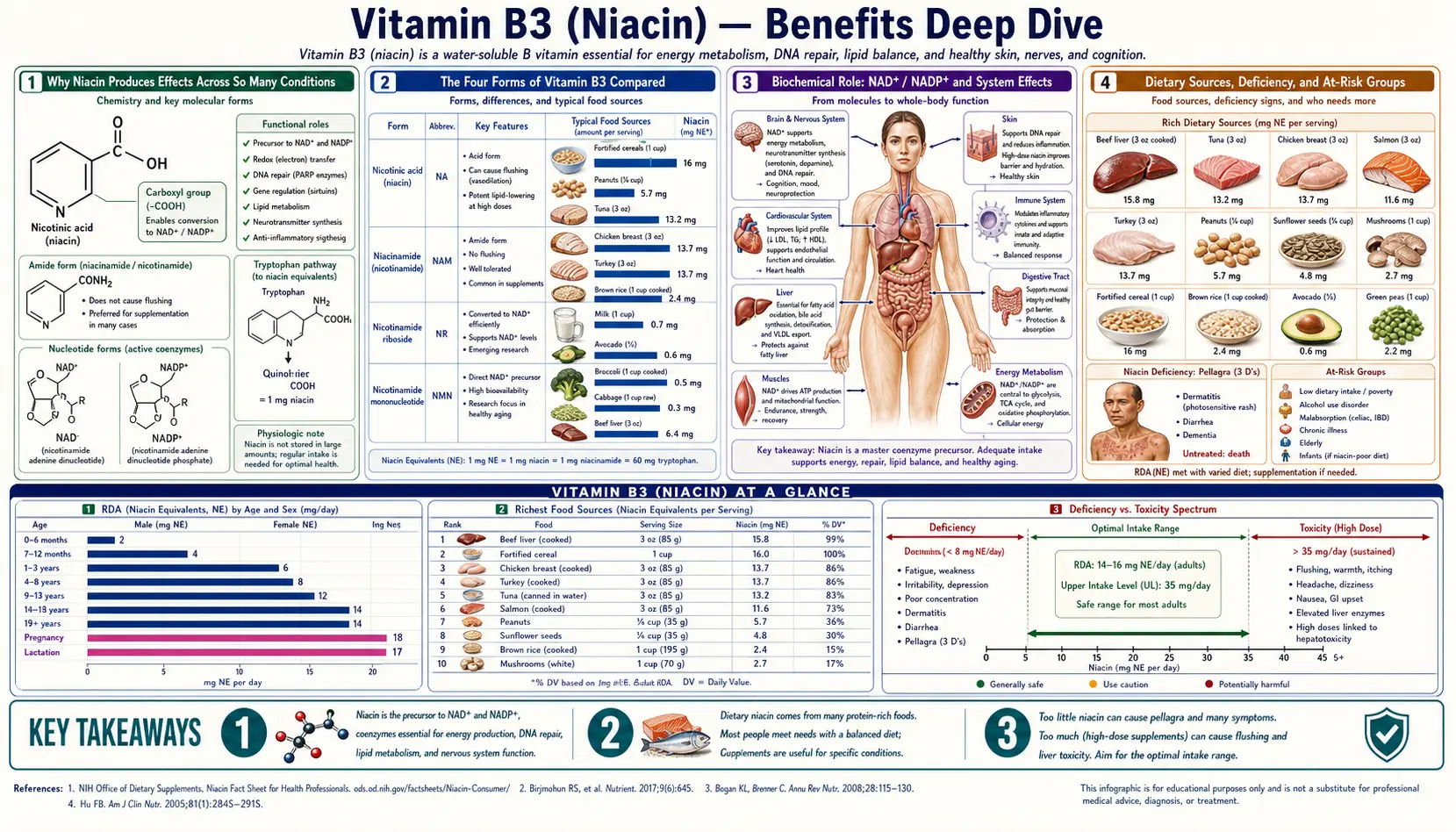
Why Niacin Produces Effects Across So Many Conditions
Most vitamins are essential cofactors for a small number of specific enzymes — vitamin C for collagen hydroxylase, biotin for the four carboxylases, vitamin K for the gamma-glutamyl carboxylase. Vitamin B3 is different. Its two derived coenzymes — NAD+ and NADP+ — participate in more than 500 enzymatic reactions, more than any other vitamin-derived molecule. That extraordinary breadth maps to four distinct clinical domains, each addressed in its own deep-dive page:
- Universal energy currency & longevity substrate — NAD+ accepts electrons in glycolysis, beta-oxidation, the pyruvate dehydrogenase complex, and three of the eight Krebs cycle steps, then delivers them to Complex I of the electron transport chain. Beyond electron carriage, NAD+ is the obligate substrate for the seven sirtuins (longevity enzymes), 17 PARPs (DNA repair), and CD38 (immune signaling) — all of which consume NAD+ rather than recycling it. NAD+ levels drop roughly 50% between ages 40 and 60 in many tissues, and restoring them is the central premise of the NAD+ precursor story.
