Vitamin B3 as an NAD+ Precursor — Why All Roads Lead to NAD+
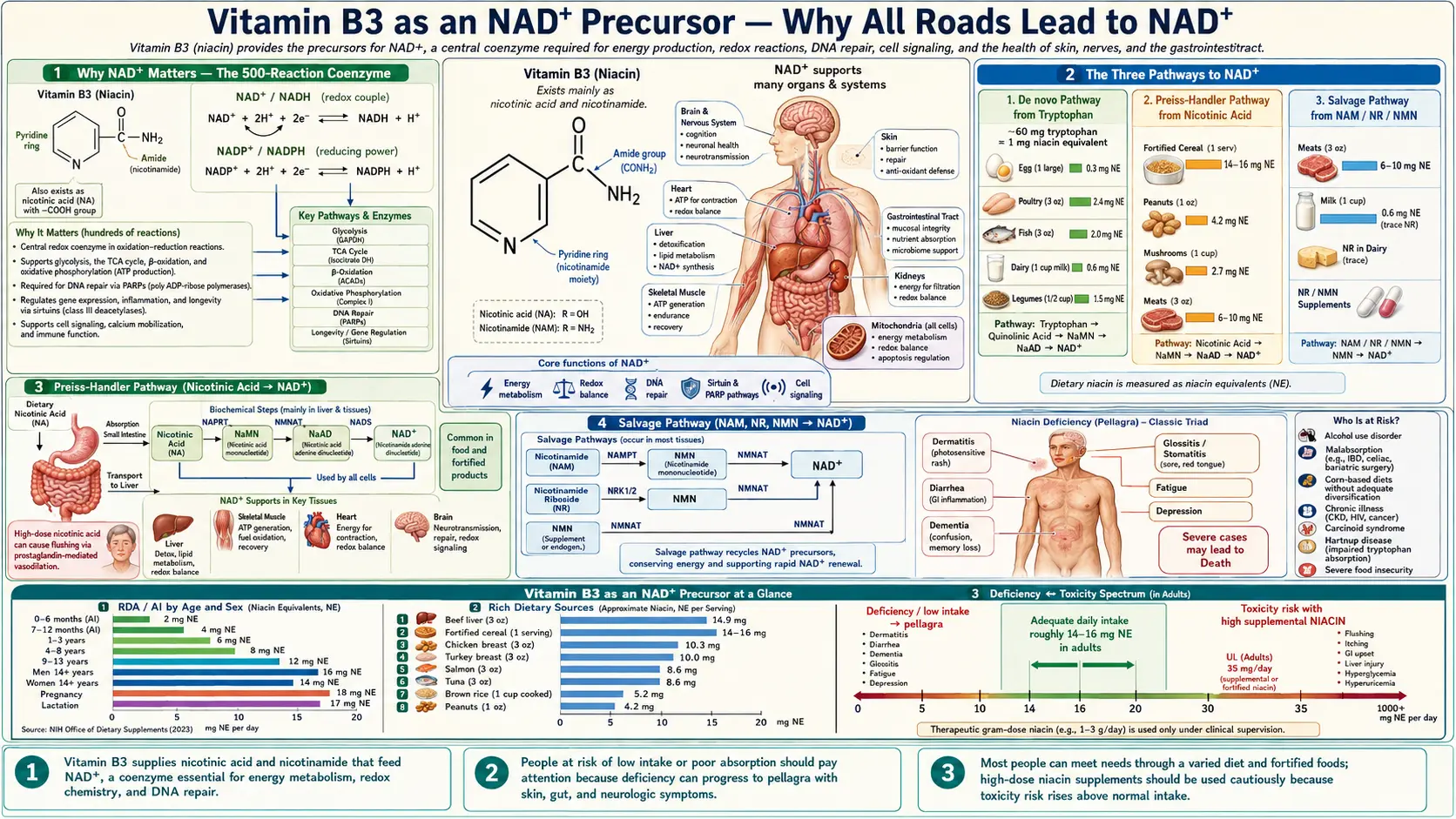
Niacin (nicotinic acid), nicotinamide (NAM), nicotinamide riboside (NR), nicotinamide mononucleotide (NMN), and even the amino acid tryptophan all converge on the same destination — nicotinamide adenine dinucleotide, NAD+. Three biosynthetic routes carry them there: the Preiss-Handler pathway (nicotinic acid), the salvage pathway (NAM, NR, NMN via NAMPT and NRK enzymes), and the de novo kynurenine pathway from tryptophan. Because all four B3 family members reach NAD+ within a few enzymatic steps, the cost-effective NAD+ supplementation question becomes a pharmacology question, not a metaphysical one: which precursor reaches which tissue at which dose, and at what cost.
Table of Contents
- Why NAD+ Matters — The 500-Reaction Coenzyme
- The Three Pathways to NAD+
- Preiss-Handler Pathway (Nicotinic Acid → NAD+)
- Salvage Pathway (NAM, NR, NMN → NAD+)
- De Novo Pathway (Tryptophan → NAD+)
- NR/NMN vs Plain Niacin/NAM — The Cost-Effectiveness Question
- Flush vs Flush-Free — The Practical Choice
- NAD+ Decline With Aging
- Practical Dosing Protocols
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Why NAD+ Matters — The 500-Reaction Coenzyme
NAD+ is the most-used coenzyme in human biology. It participates in more than 500 distinct enzymatic reactions, dwarfing every other vitamin-derived cofactor. Three broad categories of NAD+-dependent reactions explain its centrality:
- Redox reactions (electron carrier). NAD+ accepts a pair of electrons (becoming NADH) during glycolysis at glyceraldehyde-3-phosphate dehydrogenase, during the pyruvate dehydrogenase complex, during three of the eight Krebs cycle reactions (isocitrate dehydrogenase, α-ketoglutarate dehydrogenase, malate dehydrogenase), and during every round of fatty-acid beta-oxidation. NADH then donates those electrons to Complex I of the mitochondrial electron transport chain, driving roughly 2.5 ATP per molecule. Without NAD+, oxidative metabolism halts within seconds.
- Substrate for NAD+-consuming enzymes. The seven sirtuins (SIRT1-SIRT7), the 17 PARPs (poly-ADP-ribose polymerases), and CD38 all use NAD+ as a substrate rather than a recyclable cofactor — they cleave NAD+ into nicotinamide plus an ADP-ribose moiety used for protein modification. Sirtuin deacetylation, PARP-mediated DNA repair, and CD38-mediated cyclic-ADP-ribose signaling all literally consume NAD+. The cell must continuously resynthesize NAD+ from precursors to keep up.
- NADPH (anabolic reductant). NAD+ kinase phosphorylates NAD+ to NADP+, the precursor of NADPH. NADPH drives reductive biosynthesis (fatty acids, cholesterol, steroid hormones), regenerates oxidized glutathione (GSSG → GSH) via glutathione reductase, powers cytochrome P450 Phase I detoxification, and supplies electrons to NADPH oxidase in phagocytes for the oxidative burst. Without NADPH, the entire antioxidant defense system collapses.
This breadth means that NAD+ supply is rate-limiting for energy metabolism, longevity signaling, DNA repair, and antioxidant defense simultaneously. Even modest reductions in NAD+ availability create metabolic bottlenecks felt as fatigue, slowed recovery, accelerated aging signatures, and impaired detoxification.
The Three Pathways to NAD+
Mammals build NAD+ from three different starting molecules through three distinct enzymatic routes. Knowing them is the key to choosing a supplement intelligently.
| Pathway | Starting Molecule | Key Enzymes | Steps to NAD+ |
|---|---|---|---|
| Preiss-Handler | Nicotinic acid (NA) | NAPRT → NMNAT → NADS | 3 enzymatic steps |
| Salvage (NAM) | Nicotinamide (NAM) | NAMPT → NMNAT | 2 enzymatic steps |
| Salvage (NR) | Nicotinamide riboside (NR) | NRK1/NRK2 → NMNAT | 2 enzymatic steps |
| Salvage (NMN) | Nicotinamide mononucleotide (NMN) | NMNAT (or de-phosphorylated to NR first) | 1 enzymatic step |
| De Novo (kynurenine) | Tryptophan | TDO/IDO → 5+ enzymes → QPRT | 8 enzymatic steps |
Every precursor reaches the same destination — NAD+ — but the kinetics, tissue distribution, and side-effect profile differ. The salvage pathway dominates day-to-day NAD+ maintenance because sirtuins, PARPs, and CD38 continuously release NAM as they consume NAD+, and the cell salvages that NAM back to NMN and then NAD+ via NAMPT (the rate-limiting enzyme of the salvage pathway).