- Pharmacological lipid-modifying drug — at gram-range doses (1-3 g/day), nicotinic acid acts as a true pharmacological agent, not just a vitamin. It is the most effective single agent ever discovered for raising HDL (by 15-35%), and uniquely among readily available compounds it meaningfully lowers Lp(a) by up to 30%. This is the basis of the cardiovascular indication, anchored by the 1975 Coronary Drug Project trial.
- The deficiency disease that defined the vitamin — niacin's discovery came from the pellagra epidemic in the US South (1900-1940), an enormous public-health catastrophe driven by corn-based diets lacking nixtamalization. The "4 Ds" of pellagra — dermatitis, diarrhea, dementia, death — remain a teaching paradigm in nutritional medicine, and modern hidden pellagra still appears in alcoholics, Crohn's patients, and Hartnup disease (see Pellagra & Skin).
- Orthomolecular psychiatry — Abram Hoffer and Humphry Osmond's 1950s Saskatchewan niacin trials in schizophrenia were the founding work of what Linus Pauling later named "orthomolecular psychiatry." The niacin flush test (reduced or absent flush response in roughly 40% of schizophrenia patients) remains a fascinating endophenotype marker. The clinical evidence is mixed but the biochemistry is real — see Schizophrenia & Mental Health.
Beyond these four primary domains, B3 contributes to multiple supporting roles: the NADPH-glutathione recycling axis that powers Phase II detoxification, joint-mobility research dating back to William Kaufman's 1940s nicotinamide protocols for osteoarthritis, GPR109A receptor signaling that links niacin to ketosis and inflammation, and beta-cell protection in early type 1 diabetes (the ENDIT trial). The unifying thread is always NAD+ availability — whenever a clinical effect of B3 surprises a researcher, the explanation traces back to one of the 500+ NAD/NADP-dependent reactions.
The Four Forms of Vitamin B3 Compared
| Form | Raises NAD+? | Lipid Effects? | Flush? | Best For |
|---|---|---|---|---|
| Nicotinic Acid (Niacin) | Yes (Preiss-Handler) | Yes — HDL, LDL, TG, Lp(a) | Yes | Lipid management; statin intolerance |
| Nicotinamide (NAM) | Yes (salvage) | No | No | Skin cancer prevention; arthritis; pellagra treatment |
| Nicotinamide Riboside (NR) | Yes (NRK salvage) | No | No | Anti-aging; mitochondrial support |
| Nicotinamide Mononucleotide (NMN) | Yes (one step from NAD+) | No | No | Anti-aging (David Sinclair work) |
The cost differential is dramatic. Plain nicotinamide is about $0.05 per gram. Nicotinic acid is about $0.10 per gram. Nicotinamide riboside (Niagen, TRU NIAGEN) runs roughly $1-2 per gram — about 20-40x the cost. NMN is similar or more expensive. For raw NAD+ raising, plain NAM is the cost-effective option; NR/NMN gain ground only if the higher-end mitochondrial and tissue-distribution claims for them prove durable in long-term human trials.