Preiss-Handler Pathway (Nicotinic Acid → NAD+)
Described by Jack Preiss and Philip Handler in their 1958 Journal of Biological Chemistry papers, this is the route that nicotinic acid (the "niacin" of pellagra rescue and lipid-lowering therapy) takes to NAD+:
- Step 1: Nicotinic acid + PRPP (5-phosphoribosyl-1-pyrophosphate) → nicotinic acid mononucleotide (NaMN). Catalyzed by NAPRT (nicotinate phosphoribosyltransferase).
- Step 2: NaMN + ATP → nicotinic acid adenine dinucleotide (NaAD). Catalyzed by NMNAT (nicotinamide mononucleotide adenylyltransferase, three isoforms NMNAT1/2/3 with different subcellular localizations).
- Step 3: NaAD + glutamine + ATP → NAD+ + glutamate. Catalyzed by NADS (NAD synthase). This is the amidation step that converts the carboxylic acid (nicotinic) to the amide (nicotinamide) form.
The Preiss-Handler pathway is highly active in the liver and adipose tissue, which is why orally administered nicotinic acid produces such powerful systemic effects on lipid metabolism, despite the gut and liver removing most of the nicotinic acid on first pass.
Salvage Pathway (NAM, NR, NMN → NAD+)
The salvage pathway is the workhorse of cellular NAD+ maintenance. It exists primarily to recycle the nicotinamide (NAM) released by sirtuins, PARPs, and CD38 back into fresh NAD+ — but the same enzymes accept dietary NAM, NR, and NMN.
NAM route
- Step 1: NAM + PRPP → NMN. Catalyzed by NAMPT (nicotinamide phosphoribosyltransferase) — the rate-limiting enzyme of the salvage pathway.
- Step 2: NMN + ATP → NAD+. Catalyzed by NMNAT.
NR route (described by Charles Brenner, 2004)
- Step 1: NR + ATP → NMN. Catalyzed by NRK1 or NRK2 (nicotinamide riboside kinases). NRK1 is ubiquitous; NRK2 is enriched in skeletal muscle, heart, and brain.
- Step 2: NMN + ATP → NAD+. Catalyzed by NMNAT, the same enzyme as the NAM route.
NMN route
- Direct: NMN + ATP → NAD+. Catalyzed by NMNAT — one step from NAD+.
- Caveat: Orally administered NMN is rapidly de-phosphorylated by intestinal CD73 to NR, then taken up across the enterocyte membrane, then re-phosphorylated to NMN intracellularly. So although NMN is "closer" to NAD+ on paper, it enters cells largely through the NR route. This is why some pharmacologists argue NR and NMN are functionally equivalent for oral supplementation.
NAMPT, the rate-limiting NAM-salvage enzyme, is itself regulated by circadian clock genes and declines with age — one mechanism behind age-related NAD+ depletion. NR and NMN bypass NAMPT, which is part of why they may raise NAD+ more effectively than equivalent NAM doses in older tissues.
De Novo Pathway (Tryptophan → NAD+)
The de novo or "kynurenine" pathway builds NAD+ from scratch starting with the essential amino acid tryptophan:
- Tryptophan → N-formylkynurenine (by TDO in liver, IDO in inflammation/extrahepatic tissue)
- N-formylkynurenine → kynurenine
- Kynurenine → 3-hydroxykynurenine (requires vitamin B2/FAD as cofactor for kynurenine 3-monooxygenase)
- 3-hydroxykynurenine → 3-hydroxyanthranilic acid (requires vitamin B6/PLP for kynureninase)
- 3-hydroxyanthranilic acid → 2-amino-3-carboxymuconate-semialdehyde → quinolinic acid
- Quinolinic acid + PRPP → NaMN. Catalyzed by QPRT (quinolinate phosphoribosyltransferase).
- NaMN then enters the Preiss-Handler pathway and proceeds through NMNAT and NADS to NAD+.
The conversion ratio is approximately 60 mg of tryptophan per 1 mg of niacin equivalent (NE). So a steak with 1.5 g of dietary tryptophan provides about 25 mg NE on top of its preformed niacin content. This is why diets adequate in animal protein rarely cause pellagra even if preformed niacin is low.
The vitamin-cofactor catch: the de novo pathway requires B2, B6, and iron as cofactors. Deficiency of any of these can functionally impair tryptophan-to-NAD+ conversion and cause secondary niacin insufficiency even with adequate dietary tryptophan. This is why isoniazid (which depletes B6) causes pellagra-like symptoms, and why patients with hyperemesis or refeeding-syndrome contexts need broad B-vitamin replacement, not just B1.
The quinolinic acid hazard: quinolinic acid is also a potent NMDA-receptor agonist and excitotoxin. In chronic inflammation (IDO induction), the kynurenine pathway diverts away from NAD+ production and toward neurotoxic quinolinic acid accumulation — implicated in depression, HIV-associated dementia, and neurodegeneration. See our Tryptophan page for the broader context.
NR/NMN vs Plain Niacin/NAM — The Cost-Effectiveness Question
Nicotinamide riboside (NR, sold as Niagen and TRU NIAGEN) and nicotinamide mononucleotide (NMN, popularized by David Sinclair's research at Harvard) have generated enormous enthusiasm as "next-generation" NAD+ precursors. The marketing claims they raise NAD+ more efficiently than plain niacin or NAM. Is it true?
What the human trials actually show
- Trammell et al. (2016, Nature Communications) — single-dose NR PK in healthy humans confirmed bioavailability and showed dose-dependent NAD+ increases in blood.
- Martens et al. (2018, Nature Communications) — chronic 1000 mg/day NR for 6 weeks in middle-aged/older adults raised blood NAD+ by ~60%, with no significant adverse effects.
- Plain nicotinamide at similar gram-range doses also robustly raises tissue NAD+. The Knip ENDIT-era safety data showed long-term gram-range NAM dosing was well-tolerated (though see Cautions for the sirtuin-inhibition concern).
- Head-to-head NR vs NAM in older adults at equivalent NAD+-raising doses are still relatively limited. The mechanistic advantage of NR/NMN is bypassing NAMPT (which declines with age), but the magnitude of clinical-outcome difference is not yet established.
The cost reality
| Form | Approximate Cost per Gram | Cost per Month at NAD+-raising dose |
|---|---|---|
| Plain nicotinamide (NAM) | $0.05-0.10 | $3-10 (at 500-1000 mg/day) |
| Nicotinic acid (immediate-release) | $0.10-0.20 | $5-20 |
| Nicotinamide riboside (NR) | $1-2 | $30-60 (at 250-500 mg/day) |
| Nicotinamide mononucleotide (NMN) | $1-3 | $30-90 |
For pure NAD+ raising in a budget-conscious patient, plain nicotinamide is the cost-effective choice — 20-40x cheaper than NR or NMN for an effect that, in published human trials, is in the same ballpark. NR and NMN make sense when (1) the patient can afford them, (2) age-related NAMPT decline is a specific concern, or (3) tissue-distribution differences matter for a specific indication (some animal data suggest NR reaches certain tissues more efficiently than NAM). For deeper comparison see NAD+ Precursors Compared on the NAD+/NMN page.
Flush vs Flush-Free — The Practical Choice
The prostaglandin-mediated niacin flush — a warm, tingling, red sensation of skin (face, neck, chest) starting 20-30 minutes after a 50+ mg dose of immediate-release nicotinic acid — is harmless but uncomfortable. It is the single most common reason patients abandon niacin therapy.
Who flushes
- Nicotinic acid at any dose above ~50 mg, particularly on an empty stomach, reliably flushes.
- Nicotinamide (NAM), NR, and NMN do NOT flush at any dose. Flushing is specific to the carboxylic-acid form that activates GPR109A on Langerhans cells in the skin.
- Tachyphylaxis develops with repeated dosing — the flush typically diminishes substantially within 1-2 weeks of consistent use.
Managing the flush when nicotinic acid is needed
- Start low and titrate: begin at 100 mg with the largest meal of the day; double every 5-7 days as tolerated.
- Aspirin pre-treatment: 325 mg aspirin 30 minutes before the niacin dose blocks the prostaglandin D2 release that drives the flush.
- Take with food: slows absorption and reduces peak flush intensity.
- Avoid alcohol and hot beverages around the dose — both potentiate the flush.
- Sustained-release (SR) caution: SR niacin causes much less flushing but carries substantially higher hepatotoxicity risk than immediate-release at equivalent doses (see Cautions).