Research Papers: NAD+ Metabolism & Longevity
- Preiss J, Handler P (1958). Biosynthesis of diphosphopyridine nucleotide from nicotinic acid. J Biol Chem. — PubMed: Preiss-Handler pathway 1958
- Bieganowski P, Brenner C (2004). Discoveries of nicotinamide riboside as a nutrient and conserved NRK genes establish a Preiss-Handler independent route to NAD+. Cell. — PubMed: NR discovery Brenner 2004
- Yoshino J et al. (2018). NAD+ intermediates: the biology and therapeutic potential of NMN and NR. Cell Metabolism. — PubMed: Yoshino NMN/NR review
- Trammell SA et al. (2016). Nicotinamide riboside is uniquely and orally bioavailable in mice and humans. Nature Communications. — PubMed: Trammell NR human PK
- Martens CR et al. (2018). Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nature Communications. — PubMed: Martens NR human trial
- Mills KF et al. (2016). Long-term administration of nicotinamide mononucleotide mitigates age-associated physiological decline in mice. Cell Metabolism. — PubMed: Mills NMN mice 2016
- Yoshino J, Mills KF, Imai S et al. (2011). Nicotinamide mononucleotide, a key NAD+ intermediate, treats the pathophysiology of diet- and age-induced diabetes in mice. Cell Metabolism. — PubMed: NMN diabetes mice
- Imai S, Guarente L (2014). NAD+ and sirtuins in aging and disease. Trends Cell Biol. — PubMed: Imai-Guarente review
- Camacho-Pereira J et al. (2016). CD38 dictates age-related NAD decline. Cell Metabolism. — PubMed: CD38 NAD decline
- Verdin E (2015). NAD+ in aging, metabolism, and neurodegeneration. Science. — PubMed: Verdin NAD review Science
- Sinclair DA et al. (2018). Why NAD+ declines during aging: it's destroyed. Cell Metabolism. — PubMed: Sinclair NAD destruction
Research Papers: Cholesterol & Cardiovascular
- Coronary Drug Project Research Group (1975). Clofibrate and niacin in coronary heart disease. JAMA. — PubMed: CDP 1975 niacin
- Canner PL et al. (1986). Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacin. JACC. — PubMed: CDP 15-year follow-up
- AIM-HIGH Investigators (2011). Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. NEJM. — PubMed: AIM-HIGH 2011
- HPS2-THRIVE Collaborative Group (2014). Effects of extended-release niacin with laropiprant in high-risk patients. NEJM. — PubMed: HPS2-THRIVE 2014
- Carlson LA (2005). Nicotinic acid: the broad-spectrum lipid drug — a 50th anniversary review. J Intern Med. — PubMed: Carlson 50-year niacin review
- Carlson LA, Rosenhamer G (1988). Reduction of mortality in the Stockholm Ischaemic Heart Disease Secondary Prevention Study by combined treatment with clofibrate and nicotinic acid. Acta Med Scand. — PubMed: Stockholm IHD study
- Boden WE et al. (2014). Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy — AIM-HIGH author rebuttal. NEJM. — PubMed: Boden AIM-HIGH discussion
- Ginsberg HN et al. on niacin Lp(a) reduction — PubMed: niacin Lp(a) reduction
- Bruckert E et al. (2010). Meta-analysis of the effect of nicotinic acid alone or in combination on cardiovascular events and atherosclerosis. Atherosclerosis. — PubMed: Bruckert niacin meta-analysis
- McKenney JM et al. (1994). A comparison of the efficacy and toxic effects of sustained- vs immediate-release niacin in hypercholesterolemic patients. JAMA. — PubMed: McKenney IR vs SR niacin
Research Papers: Pellagra, Skin & Dermatology
- Goldberger J et al. (1923). A study of the relation of diet to pellagra incidence in seven textile-mill communities of South Carolina. Public Health Reports. — PubMed: Goldberger pellagra epidemiology