When NAM/NR/NMN is the better choice
- The indication is NAD+ raising rather than lipid management — flush-free forms work just as well for NAD+.
- The patient has experienced significant flushing distress with nicotinic acid.
- The patient has a history of peptic ulcer disease — nicotinic acid can activate latent ulcers, NAM does not.
- The patient has active gout — nicotinic acid competes with uric acid for renal excretion, NAM does not.
"No-flush" niacin (inositol hexanicotinate) warning: this product is marketed as flush-free niacin but the inositol hexanicotinate complex releases very little free nicotinic acid in humans, and the lipid-modifying benefits of true nicotinic acid largely do not occur. If you want NAD+ raising without flush, use plain NAM; if you want the lipid benefits, you must accept some flushing.
NAD+ Decline With Aging
One of the most consistent findings in aging biology is that NAD+ levels decline substantially with age — roughly 50% between ages 40 and 60 in many tissues, with continued decline thereafter. Three mechanisms converge:
- NAMPT decline. The rate-limiting salvage-pathway enzyme falls with age in many tissues, reducing the cell's ability to recycle NAM back to NMN and NAD+. Both transcriptional decline and post-translational regulation contribute.
- CD38 rise. CD38, an NAD+-consuming ectoenzyme, increases dramatically in aged tissue — partly because tissue inflammation increases with age and CD38 is induced by inflammatory cytokines. The Camacho-Pereira et al. (2016, Cell Metabolism) work titled "CD38 dictates age-related NAD decline" made this case forcefully.
- PARP hyperactivation. Accumulated DNA damage with age chronically activates PARPs, which consume NAD+ at high rates during repair attempts. PARP1 alone can account for a substantial fraction of cellular NAD+ turnover in damaged tissue.
The clinical implication: older adults likely benefit more from NAD+ precursor supplementation than younger adults — not because young people don't need NAD+, but because young people's salvage and de novo pathways are working at full capacity already. In aged tissue, exogenous precursors can fill a gap that endogenous synthesis can no longer cover.
Practical Dosing Protocols
For NAD+ raising (anti-aging, mitochondrial support)
- Plain nicotinamide (NAM): 500-1000 mg/day, can split into 2 doses. Cheap, flush-free, effective. Cap at 3000 mg/day to avoid sirtuin product inhibition.
- Nicotinamide riboside (NR): 250-500 mg/day (typical Niagen/TRU NIAGEN dosing). Some users go to 1000 mg/day per the Martens 2018 trial.
- NMN: 250-1000 mg/day. Sublingual products dissolve in saliva for buccal absorption, which may bypass intestinal CD73 conversion to NR.
For lipid management (statin-intolerant or Lp(a)-elevated patients)
- Immediate-release nicotinic acid only. Sustained-release at gram-range doses carries unacceptable hepatotoxicity risk.
- Start 100 mg with the largest meal of the day. Titrate up by 100 mg every 5-7 days as the flush is tolerated. Target 1000-2000 mg/day, divided into 2-3 doses with meals.
- Aspirin 325 mg 30 minutes before each dose dramatically reduces flushing in the titration phase.
- Monitor liver enzymes (ALT, AST) at baseline, 3 months, 6 months, then annually. Monitor fasting glucose and uric acid.
- See Cholesterol & Cardiovascular for the full clinical protocol.
For pellagra treatment
- Nicotinamide 300-500 mg/day in divided doses (use NAM not nicotinic acid — flushing in a malnourished patient is undesirable).
- Improvement typically begins within 24-48 hours; full recovery over weeks if treated before neurological damage is established.
- Always co-administer broad B-complex including B1, B2, B6, B12, and folate — pellagra rarely occurs in isolation.
Cofactor stacking note: if you're taking gram-range NAM or NR/NMN for NAD+ raising, ensure adequate B2 (riboflavin, 10-25 mg/day) and B6 (pyridoxine or P5P, 25-50 mg/day) because they are cofactors for both the tryptophan-NAD+ pathway and the glutathione regeneration that NADPH drives.
Cautions
- HEPATOTOXICITY — sustained-release nicotinic acid at >1 g/day. This is the single most important safety issue. SR-niacin causes elevated transaminases, cholestatic jaundice, and in rare cases fulminant hepatic failure. The McKenney 1994 JAMA paper directly compared SR vs immediate-release at equivalent lipid-modifying doses and found dramatically higher hepatotoxicity in the SR arm. If you take gram-range niacin for lipid management, use immediate-release only. Even with IR-niacin, monitor ALT/AST at baseline, 3 months, 6 months, and annually thereafter. Discontinue if ALT exceeds 3x upper limit of normal.