- Chen AC et al. (2015). A phase 3 randomized trial of nicotinamide for skin-cancer chemoprevention (ONTRAC). NEJM. — PubMed: ONTRAC 2015
- Hegyi J et al. (2004). Pellagra: dermatitis, dementia, and diarrhea. Int J Dermatol. — PubMed: pellagra clinical review
- Hartnup disease and niacin — PubMed: Hartnup disease niacin
- Topical niacinamide for acne — PubMed: topical niacinamide acne
- Niacinamide and skin barrier function — PubMed: niacinamide barrier function
- Niacinamide and hyperpigmentation — PubMed: niacinamide hyperpigmentation
- Crohn's disease and secondary pellagra — PubMed: Crohn's pellagra
- Alcoholism and pellagra — PubMed: alcoholism pellagra
- Carcinoid syndrome and secondary pellagra — PubMed: carcinoid pellagra
Research Papers: Psychiatry & Mental Health
- Hoffer A, Osmond H, Smythies J (1954). Schizophrenia: a new approach. II. Result of a year's research. J Ment Sci. — PubMed: Hoffer-Osmond 1954 schizophrenia
- Hoffer A (1971). Megavitamin B-3 therapy for schizophrenia. Can Psychiatr Assoc J. — PubMed: Hoffer megavitamin B3
- Pauling L (1968). Orthomolecular psychiatry. Science. — PubMed: Pauling orthomolecular 1968
- Niacin flush test in schizophrenia — PubMed: niacin flush schizophrenia
- APA Task Force (1973). Megavitamin and orthomolecular therapy in psychiatry. American Psychiatric Association. — PubMed: APA task force 1973
- Niacin and OCD — PubMed: niacin OCD
- Niacinamide and anxiety / benzodiazepine receptor — PubMed: niacinamide anxiety
- Tryptophan-kynurenine pathway and depression — PubMed: kynurenine depression
- Quinolinic acid and neuropsychiatric disease — PubMed: quinolinic acid psychiatry
- Niacin and Alzheimer's disease (epidemiology) — PubMed: niacin Alzheimer's
Research Papers: Cross-Cutting (Forms, Safety, Mechanism)
- Linus Pauling Institute — Niacin Micronutrient Information Center (current edition) — LPI Niacin MIC
- Knip M et al. (2000). Safety of high-dose nicotinamide: a review (ENDIT trial safety arm). Diabetologia. — PubMed: Knip nicotinamide safety
- Henderson LM (1983). Niacin (review of biochemistry, metabolism, requirements). Annu Rev Nutr. — PubMed: Henderson niacin review
- Sustained-release niacin hepatotoxicity — PubMed: SR niacin hepatotoxicity
- GPR109A receptor and niacin signaling — PubMed: GPR109A receptor
- Kynurenine pathway and quinolinic acid — PubMed: kynurenine pathway
- Inositol hexanicotinate ("no-flush niacin") bioavailability — PubMed: inositol hexanicotinate
- Kaufman W (1949). Common forms of niacinamide deficiency disease (osteoarthritis). Yale University Press. — PubMed: Kaufman niacinamide
- ENDIT — European Nicotinamide Diabetes Intervention Trial — PubMed: ENDIT trial
- NAD+ measurement and quantification methods — PubMed: NAD+ measurement methods
External Authoritative Resources
- Linus Pauling Institute — Niacin Micronutrient Information Center — the single most authoritative scientific summary of niacin biology and clinical evidence, regularly updated
- NIH Office of Dietary Supplements — Niacin Fact Sheet for Health Professionals
- MedlinePlus — Niacin and Niacinamide
- PubMed — All research on niacin/NAD (~100,000+ papers as of 2026)
Connections
- Vitamin B3 (Main Page)
- B3 as NAD+ Precursor
- B3 for Cholesterol & Cardiovascular
- B3 for Pellagra & Skin
- B3 for Schizophrenia & Mental Health
- Pellagra & Niacin Deficiency
- Niacin & Cholesterol
- Niacin in Gerson Therapy
- NAD+ / NMN
- Glutathione
- Tryptophan
- Cardiovascular Disease
- Cholesterol Management
- Schizophrenia
- OCD
- Depression
- Vitamin B2 (Riboflavin)
- Vitamin B6 (Pyridoxine)
- Lipid Panel
- All Vitamins