- Hyperglycemia. Pharmacological-dose nicotinic acid (>1 g/day) raises fasting glucose by 5-10 mg/dL and HbA1c by 0.3-0.4 in many patients — via increased adipose lipolysis and free fatty acid release driving hepatic gluconeogenesis. In type 2 diabetes, monitor blood glucose closely after initiation and titration. NAM, NR, and NMN do not have this effect.
- Gout / hyperuricemia. Nicotinic acid competes with uric acid for renal tubular excretion, raising serum uric acid and potentially triggering gout flares. Avoid nicotinic acid in active gout; if needed, co-administer allopurinol or use NAM.
- Flush. Harmless but uncomfortable; see flush management section above.
- Peptic ulcer activation. Nicotinic acid increases gastric acid secretion and can reactivate latent peptic ulcers. Avoid in active PUD; use NAM if B3 is needed.
- Sirtuin product inhibition (high-dose NAM). At sustained doses above 3000 mg/day, NAM accumulates intracellularly and can inhibit sirtuins as a product-feedback inhibitor — the opposite of the desired longevity effect. Cap chronic NAM at ~2000 mg/day for NAD+ goals. NR and NMN do not have this concern because they raise NAD+ without generating excess NAM.
- Pregnancy. Niacin requirements rise modestly during pregnancy (RDA 18 mg NE). Pharmacological doses (gram-range nicotinic acid) are not established as safe in pregnancy — avoid unless specifically directed.
- Statin interaction. The AIM-HIGH and HPS2-THRIVE trials showed no incremental cardiovascular benefit from adding niacin to optimized statin therapy. Niacin's modern niche is largely in statin-intolerant patients with persistent dyslipidemia, not as add-on to statins.
Key Research Papers
- Preiss J, Handler P (1958). Biosynthesis of diphosphopyridine nucleotide from nicotinic acid. J Biol Chem. — PubMed
- Bieganowski P, Brenner C (2004). Discoveries of nicotinamide riboside as a nutrient and conserved NRK genes establish a Preiss-Handler independent route to NAD+. Cell. — PubMed
- Trammell SA et al. (2016). Nicotinamide riboside is uniquely and orally bioavailable in mice and humans. Nature Communications. — PubMed
- Martens CR et al. (2018). Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nature Communications. — PubMed
- Mills KF et al. (2016). Long-term administration of nicotinamide mononucleotide mitigates age-associated physiological decline in mice. Cell Metabolism. — PubMed
- Yoshino J et al. (2018). NAD+ intermediates: the biology and therapeutic potential of NMN and NR. Cell Metabolism. — PubMed
- Camacho-Pereira J et al. (2016). CD38 dictates age-related NAD decline. Cell Metabolism. — PubMed
- Imai S, Guarente L (2014). NAD+ and sirtuins in aging and disease. Trends Cell Biol. — PubMed
- Verdin E (2015). NAD+ in aging, metabolism, and neurodegeneration. Science. — PubMed
- Canto C et al. (2012). The NAD+ precursor nicotinamide riboside enhances oxidative metabolism and protects against high-fat diet-induced obesity. Cell Metabolism. — PubMed
- McKenney JM et al. (1994). A comparison of the efficacy and toxic effects of sustained- vs immediate-release niacin in hypercholesterolemic patients. JAMA. — PubMed
PubMed Topic Searches
- PubMed: NAD+ precursors NR NMN
- PubMed: Preiss-Handler pathway
- PubMed: NAMPT salvage pathway
- PubMed: NRK1/NRK2 enzymes
- PubMed: quinolinic acid QPRT
- PubMed: NAD+ decline aging
Connections
- Vitamin B3 Overview
- B3 Benefits Hub
- B3 for Cholesterol & Cardiovascular
- B3 for Pellagra & Skin
- B3 for Schizophrenia & Mental Health
- NAD+ / NMN
- Tryptophan
- Glutathione
- Vitamin B2 (Riboflavin)
- Vitamin B6 (Pyridoxine)
- Vitamin B1 (Thiamine)
- Cholesterol Management
- Niacin in Gerson Therapy
- Lipid Panel
- All Vitamins